多项无创诊断指数评估慢性乙型肝炎肝纤维化的准确性比较*
2017-12-07张志侨黄丽雯陈永鹏
张志侨,黄丽雯,陈永鹏
多项无创诊断指数评估慢性乙型肝炎肝纤维化的准确性比较*
张志侨,黄丽雯,陈永鹏
目的探讨10种无创诊断肝纤维化指数对慢性乙型肝炎患者肝纤维化诊断的准确性。方法回顾性分析2008年1月~2014年12月期间行肝穿刺活检术诊断的1362例CHB患者的临床资料,分别计算不同的指数得分。以受试者工作特征曲线下面积(AUROC)评价各指数的准确性,采用DeLong法对各指数诊断的准确性进行比较。结果本组资料显示,诊断显著肝纤维化(≥S2)的AUROC依次为:S指数(0.745)、GPRI(0.736)和APRI(0.681);诊断肝硬化(S4)的 AUROC 依次为:S指数(0.716)、FIB-4(0.708)和 GPRI(0.707);S指数诊断肝硬化时,其截断点为0.03,敏感度为98.8%,阴性预测值为97.0%,阴性似然比为0.14;截断点为1.5的特异度为99.5%,阳性预测值为70.0%,阳性似然比为10.1;S指数诊断显著肝纤维化时,其截断点为0.89,特异度为99.5%,阳性预测值为98.5%,阳性似然比为11.5;截断点为0.02的敏感度为97.7%,阴性预测值为40.0%,阴性似然比为0.26。结论在10个无创诊断指数中,S指数的诊断性能相对最佳,值得进一步研究。
乙型肝炎;肝纤维化;常规血清指标;无创诊断指数
评估慢性乙型肝炎(chronic hepatitis B,CHB)患者肝纤维化程度的意义在于筛选显著肝纤维化,确定抗病毒治疗指征,以阻止肝硬化的发生,或筛选肝硬化以确定监测肝硬化并发症及肝癌的发生。肝活检是评价肝纤维化的金标准,但其临床应用受限于有创性和采样误差[1,2]。瞬时弹性成像对肝纤维化有较好的诊断价值,然而,其临床应用也存在局限性,如肝组织坏死性炎症和胆汁淤积可能增加肝脏硬度值而导致假阳性[3,4],腹水、肥胖和肋间隙过于狭窄容易导致检测失败[5]。目前,国内外已有多个无创诊断指数用于CHB患者肝纤维化的诊断,如γ-谷氨酰转肽酶/血小板比值(γ-glutamyltranspeptidase to platelet ratio index,GPRI)[6]、Pohl 评分[7]、肝纤维化4因子指数(fibrosis index based on the four factors,FIB-4)[8]、天冬氨酸氨基转移酶 /血小板比值(aspartate aminotransferase to platelet ratio index,APRI)[9]、天冬氨酸氨基转移酶/丙氨酸氨基转移酶比值(aspartate