Feasibility of using pedometers in a state-based surveillance system:2014 Arizona Behavioral Risk Factor Surveillance System
2018-04-26AlbertoFlrezPregoneroJanetFultonJoanDornBarbaraAinsworth
Alberto Flórez-Pregonero,Janet E.Fulton,Joan M.Dorn,Barbara E.Ainsworth*
aSchool of Nutrition and Health Promotion,College of Health Solutions,Arizona State University,Phoenix,AZ 85004,USA
bPontificia Universidad Javeriana,Bogotá 110231,Colombia
cPhysical Activity and Health Branch,Division of Nutrition,Physical Activity,and Obesity,Center for Chronic Disease Prevention and Health Promotion,U.S.Centers for Disease Control and Prevention,Atlanta,GA 30340,USA
dDepartment of Community Health and Social Medicine,City University of NewYork(CUNY)School of Medicine,NewYork,NY 10031,USA
1.Introduction
Physical activity(PA)surveillance is performed in public health settings to monitor PA levels over time,assess needs of population groups at risk for low PA levels,evaluate the effects of PA promotion programs,and determine changes in PA behaviors over time.1Most PA surveillance in the USA is based on telephone-and self-administered questionnaires.2
In the framework of strategic priorities for PA surveillance for U.S.adults,experts1have called for innovative strategies to improve public health PA surveillance activities.Walking is the most commonly reported PA by U.S.dults and represents an important behavior that contributes to meeting PA guidelines.3,4Pedometers may be a feasible,innovative method to obtain useful information for public health planning purposes.Pedometers have been used in national surveys to characterize PA levels in adult populations in Denmark,5Japan,6and Western Australia.7In the USA,steps taken have been obtained from accelerometers used in 2005-2006 National Health and Nutrition Examination Survey(NHANES).8Because the priority of the U.S.surveillance systems is to monitor the 2008 Physical Activity Guidelines for Americans,and the guidelines do not recommend an optimal number of steps taken,pedometers have not been incorporated into U.S.PA surveillance systems.Nevertheless,using pedometers to measure steps taken in a PA surveillance system may have relevance for public health practice as recently highlighted byStep it up!The surgeongeneral’s call to action to promote walking and walkable communities,in which gaps in walking surveillance have been identified.4
To examine the feasibility of using pedometers in a statelevel surveillance system,we conducted a study of pedometer use in a sub-sample of respondents completing the 2014Arizona Behavioral Risk Factor Surveillance System(AZ-BRFSS).
2.Materials and methods
2.1.BRFSS questionnaire
The BRFSS is an ongoing,national surveillance system and data are collected by each state and U.S.territories to measure behavioral risk factors for the noninstitutionalized adult population(≥18 years)residing in the USA and territories.The BRFSS uses a multistage sampling design to select a representative sample of adults to be interviewed.Both landline-and cellular telephone-based surveys are administered.The BRFSS survey consists of a core set of questions that all states administer,optional questionnaire modules about topics of specific relevance to certain states(e.g.,health care access,sugar drinks),and state-added questions.9In Arizona,the BRFSS is conducted by the Arizona Department of Health Services(ADHS)and administered by an independent contractor hired by the ADHS.The present study was approved by the Arizona State University Office of Research Integrity and Assurance and the ADHS Institutional Review Board.
2.2.Recruitment
Recruitment occurred between May and September 2014 and was stopped after a pre-established quota of 800 pedometers were mailed to respondents who agreed to participate in the study.Enrollment in the study was limited because only 800 pedometers were available to distribute to the participants.Eligible respondents were adults living in Maricopa County,who completed the 2014 BRFSS,were ambulatory,and were willing to listen to an invitation to participate in the state-added pedometer study at the end of the survey.Interested respondents were told about the pedometer study and what it involved.They were asked if they would like to participate.More details about the study invitation are provided in Appendix 1.
