Footfall patterns of a runner with an Achilles tendon rupture
2018-01-08DnielJndckDvidZhrdnikRomnFrnJroslvUchytilJosephHmillb
Dniel Jndck*,Dvid Zhrdnik Romn FrnJroslv UchytilJoseph Hm illb
a Department of Human Movement Studies,Human Motion Diagnostic Center,University of Ostrava,Ostrava 70200,Czech Republic
b Department of Kinesiology,University of Massachusetts,Amherst,MA 01003,USA
1.Introduction
Humans are one of the few animals that utilize multiple footfall patterns.Runners may use a forefoot(FF),a midfoot(MF),or a rearfoot(RF)footfall pattern during running.1,2Hasegawa et al.2reported that approximately 75%of the shod distance runners use an RF pattern and the remaining 25%of the runners use either FF or MF patterns.Only a few studies have reported that some shod runners use different footfall patterns bilaterally.3,4
Larson et al.3reported some cases where runners exhibited a bilateral difference in footfall patterns with an RF pattern mostly on non-dominant foot and an FF pattern on dominant foot.They stated that it is unclear whether these combined landing patterns were a single uncommon footfall pattern sequence or simply a gait asymmetry.Williams et al.4described an elite female runner with combined footfall pattern and speculated that this asymmetry was related to a previous groin injury.The current study is unique in trying to explain the cause of the unusual utilization of the combination of RF and FF footfall patterns.Some authors assume that MF and FF are natural types of footfall pattern that reduce running related injuries5,6and so the change to an FF pattern may be the result of escaping injury to one or the other limbs.
Recently,a runner who used different footfall patterns with each limb during shod running appeared in our laboratory during a research study of recreational runners with a history of Achilles tendon(AT)rupture.There is previous evidence of altered ankle kinematics during stance phase of 2 runners with an elongated AT.7,8Furthermore,AT elongation is a common problem for people with history of rupture.9AT rupture is a devastating injury that causes a functional defici of the plantar fl xors.10In spite of this,humans after AT rupture are still active as recreational athletes.However,running may not be without consequences if the previous musculo-skeletal system injury is associated with a higher incidence of injury among runners.11
The second most common running related injury is Achilles tendinopathy whose incidence is estimated at 9.1%–10.9%of all runners.12To prevent or even “cure”running injuries,it has been suggested that runners should use either an FF or an MF footfall pattern.5,6However,Gruber et al.13reported that an FF foot fall pattern is associated with higher AT forces compared to the RF pattern.Higher AT forces during running may indicate a greater risk of AT injuries.14
Therefore,the purpose of this study was to compare AT loading and AT length of the affected(previous AT rupture)and the unaffected(no injury)AT of a recreational runner who used a combined foot fall pattern(i.e.,FF on unaffected limb and RF on the affected limb).We hypothesized that the affected AT would appear elongated compared to the unaffected AT which could subsequently affect the ankle kinematics while running.7,8In addition,we expected a less loading on the affected AT compared to the unaffected AT.This study offers a unique opportunity to understand the preventive strategies and adaptations of the neuro-muscular system against overloading the weakened structures of the human body.
2.Case report
2.1.Participant
A 41-year-old recreational athlete and professional firema sustained AT rupture on the left limb when he suddenly changed direction during running.The AT was sutured by mini-invasive technique on the day of the injury.Treatment of the subsequent inflammatio required ablation of the proximal part of the calcaneus.From an ultrasonograph examination,a noticeable defect of the calcaneus and insertion of the affected AT was apparent(Fig.1).Further treatment resulted in casting the knee and ankle for 6 weeks and followed by 4months of rehabilitation.Four years later,this individual participated in a research study of running biomechanics of participants with a history of AT rupture.This individual reported that he used an FF footfall pattern when running before the AT injury.The procedure was approved by the University of Ostrava Ethics Committee and the written informed consent was obtained from the participant.
