Matched or nonmatched interventions based on the transtheoretical model to promote physical activity.A meta-analysis of randomized controlled trials
2018-04-26AhmedJermeRomainCatherineBortolonMathieuGourlanMarionCarayolEmmanuelleDeckerOlivierLareyreGrgoryNinotJulieBoichPaquitoBernard
Ahmed Jerôme Romain*,Catherine Bortolon,Mathieu Gourlan,Marion Carayol,Emmanuelle Decker,Olivier Lareyre,Grégory Ninot,Julie Boiché,Paquito Bernard,f,g,h
aEA4556 Laboratory Epsylon-Dynamics of Human Abilities and Health Behaviours,University of Montpellier,Montpellier 34000,France
bChallenge for the Change of Behaviour(CCB)Group,Montpellier 34000,France
cUniversity of Montreal Hospital Research Centre,Montreal,Quebec H2X 0A9,Canada
dUnit of Adult Psychiatry,La Colombière,University Hospital of Montpellier,Montpellier 34295,France
ePrevention Department of Institut Regional du Cancer de Montpellier,Epidaure,Montpellier 34298,France
fResearch Centre of the University Hospital of Quebec,Quebec G1R 2J6,Canada
gCancer Research Centre,University of Laval,Quebec G1R 3S3,Canada
hSchool of Psychology,University of Laval,Quebec G1C 0A6,Canada
1.Introduction
Over the past decades,physical activity(PA)was found to be low in most countries.1,2Future projections indicate a continuous decline,3along with an increasing prevalence of major noncommunicable diseases.4Numerous studies have been designed based on theoretical models to shed light on the processes generating significant changes in PA behavior.5Among them,the transtheoretical model6(TTM)has been widely used.
The TTM is a stage-based model of behavior change developed by Prochaska and DiClemente6based on the assumptions that(1)no single theory can account for the complexity of behavior change;(2)behavior change is a process that unfolds over time through several stages;(3)stages are stable and open to change;and(4)specific processes and principles of change should be used at specific stages to maximize the efficacy of behavior change.7In the TTM,each stage of change(SOC)describes the individual’s current intention and engagement toward a targeted health-related behavior.The stages are precontemplation(no intention to change the behavior),contemplation(individual starts to consider a possible behavior change),preparation(the individual is preparing to change),action(the individual is working on behavior change),and maintenance(the behavior change is consolidated).The TTM was initially developed for tobacco cessation6to understand how people change their behavior.However,given its success and efficacy in addictive behaviors,the TTM was further applied and extended to modify positive behaviors such as PA.8The TTM posits that there is no linearity in the evolution through the different stages,and that the progression or regression is influenced by its theoretical constructs,namely the decisional balance,temptation,self-efficacy,and processes of change(POCs).9Decisional balance is defined as a multidimensional set of values perceived as advantages and/or disadvantages associated with the decision to change a behavior.Temptation is described as an urge to engage in a specific habit in the midst of difficult situations.10Self-efficacy refers to the people’s judgments of their capabilities to organize and execute courses of action required to attain designated types of performances.11Finally,POCs are experiential and behavioral strategies that people use to change a given behavior.7
The efficacy of TTM intervention in promoting PA in adults has been assessed in 2 meta-analyses.First,Conn et al.12showed that TTM-based interventions had a small but significant effect on PA(d=0.15),but their conclusions remain limited owing to the inclusion of different study designs(e.g.,randomized trials,nonrandomized trials,controlled trials).Moreover,Conn et al.12did not define what a TTM-based intervention was(e.g.,to what extent the TTM was cited when the intervention was described)and did not consider the theoretical implementation(e.g.,to what extent the development and evaluation of the intervention are explicitly based on the TTM).13
More recently,Gourlan et al.5conducted a meta-analysis on the effects of theory-based interventions on PA promotion and further found an overall significant efficacy of TTM-based interventions with a medium effect size(d=0.31,95%confidence interval(CI):0.11-0.32).However,although those previous works have highlighted the efficacy of TTM-based interventions in promoting PA among adults,important issues remain to be resolved,notably concerning some of the characteristics(i.e.,moderators)associated with their efficacy.Indeed,both meta-analyses5,12have exhibited a high level of heterogeneity,with anI2equal to 64%12and 80%,5respectively,highlighting an important variability in individual studies’effect sizesaThe I2statistic quantifies the heterogeneity between collected studies and describes the proportion of variance in effect size due to heterogeneity.I2 between 0%and 30%is considered a not important heterogeneity,between 30%and 60%is moderate,between 50%and 90%is substantial,and 75%to 100%is considerable heterogeneity.49and indicating the necessity to further explore the sources of heterogeneity.