2.3.Study materials
Each participant was mailed a study packet consisting of an instruction page describing tasks to complete for the study,a pedometer with wearing instructions,a questionnaire about walking behaviors,a logbook to record daily steps,a copy of the informed consent statement,and a pre-addressed stamped envelope to return the completed logbook and walking questionnaire.All materials were available in English and Spanish languages.The study packet was prepared by the research team and sent by mail to the BRFSS contractor who mailed the study packet to each participant that agreed to participate.Informed consent was implied by respondents agreeing to participate in the study.
2.3.1.Instruction page
An instruction page informed participants how the pedometer worked,when and where to wear the monitor,how to obtain and record steps in a logbook,how to complete the walking questionnaire,and how to return the questionnaire and step logbook in the pre-stamped envelope.Participants were allowed to keep the pedometer following study participation.A toll-free number was provided for participants to call one of us(BEA)with questions about the study and/or how to use the pedometer.
2.3.2.Pedometer
The Omron HJ324U(Omron Corp.,Kyoto,Japan)is a small tri-axial pedometer with 5 activity modes that track total steps,aerobic steps(cadence,≥100 steps/min),steps per minute,distance walked,and estimated calories expended.The pedometer stores up to 22 days of data and displays steps taken for the current day and the previous 7 days.As the study team was interested in obtaining total steps,aerobic steps,and steps per minute counts only,the pedometers were pre-programed with a standard age(45 years),height(67 inches),weight(150 lbs.),sex(male),and stride length(60 inches)to eliminate data needed to estimate distance walked and energy expenditure.The pedometer was worn on the hip to standardize the pedometer placement.
2.3.3.Walking questionnaire
西达里亚项目组成立后,组织架构从“管理区-办公室-岗位”三级管理变成“项目经理-岗位”两级业务指导,减少巡检车1辆、专业服务人员9人,年降低费用104万元。
A questionnaire developed for this study asked participants if they had changed their intentional walking behaviors while wearing the pedometer(walked more,walked less,stayed the same)and to identify participants’perception of the ease of wearing the pedometer for 7 days(very difficult,somewhat difficult,somewhat easy,very easy).
2.3.4.Step logbook
A logbook developed for this study included spaces for participants to write the date,day of the week,total daily steps,aerobic steps,and steps per minute for each day the pedometer was worn.
2.4.Data collection procedures
Participants were instructed to wear the pedometer for 7 consecutive days except during sleep or while in water and to record data from the pedometer into a logbook each night before going to bed.After 7 days,participants were instructed to return the step logbook and the walking questionnaire in the pre-stamped envelope.
The BRFSS contractor conducted up to 9 follow-up/reminder calls to participants that did not return the step logbook within a 3-week period.Participants that did not return the step logbook after 3-4 weeks were classified as nonresponders.
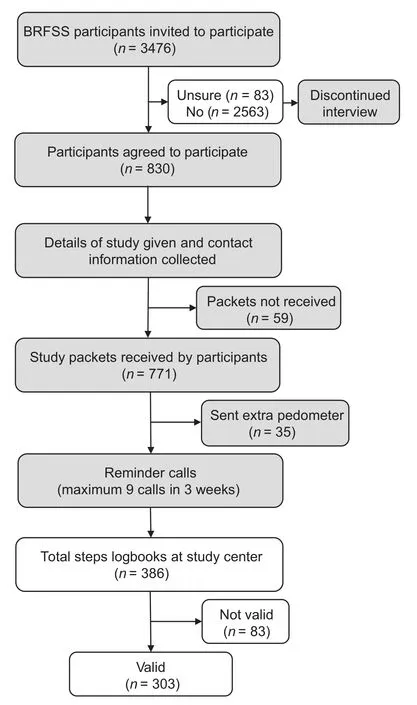
Fig.1.Overview of the Pedometer Study processes.The clear boxes indicate an activity completed by the study center activity and gray filled boxes indicate an activity completed by the Behavioral Risk Factor Surveillance System(BRFSS)contractor.