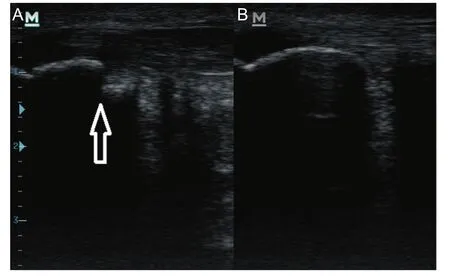
Fig.1.Ultrasonography of the(A)affected and(B)unaffected insertion of the Achilles tendon on calcaneus.
At the time of the research study in which the subject initially completed,the participant’s body mass was 86.5 kg,height1.73m,and body fat 23%of the total body weight.He reported a fift level of physical activity(i.e.,medium intensity exercise at least3 times per week).15The maximum moment of force during the isometric contraction of dorsal and plantar fl xors was measured using a force plate(Fitronic;FitroForce,Bratislava,Slovakia)with the individual’s lower extremity positioned at90°of fl xion at the ankle,knee,and hip.16
The results of the analysis indicated a greater dorsifl xor moment on the repaired AT limb versus the unaffected AT(difference11N·m,effect size(ES)> 0.8)and a weaker plantar fl xor moment on the affected limb(difference 41N·m,ES>0.8)compared to the repaired AT limb.The runner reported no pain or restrictions in activity shown by the Foot and Ankle Outcome Score(FAOS).17However the Achilles tendon Total Rupture Score(ATRS)was rated at44,causing the runner to feel limited during running.18
2.2.Instrumentation,protocol,and statistics
Two force plates(Kistler,9286AA and 9281CA;Kistler Instrumente AG,Winterthur,Switzerland)were used to collect ground reaction force data.The force platforms were placed in a17m long runway and were situated flus with the floo.Data were sampled at a frequency of 1200Hz.Retro-reflect ve markers were placed on the subject prior to data collection according to the protocol suggested by Hamill and colleagues.19Calibration markers were placed bilaterally on the lateral and medial malleoli,the medial and lateral femoral condyles,the greater trochanter,and on the shoe/foot over the firs and fift metatarsal heads.Tracking markers were securely positioned to defin the pelvis(iliac crest and posterior superior iliac spine,anterior superior iliac spine),the thighs and shanks(4 lightweight rigid plates holding a quaternion of markers),and the shoe/foot(a triad of markers on the heel over the calcaneus).Kinematics of the foot,leg,thigh,and pelvis were recorded at a frequency of 240 Hz using a motion capture system(Oqus100;Qualisys AB,Göteborg,Sweden).
The participant completed a 5m in warm-up prior to data collection.Subsequently,he completed 5 acceptable trials over the force platforms at a speed of 3.2m/s(±5%)in each of 2 conditions:(1)running shod(Mizuno Crusader;Mizuno Corp.,Osaka,Japan)and(2)running barefoot.The barefoot condition was included to determine that the individual was capable of running with an FF pattern.The difference in the dependent variables was evaluated using ES,which was calculated and interpreted as trivial with ES≤0.2,small with ES >0.2 and≤0.50,medium with ES >0.5 and ≤0.80,and large with ES>0.8.20
2.3.Footfall pattern
This individual clearly used an RF pattern on affected and an FF pattern on unaffected foot when shod(Figs.2A and 3 and Table 1).During barefoot running,he used only an FF footfall pattern(Fig.2E).However,during barefoot running,the ankle plantar fl xion angle on the unaffected lower extremity was different from that on the affected limb(Table 1).While still using an FF/MF pattern,the plantar fl xion angle on the affected limb was much reduced and may indicate a transition to a less FF and more MF pattern.