The exploration of the moderators associated with the efficacy of TTM-based intervention is an important issue because this model has the particularity to offer various implementation strategies.For instance,it is possible to deliver an intervention specifically targeting the participants’SOC(i.e.,stage-matched intervention).8Over the past years,systematic reviews have examined the impact of stage-matched interventions promoting PA on stage progression14-18and pointed out inconsistent findings.Although the authors of those articles suggested that stage-matched interventions have more impact on PA compared with non-stage-matched interventions,none of these studies statistically tested this hypothesis.Another strategy to implement TTM-based interventions is to select participants based on their specific SOCs(i.e.,selection related to stage).For instance,Fahrenwald et al.19selected only participants in contemplation and preparation stages and applied the same material to all participants.The rationale behind these approaches is that each SOC is characterized by its specific motivational characteristics,and thus TTM-based interventions must be adapted to each SOC and its features(stage-matched interventions)to avoid mismatches resulting from different SOCs(nonstage-matched intervention).Moreover,these interventions are more effective in homogeneous groups(selected by stage strategy)compared with interventions with mixed SOCs(not selected by stage).However,there were no attempts to examine whether these strategies generate more important PA changes than the inclusion of participants whatever their SOC.
Lastly,another important issue is to determine whether a better theoretical implementation of TTM-based interventions,which integrates the theoretical constructs of the model(i.e.,decisional balance,temptation,self-efficacy,POC),is associated with higher intervention efficacy.Indeed,as those constructs are hypothesized to influence behavior change,9it seems reasonable to hypothesize that interventions that would explicitly target the theoretical constructs(decisional balance,temptation,self-efficacy,POC,and the number of theoretical constructs used)would report a higher impact.However,to our knowledge,no previous research has explored the moderating impact of the integration of those theoretical constructs on the efficacy of TTM-based interventions.
From those reports,the aim of the present meta-analysis was to examine whether the impact of TTM-based interventions on PA behavior varied according to(1)whether interventions were based on SOC or not(stage-matched interventionsvs.nonstage-matched intervention),and(2)selected by stagevs.not selected by stage(i.e.,participants were selected according to their SOC or not).The second aim was to examine the moderator effect of the theoretical constructs(decisional balance,temptation,self-efficacy,POC,and the number of theoretical constructs used)on the efficacy of TTM-based interventions on PA level.
2.Methods
This meta-analysis has been conducted following a strict protocol by using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)guidelines.20
2.1.Literature search
A systematic search was done on PubMed and PsycINFO until March 2016 using appropriate terms.We used keywords similar to those used by Gourlan et al.5for exercise:“exercise”OR “exercise therapy”OR “exercise movement techniques”OR “resistance training”OR “muscle stretching exercises”OR“breathing exercises”OR “sports”OR “motor activity”OR“relaxation”OR “physical fitness”OR “physical activity”OR “walk”.Those keywords were used in interaction with the following theory-relevant construct keywords to identify studies using the transtheoretical model:(1)SOC,(2)selfefficacy,(3)decisional balance,(4)POC,(5)temptation,and(6)TTM.The limits of search were ages above 18 years and randomized controlled trial(RCT)design.Then the references of 3 systematic reviews17,21,22were also scanned to be more exhaustive and improve the search strategy.All the included trials are available online in the supplementary file(Table A1).
The titles and abstracts found were screened by 2 trained reviewers(PB and CB).The final selection was based on fulltext reading and performed by 4 trained reviewers.Any disagreements were resolved by discussion with AJR.
2.2.Inclusion and exclusion criteria
For the present meta-analysis,studies were included if(1)they had a randomized controlled design,(2)they concerned adult participants(healthy or with a chronic disease),(3)the intervention was explicitly depicted as based on the TTM in the text,(4)at least 1 TTM construct was mentioned,and(5)PA was a primary or secondary outcome.Studies were further separated into stage-matched interventionsvs.non-stage matched interventions and selected by stagevs.not selected by stage interventions based on the information provided in each study.
2.3.Coding of characteristics
Two independent reviewers gathered the following data:authors,years of publication,sample characteristics,intervention characteristics,number of TTM constructs used,and outcomes.Regarding studies with several PA indicators(steps count,metabolic equivalents per week,PA duration)and/or those involving multiple methods to measure PA(accelerometer and questionnaire),the data were averaged to generate a single summary effect size.23Regarding the TTM,information about the theoretical constructs used was collected.To be considered as used,the theoretical construct had to be explicitly mentioned in the text.