2.5.Variables and data analysis
Descriptive information for each participant was obtained from the 2014 AZ-BRFSS provided by the ADHS.Means and standard deviations and proportions were computed to characterize the sample by sex,age,race/ethnicity,education level,household income,and marital status and by PA levels using categories developed by Tudor-Locke et al.12as sedentary(<5000 steps/day),low active(5000-7499 steps/day),somewhat active(7500-9999 steps/day),active(10,000-12,499 steps/day),and highly active(≥12,500 steps/day).Means and standard deviations and proportions also were computed for selected feasibility metrics of acceptability(related to participation metrics)and demand(related to the return of data metrics)by the descriptive information.Statistical tests for differences between measures were not computed.Descriptive analysis and calculations needed to determine the feasibility metrics were performed using SAS Version 9.4(SAS Institute Inc.,Cary,NC,USA).
Feasibility was assessed using the framework proposed by Bowen et al.13for the following metrics:acceptability,demand,implementation,and practicality.Table 1 presents the operational definitions and formulas for the feasibility metrics.Levels for acceptable feasibility metrics have not been determined.
3.Results
Among the 3476 Maricopa County residents who completed the 2014 AZ-BRFSS during May to September 2014,830 agreed to participate in the study.Of those who agreed to participate,771(92.9%)received a study packet and were enrolled in the study(Table 2).The remaining 7.1%did not receive a study packet,or after receiving the study packet,indicated they were no longer interested in the study.
Implementation took 5 months(May to September 2014)to enroll 771 participants,at an average of 154 participants per month(Table 3).The cost to conduct the study was USD18,661,representing USD23.10 per delivered study packet to 809 respondents who agreed to participate in the study.A total of 771 packets were received by persons who enrolled in the study.During the follow-up calls reminding participants to return their data,38 requested additional packets were sent to them.The cost for each set of valid data(n=303)was USD61.60.A breakdown of the study costs is presented in Appendix 2.
The average number of steps/day and pedometer-determined PA levels by selected demographic characteristics are presented in Table4.On average,participants took 6363±3049steps/day.Based on their step data,most were classified as sedentary(36.0%)and low active(35.6%),with fewer classified as somewhat active(17.2%),active(7.6%),and highly active(3.6%).14
4.Discussion