aminotransferase to alanine aminotransferase ratio,AAR)[10]、S 指数[11]、Mohamadnejad指数[12]、天冬氨酸氨基转移酶/血小板/γ-谷氨酰转肽酶/甲胎蛋白指数(aspartate aminotransferase/platelet/GGT/AFP,APGA)[13]、年龄 /血小板指数(age to platelet index,API)[14]和 AAR/血小板评分(AAR/platelet score,AARP)等[15]。然而,这些无创诊断指数在CHB患者中的诊断准确性尚未明确。本研究旨在比较分析上述指数对CHB患者肝纤维化诊断的准确性。
1 资料与方法
1.1 病例来源 2008年1月~2014年12月在南方医科大学顺德医院感染性疾病科住院行肝穿刺活检术的CHB患者,CHB诊断参照2010年中华医学会发布的《慢性乙型肝炎防治指南》的标准[16]。纳入标准:有乙型肝炎或HBsAg阳性史超过6个月。排除标准:1、合并丙型肝炎病毒感染、人类免疫缺陷病毒感染、酒精性肝病、自身免疫性肝病和肝癌;2、标本长度<1.5cm或汇管区<7个。
1.2 肝活检 采用Menghini针双人法一秒钟快速负压抽吸法取材。肝组织用10%甲醛溶液固定,常规石蜡切片,行HE、Gorden-Sweet法、Masson三色和胶原纤维(VG)染色。病理学诊断参照Scheuer诊断标准[17],由1名病理学医师独立复核诊断。合格肝组织定义为标本长度≥1.5 cm,且汇管区≥7个。肝组织炎症分为 G0、G1、G2、G3、G4,纤维化程度分为S0、S1、S2、S3、S4。
1.3 各指数的计算 按照原始文献中给出的方程式[6-15],计算各个指数得分。
1.4 统计分析 应用SPSS l9.0分析软件进行统计分析。对正态分布的计量资料以(±s)表示,两组间比较采用t检验;对非正态分布的计量资料以M(IQR)表示,两组间比较采用两组独立样本非参数秩和(Mann-Whitney U)检验。以受试者工作特征曲线(receiver operating characteristic curve,ROC)下面积(AUROC)评价各指数诊断的准确性。采用DeLong法对各指数诊断的准确性进行比较[18]。采用进展性与非进展性肝纤维化发生率差异(difference between advanced and nonadvanced fibrosis,DANA)法校正不同肝纤维化分期发生率对AUROC的影响[19]。校正AUROC=原始AUROC+0.1056×(2.5-DANA)。诊断显著肝纤维化(S≥2)时,DANA=(S2发生率×2+S3发生率×3+S4发生率×4)(S2发生率+S3发生率+S4发生率)[S1发生率(S0发生率+S1发生率)],诊断肝硬化(S≥4)时,DANA=S4发生率×4/S4发生率-[(S1发生率+S2发生率×2+S3发生率×3)/(S0发生率+S1发生率+S2发生率+S3发生率)]。P<0.05为差异有统计学意义。