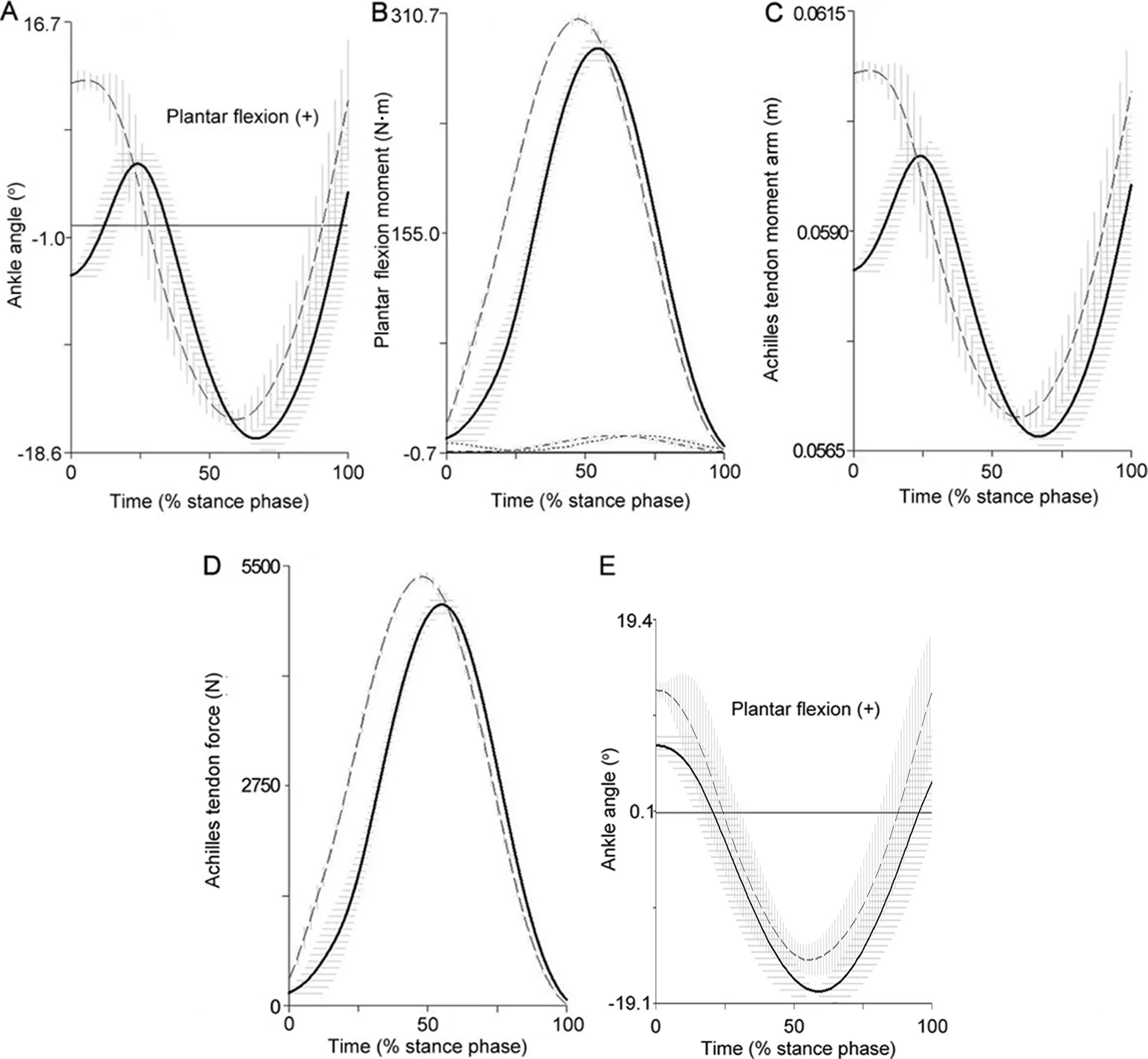
Fig.2.Comparison of the affected(solid curve)and unaffected(dashed curve)ankle joint kinematics and kinetics during stance phase of shod running(A–D)and barefoot running(E)(n=5 trials,mean±SD).(A,E)The angle in the ankle joint;(B)Active moment of plantar fl xors and passive ankle moments on the unaffected(dot dash)and the affected(with dots);(C)Achilles tendon moment arm;and(D)Achilles tendon force.