The feasibility of using pedometers in a PA surveillance system was low-to-moderate in this sample.While the studywas implemented as planned and the cost to obtain valid step count data was on the order of USD61.60 per person,acceptability was low with only a quarter of respondents invited agreeing to participate in the study.There was modest demand for the study with approximately 40%of adults participating returning valid data.
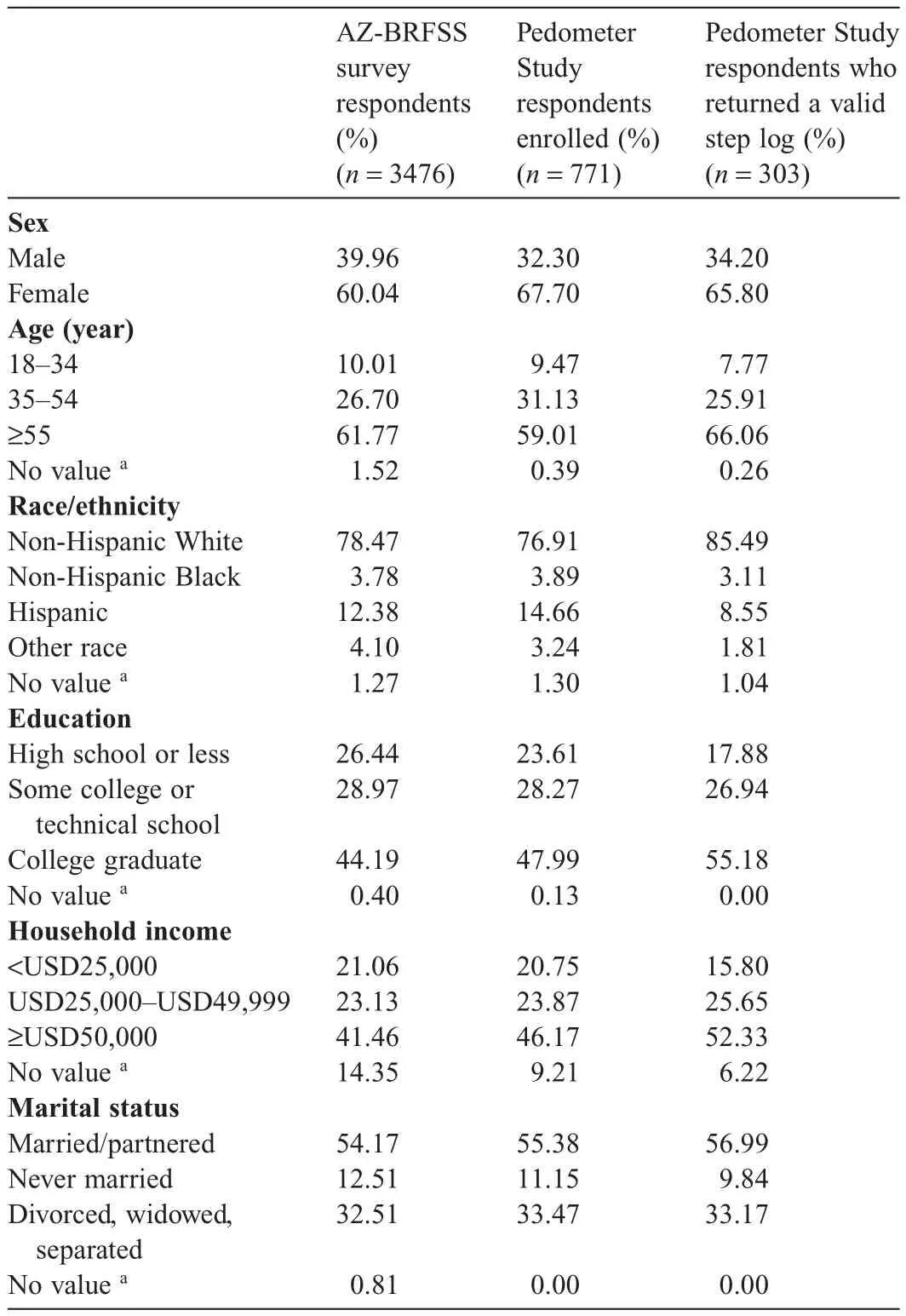
Table 2Demographic characteristics for participants from the 2014Arizona Behavioral Risk Factor Surveillance System(AZ-BRFSS)and the 2014 Pedometer Study.
The low acceptability reflects the extent to which the study was judged as suitable and attractive to respondents invited to participate in the study.Of those invited,only 24%agreed to wear a pedometer for 7 consecutive days.Whereas this response rate is similar to the 31% response rate observed by Tudor-Locke et al.12in a similar7-day pedometer surveillance feasibility study among209adults residing in Sumter,SC,it is lower than the 45% response rate reported for 2522 adults agreeing to wear a pedometer for 2 days in the American on the Move initiative,10and the 66%response rate for the 1098 adults agreeing to wear a pedometer for 4 days in the Colorado on the Move initiative.11
The acceptability metric may have been influenced by combining the study with a telephone-based surveillance survey that asks questions about varied health behaviors(similar to Tudor-Locke’s methods for their pedometer feasibility study)and that participating in the study linked the participant’s name with data collected on BRFSS moved the study from anonymous to confidential.This is in contrast to the American on the Move and the Colorado on the Move survey which was designed specifically to recruit participants into walking initiatives and was not designed as an anonymous survey.Others may have said no just to end the AZ-BRFSS survey at the end of the core and optional questions.It is also possible that wearing a pedometer for 7 days and requiring participants to record their data nightly represented too much of a commitment for some respondents.Additionally,placing the pedometer study invitation at the end of the 2014 AZ-BRFSS questionnaire eliminated the opportunity for those who terminated the BRFSS interview early to participate in the study.Studies that have used pedometers in surveillance settings have included wear times rangingfrom 1 to 7 consecutive days.In international surveillance settings that have used pedometers,Danish5and Western Australian7systems collected pedometer data for 7 days;whereas a Japanese6surveillance system collected data for a single day.In the previously mentioned U.S.pedometer studies,pedometer wear time ranged from 2 to 7 days.13-15Additional studies are needed to determine the optimal number of days to collect pedometer data to optimize acceptability in surveillance settings.