2.4.Statistical analyses
Concerning the overall effect,effect sizes were calculated using Cohen’sd24with positive effect size indicating favorable changes in TTM-based interventions compared with the control groups.By convention,effect sizes of 0.2,0.5,and 0.8 represent small,medium,and large effect,respectively.24The moderation effects of selected by stagevs.not selected by stage interventions and stage-matched interventionsvs.non-stage-matched interventions criteria were separately assessed with a metaanalytical analogue of analysis of variance,using the between group heterogeneity statistic(Qb).25The same analyses were performed for the TTM constructs.Summary effects of interventions were computed by pooling subgroups of RCTs based on “matching”criteria.Given the expected high level of heterogeneity,statistical analyses were performed using a random effect.The publication bias was evaluated using a funnel plot.Statistical analyses were performed by using Comprehensive Meta-analysis(Version 2.2.064;Biostat,Englewood,NJ,USA).25
3.Results
3.1.Study selection
Database research led to the screening of 334 potentially relevant articles by applying the inclusion and exclusion criteria,and 33 articles focusing on the effects of TTM-based RCTs on PA were included in the present study(the flow chart is available online in the supplementary file Fig.A.1).
3.2.Study characteristics
A total sample of 10,350 participants(median:186.5;range:22-1369)was included in the present meta-analysis.Among included participants,5400(median:81;range:11-688)were in the control group and 4950(median:102;range:11-681)in the intervention group.Most of studies used mixed-sex samples,and 8 of the 33 studies were exclusively performed among women.The included population was aged 47.27±9.48(mean±SD)years old(median:47;range:26.48-70.30).
Regarding the included RCTs,4 studies were performed on workers,7 on specific populations(e.g.,low-income mothers),8 on sedentary people,and 14 on adults with chronic diseases(e.g.,type 2 diabetes).These interventions had mean duration of 22.33±21.13 weeks(median:14;range:2-100).RCTs are detailed online in supplementary file(Table A.1).
3.3.Bias of publication
The funnel plot of TTM-based interventions(as compared with controls)was found to be asymmetrical,which indicated the presence of a publication bias for these data(Fig.1).
3.4.Overall intervention effects
Regarding the overall effect of TTM-based interventions on PA,a significant effect was found(d=0.33;95%CI:0.22-0.43).
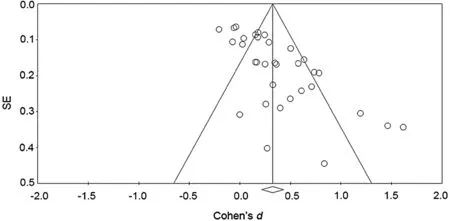
Fig.1.Funnel plot of publication bias.SE=standard error.
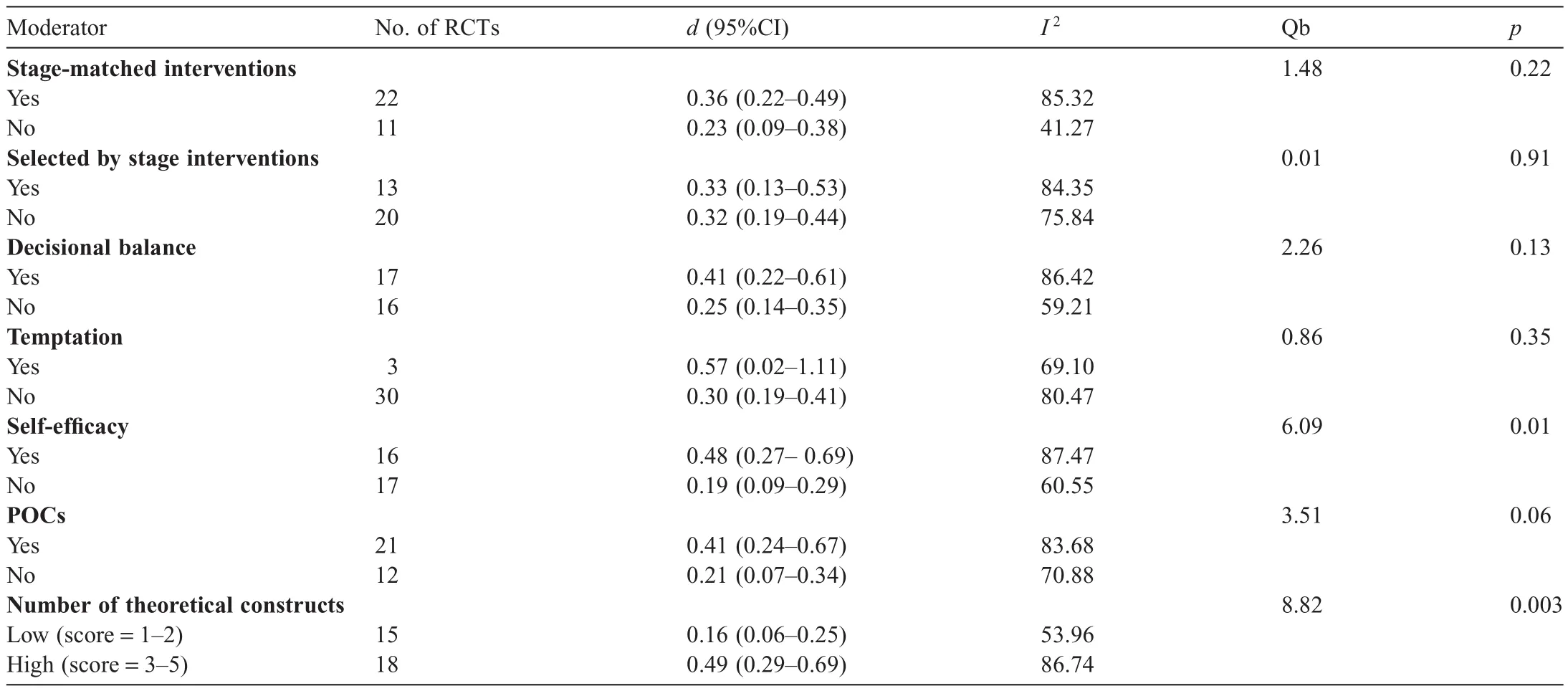
Table 1Analyses of moderators of TTM-based interventions as its constructs.
3.5.Moderator analyses
All statistical results are available in Table 1.
3.5.1.Stage-matched interventions vs.non-stage-matched interventions