2.4.AT length,force,and loading rate
AT length was measured by a non-invasive method that combined both ultrasonography and an infrared camera system.21AT length was define as the distance between the gastrocnemius musculotendinous junction and the calcaneal osteotendinous junction.7There was no difference between the length of the affected and the unaffected AT(Table 2).
Visual 3D(C-motion,Rockville,MD,USA)was used to determine the AT force.To estimate AT moment arm(Fig.2C),we used a regression equation.22An estimate of the passive ankle moment was subtracted from the net ankle moment to determine the active plantar fl xion moment(Fig.2B).23The AT force was estimated as the active plantar fl xion moment divided by AT moment arm during the stance phase(Fig.2D).During shod running,the maximal AT force was348N lower in the affected AT versus the unaffected AT.The AT loading rate followed a similar trend with a difference of 7846 N/s(Table 2,Fig.2D).During barefoot running,the affected maximal AT force was 221N greater than unaffected maximal AT force.Again there was a similar trend for the AT loading rate with a difference of 1651N/s between the affected and the unaffected AT loading rates.

Fig.3.Footfall patterns of a shod runner with an Achilles tendon rupture during the instant of initial contact within a single running cycle.Note(A)the rearfoot footfall pattern on the affected foot and(B)the forefoot/midfoot footfall pattern on the unaffected foot.

Table1 Comparison of ankle angle during initial contact on the affected and unaffected lower extremity while running in shoes(SH)and barefoot(BF).
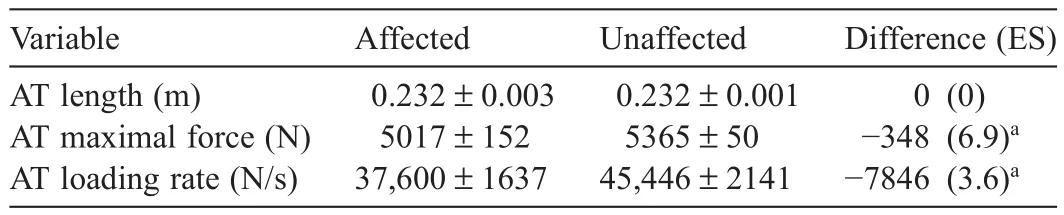
Table2 Comparison of AT length and loading on the affected and unaffected lower extremity while running in shoes.
3.Discussion
In this case report,we described a unique runner who used different footfall patterns on the AT ruptured limb and the unaffected AT in a single gait cycle during shod running.We hypothesized that the affected AT would be elongated which subsequently could affect the kinematics of the ankle joint movement during stance phase of running.Contrary to our hypothesis,AT length did not differ between limbs.Further,we hypothesized that the affected AT may have altered loading during running.The individual in this report showed an asymmetry during shod running using an RF pattern on the affected AT and an FF/MF pattern on the unaffected AT.He showed an AT loading asymmetry with a greater AT load on the FF footfall pattern or unaffected side.In contrast,during barefoot running,when this individual used only FF/MF pattern,loading of affected AT was greater than on the unaffected side.
Repetitive tendon loading,such as that experienced during distance running,may initiate production of prostaglandin E2 which can result in degenerative changes within the tendon.24,25Sinclair14advocated that barefoot running(i.e.,with an FF pattern)may not be appropriate for runners who are predisposed to AT pathology.He showed increased AT loading during barefoot running compared to shod running in healthy individuals.Gruber and associates13reported that there was decreased loading of the AT in the loading phase during an RF pattern.On the other hand,the AT was loaded throughout the support phase in anMF/FF footfall pattern.Thus,an RF footfall pattern on the affected side(i.e.,the previously injured AT)during shod running could be protective mechanism against chronic injuries of the AT with history of rupture.