Table 3Selected feasibility metrics by demographic characteristics for the 2014 Pedometer Study.
Fewer than half the respondents followed the study protocol as presented(demand).Similar patterns were observed among all demographic groups.The return rates and valid logbook rates were best in participants with the highest educational attainment and household incomes,married or partner status,non-Hispanic White race,males,and in the oldest age group.The relatively low return rates with valid data can be due to several factors.While pedometers have high validity and reliability and generally are easy to use,15most of the participants calling the 1-800 number for assistance were confused with how to use the pedometers.Several participants tried to program their pedometers which made the units nonfunctional.Others expressed frustration with the small screen and/or were unable to read the data.A few people just returned the pedometer with a note that it was too difficult to use.In retrospect,the pedometer model used in the current study(Omron HJ324U)may have been a deterrent to receiving valid data due to its difficulty in accessing the data.The aforementioned U.S.studies with higher return rates(31%-66%)for valid data used pedometers that have only 1 button to press to display steps/day.Since nearly two thirds(59%)of the current study were aged 55 years and older,this underscores the need to use a pedometer and a study protocol that is easy for older adults to use and to follow,respectively.
Another reason for the low acceptability of the study relates to the receipt of the study packet.Thirty-eight participants requested an extra study packet containing the pedometer as they either lost the original study packet,broke the pedometer,or were unable to access the step data from the pedometer.It is unknown if these participants wore the pedometer and returned the data as planned.
Recording data into the step logbook seemed problematic.Nearly a quarter(22%)of the step data written into the step logbook were invalid(<3 days/week with data or <1000 or>25,000 steps/day)or missing.Most likely the difficulty in accessing and reading the step data contributed to the incorrect recording of the participants’step data.This underscores theneed to use pedometers for surveillance purposes that require the fewest interactions between the participant and the pedometer.Ideally,pedometers with wireless capacity to download data into a smart phone or computer without having to read and record the data should eliminate errors in writing step counts into a logbook.Further,using a software system that allows data to be uploaded to the study center may have the greatest potential to increase the demand for pedometer surveillance systems.

Table 4The average of steps per day and percent of pedometer-determined physical activity levels by selected demographic characteristics for the 2014 Pedometer Study.
The study was implemented as planned with 93%of the 800 pedometers being distributed in 5 months.However,nearly three fourths of persons invited to participate in the study declined to do so.Of those agreeing to participate,the proportion was biased to more educated and white race relative to those who participated in the 2014 AZ-BRFSS.If this study were repeated,it is recommended that a sufficient number of pedometers are available to recruit participants during the entire duration of the BRFSS survey and that strategies be used to reduce the refusal rate.
The resources available for this study were modest(USD16,400);however,due to the number of returned logbooks with incorrect data,the cost for each valid data point was USD61.60.Notably,the costs would have been much lower(USD21.27)if all participants starting the study had returned valid data.On the other hand,the cost per person would have been USD21 higher(USD82.60)if the pedometers had been purchased.The study costs were relatively low because the pedometers were donated and the study was linked to the 2014 AZ-BRFSS.It is anticipated that implementation costs could have been reduced further by using internet-based methods to upload the step data into an electronic dataset.However,this latter mode would have some costs to develop and/or access a data collection platform.