2 结果
2.1 临床特征 在入组的1362例CHB患者中,男性1063例(78.0%),女性299例(22.0%);血清HBeAg阳性849例(62.3%);肝纤维化S1期204例(15.0%),S2期 530例 (38.9%),S3期 372例(27.3%),S4期256例(18.8%)。不同肝纤维化分期患者临床特征和各指数得分见表1和表2。
2.2 各指数诊断肝纤维化的效能情况 在统计学上,一般认为AUROC低于0.7的诊断方法准确性较差[20]。各指数诊断肝纤维化的效能见表3(限于篇幅,仅列出AUROC≥0.7的诊断指数)。采用DeLong法对AUROC≥0.7的诊断指数进行比较,结果表明诊断显著肝纤维化时,S指数和GPRI优于其他指数(P<0.05);诊断肝硬化时,S 指数与 FIB-4、GPRI和API的差异均无统计学意义(P>0.05)。在诊断显著肝纤维化和肝硬化时,S指数DANA校正后的AUROC分别为0.823和0.785,其约登指数分别为0.408和0.339,其准确率分别为67.3%和69.3%,高于其他9个指数,提示在10个指数中其诊断性能最佳。
2.3 S指数诊断界值的应用 见表4。
3 讨论
在诊断显著肝纤维化和肝硬化时,S指数DANA校正后AUROC分别为 0.823和 0.785,其AUROC、约登指数和准确率在10个指数中最高。尽管如此,S指数诊断显著肝纤维化和肝硬化的临床价值仍有限,因为S指数>0.89确定显著肝纤维化的患者仅67例(6.3%),S指数<0.03排除肝硬化及S指数≥1.5确定肝硬化的患者也仅93例(8.7%)。
表1 1362例CHB 患者临床特征【%,(±s),M(IQR)】

表1 1362例CHB 患者临床特征【%,(±s),M(IQR)】
非显著肝纤维化(n=204)显著肝纤维化(n=1158) P值 非肝硬化(n=1106)肝硬化(n=256) P值男性 158(77.5) 905(78.2) 0.824 849(76.7) 214(83.6) 0.017年龄(岁) 31.7±9.1 33.9±9.7 0.003 32.7±9.4 37.2±9.9 <0.001谷丙转氨酶(U/L) 52(4,316) 68(2,380) <0.001 68(4,400) 57(2,416) 