Alternatively,based on the isometric measurements,there was a weaker plantar fl xor moment on the affected limb indicating that the asymmetric loading may be due to differences in the capability of the muscles rather than the use of RF loading as a “protective mechanism”.However,the runner used the FF/MF footfall pattern when barefoot(Fig.2E).This provides support for the fact that the participant had sufficien plantar fl xion strength for FF/MF running but chose not to do during shod running.
Currently,the individual from this study does not feel any pain bu the feels limited during running.Despite the subjective difficulties 4 years after the AT surgery,he performs physical activity of medium intensity 3 times a week and carries on his physically demanding profession as a firefight.The participant self-reported the use of an FF/MF footfall pattern before measurement.We identifie a mixed footfall pattern after the measurement of shod running.The low number of FF/MF distance runners in the population2could bean explanation for the rare occurrence of switching the footfall pattern from FF/MF to RF on the affected lower extremity.Running with the FF/MF footfall pattern on both lower extremities when barefoot(Fig.2E)provides support for our hypothesis of the FF/MF footfall pattern bilaterally before injury.
In conclusion,we described a unique case of a physically active individual who uses different footfall patterns bilaterally when running.This asymmetry in footfall patterns may be a result of the AT loading on the leg with a history of AT rupture.Different footfall patterns could affect the AT forces13and may be an adaptation to the weakening of osteotendinous junction.However,the asymmetry was not related to AT elongation.These results suggest that an RF footfall pattern may be an adaptation to reduce the loading on the AT that was previously injured.This extreme case of combined footfall pattern can contribute to an understanding of the reasons for the strategy of footfall pattern in general.
Acknowledgment
This research has been supported by a grant from the University of Ostrava(SGS 6148),Czech Republic.
Authors’contributions
DJ carried out the measurement,participated in the biomechanical analysis and manuscript drafting,performed the statistical analysis,conceived of the study and participated in its design;JU,RF,and DZ carried out the measurement;JH participated in the biomechanical analysis,conceived of the study,participated in its design and coordination,and helped draft the manuscript.All authors have read and approved the fina version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
1.Gruber AH,Boyer K,Silvernail JF,Hamill J.Comparison of classificatio methods to determine footfall pattern.Footwear Sci 2013;5(Suppl.1):S103–4.
2.Hasegawa H,Yamauchi T,Kraemer WJ.Foot strike patterns of runners at the 15-km point during an elite-level half marathon.J Strength Cond Res 2007;21:888–93.
3.Larson P,Higgins E,Kaminski J,Decker T,Preble J,Lyons D,et al.Foot strike patterns of recreational and sub-elite runners in a long-distance road race.J Sports Sci2011;29:1665–73.
4.Williams KR,Cavanagh PR,Ziff JL.Biomechanical studies of elite female distance runners.Int J Sports Med 1987;8:107–18.
5.Lieberman DE,Venkadesan M,Werbel WA,Daoud AI,D’Andrea S,Davis IS,et al.Foot strike patterns and collision forces in habitually barefoot versus shod runners.Nature 2010;463:531–5.
6.Daoud AI,Geissler GJ,Wang F,Saretsky J,Daoud YA,Lieberman DE.Foot strike and injury rates in endurance runners:a retrospective study.Med Sci Sports Exerc 2012;44:1325–34.
7.Silbernagel KG,Willy R,Davis I.Preinjury and postinjury running analysis along with measurements of strength and tendon length in a patient with a surgically repaired Achilles tendon rupture.J Orthop Sports Phys Ther 2012;42:521–9.
8.Jandacka D,Zahradnik D,Foldyna K,Hamill J.Running biomechanics in a long-term monitored recreational athlete with a history of Achilles tendon rupture.BMJ Case Rep 2013;doi:10.1136/bcr-2012-007370
9.Rosso C,Vavken P,Polzer C,Buckland DM,Studler U,Weisskopf L,et al.Long-term outcomes of muscle volume and Achilles tendon length after Achilles tendon ruptures.Knee Surg Sports Traumatol Arthrosc 2013;21:1369–77.