Twenty-two studies of 33(67%)implemented a stagematched intervention.The moderation analyses did not reveal any differential efficacy in stage-matched interventions compared with non-stage-matched interventions (Qb=1.48,p=0.22).TTM-based interventions enhanced PA behavior whether they were stage matched(d=0.36;95%CI:0.22-0.49)or non-stage-matched(d=0.23;95%CI:0.09-0.38)(Fig.2).
3.5.2.Selected by stage vs.not selected by stage
interventions
Thirteen studies of 33(39%)selected their participants according to their SOC membership.The moderation analyses did not reveal any differential efficacy in selected by stage interventions compared with not selected by stage interventions(Qb=0.01,p=0.91).TTM-based interventions significantly improved PA behavior whether participants were selected by stage(d=0.33;95%CI:0.13-0.53)or not selected by stage(d=0.32;95%CI:0.19-0.44)(Fig.3).
3.5.3.Decisional balance
Seventeen studies of 33(52%)used decisional balance in their intervention.No statistical difference was found according to the use of the decisional balance(Qb=2.26,p=0.13).TTM-based interventions increased PA whether decisional balance was used or not.
3.5.4.Temptation
Three studies of 33(9%)used temptation in their intervention.No statistical difference was found according to the use of the temptation construct(Qb=0.86,p=0.35).TTM-based interventions increased PA whether temptation was used or not.
3.5.5.Self-efficacy
Sixteen studies of 33(48%)used self-efficacy in their intervention.A significant moderation effect of self-efficacy on PA behavior was observed(Qb=6.09,p=0.01),with studies using self-efficacy being more likely to increase PA behavior(d=0.48,95%CI:0.27-0.69)compared with studies that did not use this construct(d=0.19,95%CI:0.09-0.29).
3.5.6.POCs
Twenty-one studies of 33(64%)used the processes of change in their intervention.A moderation effect of processes of change on PA behavior was suggested with borderline significance(Qb=3.51,p=0.06),meaning that studies using processes of change were twice as likely to increase PA(d=0.41,95%CI:0.24-0.67)compared with those that did not(d=0.21,95%CI:0.07-0.34).
3.5.7.Number of TTM theoretical constructs
Eighteen studies of 33(55%)used at least 3 of the 5 TTM constructs(e.g.,SOC,decisional balance,temptation,selfefficacy,POC)to tailor their intervention.A significant moderation effect of the number of implemented constructs on PA behavior was observed(Qb=8.82,p=0.003),with studies using at least 3 constructs being 3 times more likely to increase PA(d=0.49,95%CI:0.29-0.69)compared with studies that used less than 3 constructs(d=0.16,95%CI:0.06-0.25).
4.Discussio n
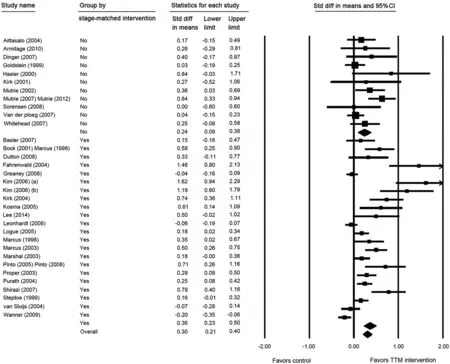
Fig.2.Forest plot of stage-matched interventions.Full references for the study names appear in the online supplemental material.CI=confidence interval;Std diff=standard difference;TTM=transtheoretical model.