0.014谷草转氨酶(U/L) 41(14,380) 53(10,399) <0.001 51(8,410) 51(18,399) 0.317谷氨酰转肽酶(U/L) 26(5,330) 55(5,760) <0.001 45(5,649) 77(11,760) <0.001白蛋白(G/L) 45.7±4.5 44.0±5.1 <0.001 44.6±5.0 42.5±5.0 <0.001球蛋白(G/L) 26.0±4.9 27.9±4.1 <0.001 27.2±4.5 29.3±5.3 <0.001总胆红素(μmol/L) 14(4.9,43.1) 15(3,134.0) 0.068 14.6(3,134.0) 16.7(4.0,84.0) <0.001白细胞(×109/L) 5.7±1.5 5.6±1.7 0.133 5.6±1.6 5.5±1.9 0.350血红蛋白(G/L) 142.6±21.3 143.0±16.3 0.803 143.5±17.3 140.5±16.0 0.012血小板(×109/L) 196.0±49.7 178.4±57.6 <0.001 188.2±55.2 150.0±53.4 <0.001尿素氮(μmol/L) 4.4±1.3 4.3±1.2 0.115 4.3±1.2 4.2±1.2 0.165肌酐(μmol/L) 77.4±18.3 76.1±24.4 0.447 76.1±18.3 77.2±39.0 0.506血糖(mmol/L) 4.6±0.9 4.8±1.4 0.113 4.7±1.2 5.0±1.8 0.025总胆固醇(mmol/L) 4.4±1.0 4.3±1.0 0.096 4.3±1.0 4.2±0.9 0.033甘油三酯(mmol/L) 1.0±0.7 1.1±0.7 0.052 1.1±0.7 1.1±0.7 0.304 HBV DNA(lg copies/ml) 4.4±3.0 4.5±2.8 0.884 4.7±2.7 3.6±2.8 <0.001 HBeAg阳性 124(60.8) 725(62.6) 0.6207 17(64.8) 132(51.6) <0.001抗病毒治疗 47(23.0) 256(22.1) 0.9752 34(21.2) 69(27.0) 0.045
表2 不同肝纤维化分期患者无创诊断指数得分【(±s),M(IQR)】比较
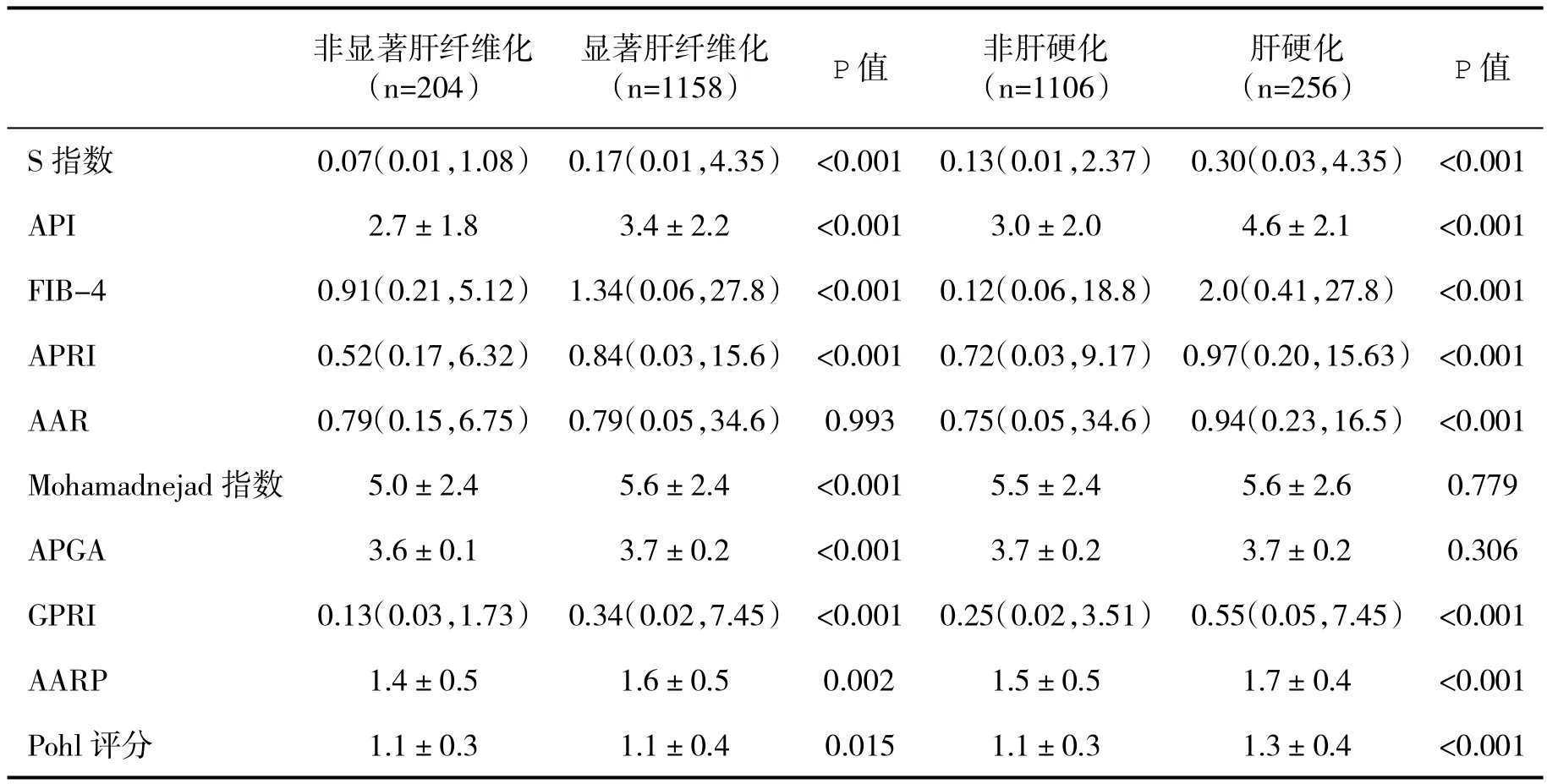
表2 不同肝纤维化分期患者无创诊断指数得分【(±s),M(IQR)】比较