10.Bressel E,Larsen BT,McNair PJ,Cronin J.Ankle joint proprioception and passive mechanical properties of the calf muscles after an Achilles tendon rupture:a comparison with matched controls.Clin Biomech(Bristol,Avon)2004;19:284–91.
11.Saragiotto BT,Yamato TP,Hespanhol Junior LC,Rainbow MJ,Davis IS,Lopes AD.What are the main risk factors for running-related injuries?Sports Med 2014;44:1153–63.
12.Lopes AD,Hespanhol Júnior LC,Yeung SS,Costa LO.What are the main running-related musculoskeletal injuries?A systematic review.Sports Med 2012;42:891–905.
13.Gruber AH,Umberger BR,Jewell C,DelPilar S,Ham ill J.Achilles tendon forces in forefoot and rearfoot running.In:2011 Annual Meeting of American Society of Biomechanics.Long Beach,CA,USA.August10–13,2011.
14.Sinclair J.Effects of barefoot and barefoot inspired footwear on knee and ankle loading during running.Clin Biomech (Bristol,Avon)2014;29:395–9.
15.Grimby G.Physical activity and muscle training in the elderly.Acta Med Scand Suppl 1986;711:233–7.
16.Moraux A,Canal A,Ollivier G,Ledoux I,Doppler V,Payan C,et al.Ankle dorsi-and plantar-fl xion torques measured by dynamometry in healthy subjects from 5 to 80 years.BMC Musculoskelet Disord 2013;14:104.doi:10.1186/1471-2474-14-104
17.Roos EM,Brandsson S,Karlsson J.Validation of the foot and ankle outcome score for ankle ligament reconstruction.Foot Ankle Int 2001;22:788–94.
18.Nilsson-Helander K,Thomeé R,Silbernagel KG,Thomeé P,Faxén E,Eriksson BI,et al.The Achilles tendon Total Rupture Score(ATRS):development and validation.Am J Sports Med 2007;35:421–6.
19.Hamill J,Selbie WS,Kepple TM.Three-dimensional Kinematics.In:Robertson DGE,Caldwell GE,Ham ill J,Kamen G,Whittlesey SN,editors.Research methods in biomechanics.2nd ed.Champaign,IL:Human Kinetics Publishers;2013.p.35–60.
20.Cohen J.Statistical power analysis for the behavioral sciences.Hillsdale,NJ:Erlbaum;1988.
21.Rees JD,Lichtwark GA,Wolman RL,Wilson AM.The mechanism for effica y of eccentric loading in Achilles tendon injury:an in vivo study in humans.Rheumatology(Oxford)2008;47:1493–7.
22.Self BP,Paine D.Ankle biomechanics during four landing techniques.Med Sci Sports Exerc 2001;33:1338–44.
23.Riener R,Edrich T.Identificatio of passive elastic jointmoments in the lower extremities.J Biomech 1999;32:539–44.
24.Khan MH,Li Z,Wang JH.Repeated exposure of tendon to prostaglandin-E2 leads to localized tendon degeneration.Clin J Sport Med 2005;15:27–33.
25.Zhang J,Wang JH.Production of PGE2increases in tendons subjected to repetitive mechanical loading and induces differentiation of tendon stem cells into non-tenocytes.J Orthop Res 2010;28:198–203.
杂志排行

Journal of Sport and Health Science的其它文章
- The effects of aerobic exercise training on oxidant-antioxidant balance, neurotrophic factor levels, and blood-brain barrier function in obese and non-obese men
- Three-dimensional impact kinetics with foot-strike manipulations during running
- Shock attenuation,spatio-temporal and physiological parameter comparisons between land treadmill and water treadmill running
- Tribulus terrestris extracts alleviate muscle damage and promote anaerobic performance of trained male boxers and its mechanisms:Roles of androgen,IGF-1,and IGF binding protein-3
- Heart rate variability to assess ventilatory thresholds in professional basketball players
- The influenc of different exercise intensities on kicking accuracy and velocity in soccer players