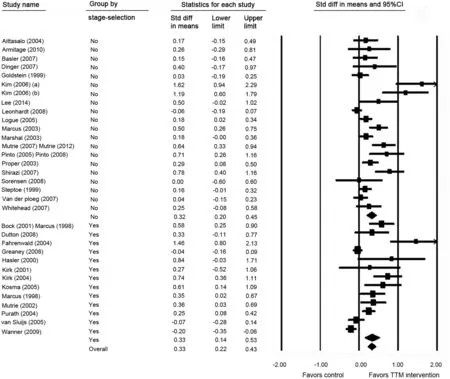
Fig.3.Forest plot of stage-selection interventions.Full references for the study names appear in the online supplemental material.CI=confidence interval;Std diff=standard difference;TTM=transtheoretical model.
The overall goal of this meta-analysis was to analyze the moderation effect of TTM theoretical constructs.The first objective was to investigate whether the impact of TTM-based interventions on PA behavior varied according to,on the one hand,stage-matched interventionsvs.non-stage-matched interventions(i.e.,the interventions were based on SOC or not),and,on the other hand,selected by stagevs.not selected by stage interventions(i.e.,participants were selected according to their SOC or not).The second objective was to investigate the moderation effect of the theoretical constructs(decisional balance,temptation,self-efficacy,POC)on TTM-based interventions aimed at promoting PA.
Regarding the first objective,the moderation analyses did not reveal any differential efficacy in interventions according to these moderators.TTM-based interventions showed significant improvement of PA behavior whether they were stage matched or non-stage-matched,and whether participants were selected by stage or not selected by stage.
Indeed,this result can be explained by the fact that SOCs have been defined differently across trials of PA promotion.In the literature,several staging algorithms have been used.For example,whereas some studies defined regular PA as 30 min per session at least 4 times per week,26,27other studies defined regular PA as 20 min per session or longer performed 3 to 5 times per week,8,28or as 30 min or more per day on 5 days per week.29,30So it is possible that this difference across RCTs could account for the failure of SOC to moderate outcomes in the present meta-analysis.However,another explanation is also possible.In fact,the present results suggest that SOC may not be the better way to implement TTM-based interventions to improve PA.As theoretically described,it is likely that TTM-based interventions are moderated by the other constructs.We therefore compared studies using at least 3 TTM constructs to tailor their interventions compared with those using less than 3 constructs.The first observation was that barely 50%of interventions used at least 3 TTM constructs.Then,as assumed by the TTM,7studies using more TTM constructs to tailor their interventions were 3 times more likely to increase PA than others.Indeed,studies that rightly implemented the TTM had an effect size that could be considered medium to large,whereas other studies had an effect size that could be considered small.Therefore,2 conclusions can be deduced from this result.The first point is that with 45%of included studies using 2 or fewer theoretical constructs,we can say that almost half of TTM-based studies are TTM inspired(constructs used separately)rather than really TTM driven(using all the theoretical constructs).31The second point is that PA interventions should use all TTM constructs to really know the efficacy of this model.Gourlan et al.5previously noticed that small effect size could be a result of poor implementation of a theory.This poor reporting associated with a poor implementation of theory-based interventions is not new32and may explain the mixed findings of previous studies using the TTM.