非显著肝纤维化(n=204)显著肝纤维化(n=1158) P值 非肝硬化(n=1106)肝硬化(n=256) P值S 指数 0.07(0.01,1.08) 0.17(0.01,4.35) <0.001 0.13(0.01,2.37) 0.30(0.03,4.35) <0.001 API 2.7±1.8 3.4±2.2 <0.001 3.0±2.0 4.6±2.1 <0.001 FIB-4 0.91(0.21,5.12) 1.34(0.06,27.8) <0.001 0.12(0.06,18.8) 2.0(0.41,27.8) <0.001 APRI 0.52(0.17,6.32) 0.84(0.03,15.6) <0.001 0.72(0.03,9.17) 0.97(0.20,15.63) <0.001 AAR 0.79(0.15,6.75) 0.79(0.05,34.6) 0.993 0.75(0.05,34.6) 0.94(0.23,16.5) <0.001 Mohamadnejad指数 5.0±2.4 5.6±2.4 <0.001 5.5±2.4 5.6±2.6 0.779 APGA 3.6±0.1 3.7±0.2 <0.001 3.7±0.2 3.7±0.2 0.306 GPRI 0.13(0.03,1.73) 0.34(0.02,7.45) <0.001 0.25(0.02,3.51) 0.55(0.05,7.45) <0.001 AARP 1.4±0.5 1.6±0.5 0.002 1.5±0.5 1.7±0.4 <0.001 Pohl评分 1.1±0.3 1.1±0.4 0.015 1.1±0.3 1.3±0.4 <0.001
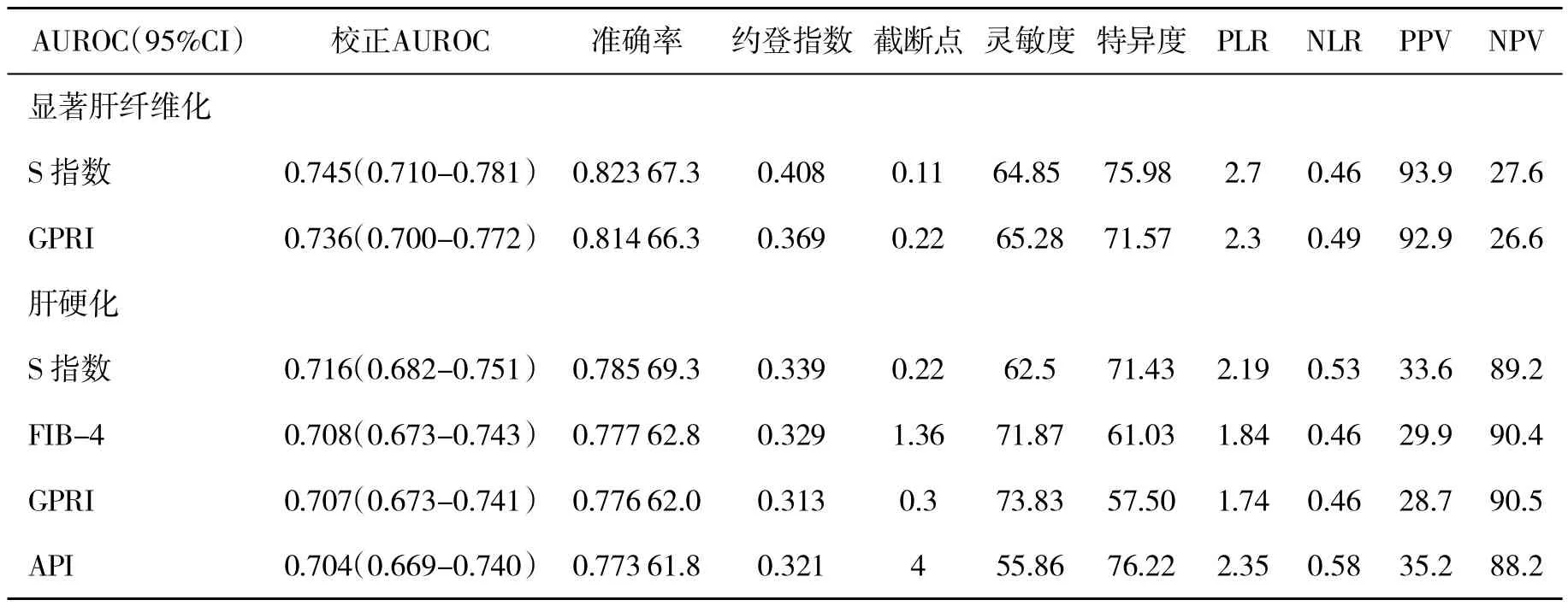
表3 不同无创诊断指数诊断肝纤维化的效能比较
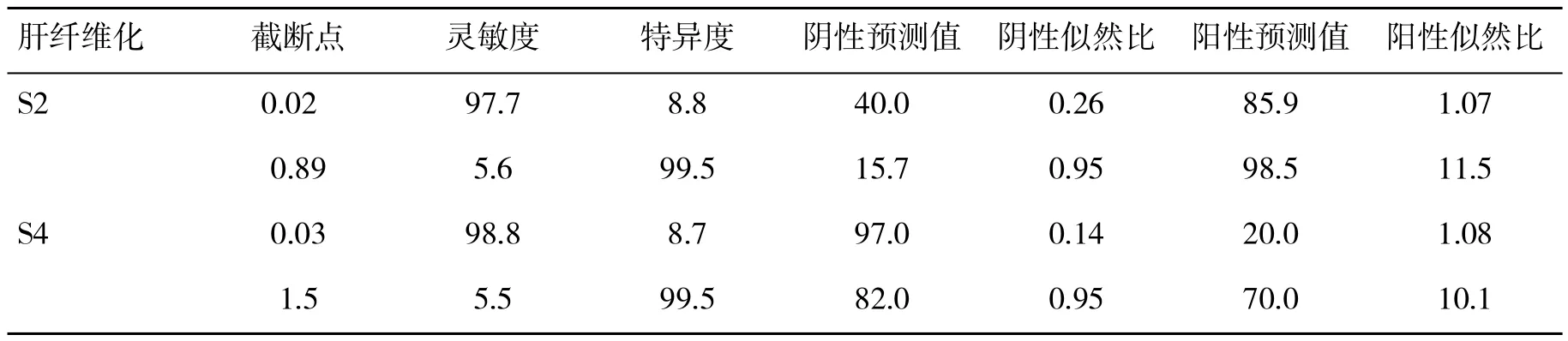
表4 S指数诊断肝纤维化的效能评价
Zhou K[11]报道,在诊断显著肝纤维化和肝硬化时,S指数和 APRI的 AUROC分别为 0.812对0.717、0.890对 0.790,S指数的诊断准确性优于APRI。Basar O[22]报道,在诊断显著肝纤维化时,S指数、FIB-4和 APRI的 AUROC分别为 0.669、0.741和0.669,诊断肝硬化时的AUROC分别为0.792、0.768 和 0.741。Zeng XH[23]报道,在诊断显著肝 纤 维 化 时 ,S 指 数 、GPRI、FIB-4、APRI、API 和AAR 的 AUROC 依次为 0.726、0.726、0.621、0.619、0.580和0.495。本研究发现在诊断显著肝纤维化和肝硬化时,S指数DANA校正后AUROC、约登指数和准确率高于其他9个无创指数。