While this study reflects an initial attempt to obtain pedometer step data as an add-on to a state-based surveillance system,its limitations should be noted.The study sample included only residents of Maricopa County,AZ who participated in the 2014 AZ-BRFSS.As Maricopa County is primarily urban with a demographic profile that differs from more rural parts of Arizona,the results do not reflect the feasibility metric data of those not invited to participate in the study.Also,the majority of respondents were female,55 years and older,non-Hispanic white race,college educated,married,and earning a high income.While this distribution is similar to respondents completing the 2014 AZ-BRFSS and other telephone surveys in adult populations,including the BRFSS,16the sample under-represents minorities,younger adults,and those with lower incomes and educational attainment.
The step counts obtained in the total sample averaged 6363±3049 steps/day.This is similar to average step counts obtained in the Sumter,SC(5931±3664 steps/day),17Colorado on the Move(6804 steps/day),112005-2006 NHANES(6540 steps/day),8and America on the Move(5117 steps/day)10cohorts.Among the step counts obtained in the current study,nearly two thirds(71.6%)were in the inactive and low-active categories.14This underscores the need for community initiatives such asStep it up!The surgeon general’s call to action to promote walking and walkable communities,to increase PA among adults of all ages.
5.Conclusion
While self-report measures have been the mainstay of PA surveillance systems,device-based methods have the potential to add more accurate assessments of PA motion.This study assessed the feasibility of adding pedometers to a sub-sample of respondents to the 2014 AZ-BRFSS.Acceptability was modest at best with only a quarter of respondents invited agreeing to participate in the study.The demand for accurate step-count data also was modest with return rates of valid data approximating 40%of those participating in the study.The study was implemented as planned and the cost to obtain valid step count data was approximately of USD62 per person.The feasibility of collecting pedometer data likely can be improved by using pedometers that are easy for respondents to use,where data can be downloaded into a smart phone or computer for direct access by the study center,and with monitoring for a shorter duration.
This study was partially supported under a contract from McKing Consulting(#4568)with the U.S.Centers for Disease Control and Prevention(200-2012-F-53729)to assist with pedometer distribution.We are grateful to Omron Inc.for donating the pedometers used in the study and to Judy Bass and her staff from the Arizona Department of Health Services for her assistance in making this study possible.
Authors’contributions
AFP carried out the data collection,performed the statistical analysis,and drafted the manuscript;BEA conceived of the study,created the study design,and helped to edit the manuscript;JEF helped to draft and edit the manuscript;JMD helped to design the study and edit the manuscript.All the authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Appendix 1
Invitation for the pedometer sub-study read to the respondents of the 2014 Arizona Behavioral Risk Factor Surveillance System(AZ-BRFSS)who lived in Maricopa County.
“We are conducting a physical activity study using pedometers.Pedometers are small devices that clip to your clothing and count the number of steps you take each day.If you agree to participate in this study you will wear the pedometer we give to you for 7 consecutive days,1 week,during your waking hours.At the end of 7 days you will put your logbook and questionnaire into an addressed,pre-paid envelope and drop it into a mail box.Your information will be strictly confidential and you will receive a full report of your individual results at the end of the study.Would you like to participate in our study?”
Appendix 2
Cost breakdown for the 2014 Arizona Behavioral Risk Factor Surveillance System(AZ-BRFSS)pedometer study

Note:Participant costs would have been increased by approximately USD21 if the pedometers had been purchased.
1.Fulton JE,Carlson SA,Ainsworth BE,Berrigan D,Carlson C,Dorn JM,et al.Strategic priorities for physical activity surveillance in the United States.Med Sci Sports Exerc2016;48:2057-69.
2.U.S.Centers for Disease Control and Prevention.Surveillance Systems.Available at:https://www.cdc.gov/physicalactivity/data/surveillance.htm;2015[accessed 23.07.2017].