When we investigated more precisely the moderation effect of each of the other TTM constructs(i.e.,decisional balance,temptation,self-efficacy,POC),our analyses highlighted that self-efficacy and the POC were 2 constructs of importance in the TTM.Indeed,interventions that had included self-efficacy were more than twice as likely to increase PA compared with interventions that had not.This finding confirms previous investigations highlighting that self-efficacy is well known to be a powerful predictor of behavior change,as in facilitating the transition between the SOC33,34notably in conjunction with the POC.In fact,self-efficacy was able to predict the transition out of preaction stage,the retention in the maintenance stage of change,as the relapse to earlier stages.33-35
Studies that had included POC were twice as likely to increase PA compared with studies that had not.This result is of interest because POC,the experiential/behavioral mechanisms involved in behavior change,is a core construct of the TTM.Although important in the TTM,this construct was not systematically used in the interventions but was found to be associated with PA level and the transition between SOC and was a mediator of the adherence to PA.36-40In fact,in the TTM,POCs“provide important guide for interventions programs,as processes are like independent variables that people need to apply to move from stage to stage”.7Moreover,when activated during interventions,POCs can constitute a possible explanation for the results observed in stage-matched interventionsvs.nonstage-matched interventions and selected by stagevs.not selected by stage interventions.Effectively,even though these interventions were not designed to do so,it is possible that some included studies have used behavior change techniques that have further led to changes in POC and PA behavior.41
From a methodological point of view,a bias of publication was found in our present study with a lack of symmetry in the funnel plot.When analyzed,the funnel plot indicated an intervention-shifted bias,with small sample size studies being more likely to have larger effect size,which may have inflated our results.42This phenomenon could be explained by the fact that studies with small sample size and small effects are less likely to be published than studies with identical sample size showing large effects.43
The present study has some limitations.First,given the overall weakness of the TTM construct implementation,we still do not have enough information about its precise efficacy even though our results showed that properly implemented studies had medium to large effect size.Second,it is possible that other study characteristics could have moderated the effect estimates of RCTs designed to improve PA,such as the frequency of contact with participants,the presence of supervised PA sessions,44,45or the methodological quality criteria of RCTs.12,46,47For example,it is known that theory-based interventions including female participants yielded greater effect size than interventions including solely males or mixed populations.47Although the sex effect was no longer significant when entered into the multivariate analysis,we cannot exclude that it could probably have a role in our results,such as other demographic parameters(e.g.,age,presence of chronic diseases).Nevertheless,these aspects were beyond the scope of the present study.Another limitation was the relatively small number of included studies,which probably had limited power to find differences.Indeed,our data were limited by how the moderators were distributed across trials.For example,the test for temptation as a moderator examined only 3 trials compared with the remaining 30 studies,which necessarily had an impact on power.
Consequently,and as recommended for studies with interventions,48other theoretical constructs of the TTM that could moderate its efficacy regarding PA should be more frequently and accurately employed and reported in publications to be analyzed in further meta-regression analyses.
Several strengths should also be acknowledged.To our knowledge,this is the first study that has statistically tested whether tailoring the intervention according to participants’SOC would lead to higher changes in PA than applying the same program to everyone.A second strength is that this meta analysis was the first to show the evidence-based efficacy of the TTM constructs on PA behavior and to further confirm the interest in the entire model.Finally,to keep a higher level of evidence-based approach,only RCTs were included,which strengthened our results.
5.Conclusion
In conclusion,matching or not matching interventions and participants according to their SOCs did not moderate the effect of TTM-based interventions on PA promotion.TTM-based interventions significantly improved PA behavior whether interventions or participants were matched with SOC or not.Future TTM studies should report accurately how they used TTM constructs and pay attention to the implementation of the greatest number of TTM constructs,with particular importance paid to self-efficacy and the POC.
Authors’contributions
All authors conceived of the study design.AJR,PB,JB,CB,OL,and MG did the literature review and extracted the data;AJR,PB,GN,and MG did the literature review update;AJR,MG,PB,and MC did the statistical plan and analyses;AJR,CB,PB,GN,and MC wrote the first draft of the manuscript;ED assisted in the literature update and review.All authors did a significant revision to the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Appendix:Supplementary material
Supplementary data to this article can be found online at doi:10.1016/j.jshs.2016.10.007.
1.Dumith SC,Hallal PC,Reis RS,Kohl 3rd HW.Worldwide prevalence of physical inactivity and its association with human development index in 76 countries.Prev Med2011;53:24-8.
2.Hallal PC,Andersen LB,Bull FC,Guthold R,Haskell W,Ekelund U,et al.Global physical activity levels:surveillance progress,pitfalls,and prospects.The Lancet2012;380:247-57.
3.Ng SW,Popkin BM.Time use and physical activity:a shift away from movement across the globe.Obes Rev2012;13:659-80.
4.Lee C,Joseph L,Colosimo A,Dasgupta K.Mortality in diabetes compared with previous cardiovascular disease:a gender-specific meta-analysis.Diabetes Metab2012;38:420-7.
5.Gourlan M,Bernard P,Bortholon C,Romain AJ,Lareyre O,Carayol M,et al.Efficacy of theory-based interventions to promote physical activity.A meta-analysis of randomised controlled trials.Health Psychol Rev2016;10:50-66.
6.Prochaska JO,DiClemente CC.Stages and processes of self-change of smoking:toward an integrative model of change.J Consult Clin Psychol1983;51:390-5.
7.Prochaska JO,Redding CA,Evers KE.The transtheoretical model and stages of change.In:Glanz K,Rimer BK,Viswanath K,editors.Health behavior and health education:theory,research and practice.4th ed.Hoboken,NJ:Jossey-Bass;2008.p.97-121.