本研究和既往多个研究中S指数诊断肝纤维化的AUROC存在一定的差异,可能与下列因素有关:不同研究人群肝纤维化发生率不同可能影响了准确性的评价以及不同研究人群的基线特征存在差异。由于不同肝纤维化分期发生率可能影响诊断指数诊断准确性的评价,各研究的结果不宜进行简单的横向比较,考虑应对不同肝纤维化分期进行校正后再进行横向比较分析。
本研究对S指数诊断显著肝纤维化和肝硬化的截断点作了初步探讨。然而,其诊断效能差强人意。既往诊断试验研究多采用约登指数确定诊断界值。Jaeschke R et al[21]指出,在评价诊断试验性能时,诊断界值似然比对确定诊断结果很重要:一方面,似然比不受研究人群病例的影响,有利于不同研究之间横向比较;另一方面,PLR接近10或NLR接近0.1常常可结论性地作出确定或排除诊断,而PLR 2~5或NLR 0.5~0.2确定或排除诊断的可能性小。本文根据约登指数确定的S指数诊断界值,确定诊断的PLR 1.91~2.70,排除诊断的NLR 0.46~0.53,作出结论性诊断的可能性均较低,而根据PLR接近于10或NLR接近0.1可作出结论性诊断的比例则低于10%。
本研究为单中心研究,研究样本量高达1362例,研究结果可信度高。虽然S指数是上述10个无创指数中诊断性能最高的指数,但其对不同程度肝纤维化的诊断价值仍较低。联合多个无创指数可提高无创指数对肝纤维化诊断的准确性,与病理诊断价值趋近,提示不同诊断指数之间的联合应用有助于提高诊断效能。我们近期研究显示,在诊断界值PLR接近10或NLR接近0.1情况下,逐步应用不同无创诊断方法可提高诊断性能[24],进一步研究可尝试构建新的诊断指数或采用多个指数逐步联合应用,以期提高诊断效能。
[1]Shackel NA,McCaughan GW.Liver biopsy:is it still relevant.Intern Med J,2006,36:689-691.
[2]Emanuele E.Is biopsy always necessary toward a clinico-laboratory approach for diagnosing nonalcoholic steatohepatitis in obesity.Hepatology,2008,48:2086-2087.
[3]Chen YP,Peng J,Hou JL.Non-invasive assessment of liver fibrosis in patients with chronic hepatitis B.Hepatol Int,2013,7(2):356-368.