3.Berrigan D,Carroll DD,Fulton JE,Galuska DA,Brown DR,Dorn JM,et al.Vital signs:walking among adults—United States,2005 and 2010.MMWR Morb Mortal Wkly Rep2012;61:595-601.
4.U.S.Department of Health and Human Services.Step it up!The surgeon general’s call to action to promote walking and walkable communities.Washington,DC:U.S.Department of Health and Human Services,Office of the Surgeon General;2015.
5.Matthiessen J,Andersen EW,Raustorp A,Knudsen VK,Sorensen MR.Reduction in pedometer-determined physical activity in the adult Danish population from 2007 to 2012.Scand J Public Health2015;43:525-33.
6.Inoue S,Ohya Y,Tudor-Locke C,Yoshiike N,Shimomitsu T.Step-defined physical activity and cardiovascular risk among middle-aged Japanese:the National Health and Nutrition Survey of Japan.J Phys Act Health2006;9:1117-24.
7.Rosenberg M,Mills C,McCormack G,Martin K,Grove B,Pratt S,et al.Physical activity levels of Western Australian adults 2009: findings from the Physical Activity Taskforce Adult Physical Activity Survey.Perth:Health Promotion Evaluation Unit,The University of Western Australia.2010.
8.Tudor-Locke C,Johnson WD,Katzmarzyk PT.Accelerometer-determined steps per day in US adults.Med Sci Sports Exerc2009;41:1384-91.
9.U.S.Centers for Disease Control and Prevention.Behavioral Risk Factor Surveillance System Overview:BRFSS 2014.GA:Atlanta.2015.
10.Bassett D,Wyatt HR,Thompson H,Peters JC,Hill JO.Pedometer measured physical activity and health behaviors in U.S.adults.Med Sci Sports Exerc2010;42:1819-25.
11.Wyatt H,Peters JC,Reed GW,Barry M,Hill JO.A Colorado statewide survey of walking and its relation to excessive weight.Med Sci Sports Exerc2005;37:724-30.
12.Tudor-Locke C,Lind KA,Reis JP,Ainsworth BE,Macera CA.A preliminary evaluation of a pedometer-assessed physical activity self-monitoring survey.Field Methods2004;16:422-38.
13.Bowen D,Kreuter M,Spring B,Cofta-Woerpel L,Linnan L,Weiner D,et al.How we design feasibility studies.Am J Prev Med2009;36:452-7.
14.Tudor-Locke C,Hatano Y,Pangrazi RP,Kang M.Revisiting“How many steps are enough?”Med Sci Sports Exerc2008;40(Suppl.2):S537-43.
15.Tudor-Locke C,Lutes L.Why do pedometers work?:a reflection upon the factors related to successfully increasing physical activity.Sports Med2009;39:981-93.
16.Link M,Mokdad A.Can web and mail survey modes improve participation in an RDD-based national health surveillance?J Off Stat2006;22:293-312.
17.Tudor-Locke C,Ham SA,Macera CA,Ainsworth BE,Kirtland KA,Reis JP,et al.Descriptive epidemiology of pedometer-determined physical activity.Med Sci Sports Exerc2004;36:1567-73.
猜你喜欢
杂志排行

Journal of Sport and Health Science的其它文章
- Research highlights from the Status report for step it up!The surgeon general’s call to action to promote walking and walkable communities
- Environments favorable to healthy lifestyles:A systematic review of initiatives in Canada
- The built environment correlates of objectively measured physical activity in Norwegian adults:A cross-sectional study
- The association of various social capital indicators and physical activity participation among Turkish adolescents
- Matched or nonmatched interventions based on the transtheoretical model to promote physical activity.A meta-analysis of randomized controlled trials
- Collegiate athletes’mental health services utilization:A systematic review of conceptualizations,operationalizations,facilitators,and barriers