8.Marcus BH,Rossi JS,Selby VC,Niaura RS,Abrams DB.The stages and processes of exercise adoption and maintenance in a worksite sample.Health Psychol1992;11:386-95.
9.Prochaska JO,DiClemente CC,Norcross JC.In search of how people change:applications to addictive behaviors.Am Psychol1992;47:1102-14.
10.Hausenblas HA,Nigg CR,Dannecker EA,Downs DS,Gardner RE,Fallon E,et al.A missing piece of the transtheoretical model applied to exercise:development and validation of the temptation to not exercise scale.Psychol Health2001;16:381-90.
11.Bandura A.Self-efficacy:toward a unifying theory of behavioral change.Psychol Rev1977;84:191-215.
12.Conn VS,Hafdahl AR,Mehr DR.Interventions to increase physical activity among healthy adults:meta-analysis of outcomes.Am J Public Health2011;101:751-8.
13.Michie S,Prestwich A.Are interventions theory-based?Development of a theory coding scheme.Health Psychol2010;29:1-8.
14.Adams J,White M.Are activity promotion interventions based on the transtheoretical model effective?A critical review.Br J Sports Med2003;37:106-14.
15.Brug J,Conner M,Harré N,Kremers S,McKellar S,Whitelaw S.The Transtheoretical Model and stages of change:a critique:observations by five commentators on the paper by Adams,J.and White,M.(2004)why don’t stage-based activity promotion interventions work?Health Educ Res2004;20:244-58.
16.Riemsma RP,Pattenden J,Bridle C,Mather L,Watt IS,Walker A,et al.A systematic review of the effectiveness of interventions based on a stages-of-change approach to promote individual behaviour change.Health Technol Assess2002;6:1-231.
17.Spencer L,Adams TB,Malone S,Roy L,Yost E.Applying the transtheoretical model to exercise:a systematic and comprehensive review of the literature.Health Promot Pract2006;7:428-43.
18.Van Sluijs EM,van Poppel MN,van Mechelen W.Stage-based lifestyle interventions in primary care.Am J Prev Med2004;26:330-43.
19.Fahrenwald NL,Atwood JR,Walker SN,Johnson DR,Berg K.A randomized pilot test of “Moms on the Move”:a physical activity intervention for WIC mothers.Ann Behav Med2004;27:82-90.
20.Moher D,Liberati A,Tetzlaff J,Altman DG,The PRISMA Group.Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement.PLoS Med2009;6:e1000097.doi:10.1371/journal.pmed.1000097
21.Marshall SJ,Biddle SJ.The transtheoretical model of behavior change:a meta-analysis of applications to physical activity and exercise.Ann Behav Med2001;23:229-46.
22.Hutchison AJ,Breckon JD,Johnston LH.Physical activity behavior change interventions based on the transtheoretical model:a systematic review.Health Educ Behav2009;36:829-45.
23.Rosenthal R,Rubin DB.Meta-analytic procedures for combining studies with multiple effect sizes.Psychol Bull1986;99:400-6.
24.Cohen J.Statistical power analysis for the behavioral sciences.2nd ed.Hillsdale,NJ:L.Erlbaum Associates;1988.
25.Borenstein M,Hedges LV,Higgins JPT,Rothstein HR.Introduction to meta-analysis.Chichester:John Wiley& Sons,Ltd;Available at:http://doi.wiley.com/10.1002/9780470743386;2009 [accessed 22.09.2015].
26.Nigg C,Hellsten L,Norman G,Braun L,Breger R,Burbank P,et al.Physical activity staging distribution:establishing a heuristic using multiple studies.Ann Behav Med2005;29(Suppl.):S35-45.
27.Romain AJ,Bernard P,Attalin V,Gernigon C,Ninot G,Avignon A.Health-related quality of life and stages of behavioural change for exercise in overweight/obese individuals.Diabetes Metab2012;38:352-8.
28.Schumann A,Nigg CR,Rossi JS,Jordan PJ,Norman GJ,Garber CE,et al.Construct validity of the stages of change of exercise adoption for different intensities of physical activity in four samples of differing age groups.Am J Health Promot2002;16:280-7.
29.Garber CE,Allsworth JE,Marcus BH,Hesser J,Lapane KL.Correlates of the stages of change for physical activity in a population survey.Am J Public Health2008;98:897-904.
30.Farmanbar R,Niknami S,Lubans DR,Hidarnia A.Predicting exercise behaviour in Iranian college students:utility of an integrated model of health behaviour based on the transtheoretical model and self-determination theory.Health Educ J2012;72:56-69.
31.Michie S,Abraham C.Interventions to change health behaviours:evidence-based or evidence-inspired?Psychol Health2004;19:29-49.
32.Prestwich A,Webb TL,Conner M.Using theory to develop and test interventions to promote changes in health behaviour:evidence,issues,and recommendations.Curr Opin Psychol2015;5:1-5.
33.Plotnikoff RC,Hotz SB,Birkett NJ,Courneya KS.Exercise and the transtheoretical model:a longitudinal test of a population sample.Prev Med2001;33:441-52.
34.Levy SS,Li KK,Cardinal BJ,Maddalozzo GF.Transitional shifts in exercise behavior among women with multiple sclerosis.Disabil Health J2009;2:216-23.
35.Lipschitz JM,Yusufov M,Paiva A,Redding CA,Rossi JS,Johnson S,et al.Transtheoretical principles and processes for adopting physical activity:a longitudinal24-month comparison of maintainers,relapsers,and nonchangers.J Sport Exerc Psychol2015;37:592-606.
36.Dishman RK,Jackson AS,Bray MS.Self-regulation of exercise behavior in the TIGER Study.Ann Behav Med2013;48:80-91.
37.Kirk AF,Mutrie N,MacIntyre PD,Fisher MB.Promoting and maintaining physical activity in people with type 2 diabetes.Am J Prev Med2004;27:289-96.
38.Romain AJ,Attalin V,Sultan A,Boegner C,Gernigon C,Avignon A.Experiential or behavioral processes:which one is prominent in physical activity?Examining the processes of change 1 year after an intervention of therapeutic education among adults with obesity.Patient Educ Couns2014;97:261-8.
39.Romain AJ,Bernard P,Galvez M,Caudroit J.Response to an exercise intervention for patients with type 2 diabetes:a preliminary study of processes of change:physical activity and processes of change.J Appl Biobehav Res2015;20:130-6.
40.Romain AJ,Horwath C,Bernard P.Prediction of physical activity level using processes of change from the transtheoretical model.Experiential,behavioral,or an interaction effect?Am J Health Promot2018;32:16-23.
41.Lowther M,Mutrie N,Scott EM.Identifying key processes of exercise behaviour change associated with movement through the stages of exercise behaviour change.J Health Psychol2007;12:261-72.
42.Sterne JA,Egger M.Funnel plots for detecting bias in meta-analysis:guidelines on choice of axis.J Clin Epidemiol2001;54:1046-55.
43.Macaskill P,Walter SD,Irwig L.A comparison of methods to detect publication bias in meta-analysis.Stat Med2001;20:641-54.
44.Baillot A,Romain AJ,Boisvert-Vigneault K,Audet M,Baillargeon JP,Dionne IJ,et al.Effects of lifestyle interventions that include a physical activity component in class II and III obese individuals:a systematic review and meta-analysis.PLoS One2015;10:e0119017.doi:10.1371/journal.pone.0119017
45.Gourlan MJ,Trouilloud DO,Sarrazin PG.Interventions promoting physical activity among obese populations:a meta-analysis considering global effect,long-term maintenance,physical activity indicators and dose characteristics.Obes Rev2011;12:e633-45.doi:10.1111/j.1467-789X.2011.00874.x
46.Carayol M,Delpierre C,Bernard P,Ninot G.Population-,intervention and methodology-related characteristics of clinical trials impact exercise efficacy during adjuvant therapy for breast cancer:a meta-regression analysis:exercise for adjuvant breast cancer:meta-regression analysis.Psychooncology2015;24:737-47.
47.Bernard P,Carayol M,Gourlan M,Boiché J,Romain AJ,Bortolon C,et al.Moderators of theory-based interventions to promote physical activity in 77 randomized controlled trials.Health Educ Behav2017;44:227-35.
48.Hoffmann TC,Glasziou PP,Boutron I,Milne R,Perera R,Moher D,et al.Better reporting of interventions:template for intervention description and replication (TIDieR)checklist and guide.BMJ2014;348:g1687.doi:10.1055/s-0041-111066
49.Higgins JPT,Green S,Cochrane Collaboration,editors.Cochrane handbookfor systematicreviews of interventions.Hoboken,NJ:Wiley-Blackwell;2008.
杂志排行

Journal of Sport and Health Science的其它文章
- Research highlights from the Status report for step it up!The surgeon general’s call to action to promote walking and walkable communities
- Environments favorable to healthy lifestyles:A systematic review of initiatives in Canada
- The built environment correlates of objectively measured physical activity in Norwegian adults:A cross-sectional study
- The association of various social capital indicators and physical activity participation among Turkish adolescents
- Feasibility of using pedometers in a state-based surveillance system:2014 Arizona Behavioral Risk Factor Surveillance System
- Collegiate athletes’mental health services utilization:A systematic review of conceptualizations,operationalizations,facilitators,and barriers