[4]Liang XE,Chen YP,Zhang Q,et al.Dynamic evaluation paralleled with bilirubin and ALT normalization to improve diagnostic accuracy of FibroScan in patients with hepatitis B exacerbation.J Viral Hepat,2011,18:884-891.
[5]Caste'ra L,Foucher J,Bernard PH,et al.Pitfalls of liver stiffness measurement:a 5-year prospective study of 13,369 examinations.Hepatology,2010,51:828-835.
[6]Vardar R,Vardar E,Demiri S,et al.Is there any non-invasive marker replace the needle liver biopsy predictive for liver fibrosis,in patients with chronic hepatitis Hepatogastroenterology,2009,56:1459-1465.
[7]Pohl A,Behling C,Oliver D,et al.Serum aminotransferase levels and plateletcounts aspredictorsofdegree offibrosisin chronic hepatitis C virus infection.Am J Gastroenterol,2001,96(11):3142-3146.
[8]Valet-Pichard A,Mallet V,Nalpas B,et al.FIB-4:an inexpensive and accurate marker of fibrosis in HCV infection.comparison with liver biopsy and Fibrotest. Hepatology,2007,46(1):32-36.
[9]Wai CT,Greenson JK,Fontana RJ,et al.A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C.Hepatology,2003,38:518-526.
[10]Williams AL,Hoofnagle JH.Ratio of serum aspartate to alanine aminotransferase in chronic hepatitis.Relationship to cirrhosis.Gastroenterology,1988,95(3):734-739.
[11]Zhou K,Gao CF,Zhao YP,et al.Simpler score of routine laboratory tests predicts liver fibrosis in patients with chronic hepatitis B.J Gastroenterol Hepatol,2010,25(9):1569-1577.
[12]Mohamadnejad M,Montazeri G,Fazlollahi A,et al.Noninvasive markers of liver fibrosis and inflammation in chronic hepatitis B-virusrelated liverdisease.Am JGastroenterol,2006,101(11):2537-2545.
[13]Fung J,Lai CL,Fong DY,et al.Correlation of liver biochemistry with liver stiffness in chronic hepatitis B and development of a predictive model for liver fibrosis.Liver Int,2008,28:1408-1416.
[14]Poynard T,Bedossa P.Age and platelet count:a simple index for predicting the presence of histological lesions in patients with antibodies to hepatitis C virus. METAVIR and CLINIVIR Cooperative Study Groups.J Viral Hepat,1997,4:199-208.
[15]Lee IC,Chan CC,Huang YH,et al.Comparative analysis of noninvasive models to predict early liver fibrosis in hepatitis B e antigen-negative chronic hepatitis B.J Clin Gastroenterol,2011,45(3):278-285.
[16]中华医学会肝病学分会和感染病学分会.慢性乙型肝炎防治指南(2010年版).实用肝脏病杂志,2011,14(2):81-89.
[17]European Association for the study of the liver.EASL clinical practice guidelines:management of chronic hepatitis B.J Hepatol,2009,50:227-242.
[18]Poynard T,Halfon P,Castera L,et al.Standardization of ROC curve areas for diagnostic evaluation of liver fibrosis markers based on prevalences of fibrosis stages.Clin Chem,2007,53:1615-1622.
[19]Poynard T,Halfon P,Castera L,et al.Standardization of ROC curve areas for diagnostic evaluation of liver fibrosis markers based on prevalences of fibrosis stages.Clin Chem,2007,53:1615-1622.
[20]Swets JA.Measuring the accuracy of diagnostic systems.Science,1988,240:1285-1293.
[21]Jaeschke R,Guyatt GH,Sackett DL,et al.Users'guides to the medical literture III.How to use an article about a diagnostic test B.What are the results and will they help me in caring for my patients.JAMA,1994,271:703-707.
[22]Basar O,Yimaz B,Ekiz F,et al.Non-invasive tests in prediction of liver fibrosis in chronic hepatitis B and comparison with post-antiviral treatment results.Clin Res Hepatol Gastroenterol,2013,37(2):152-158.
[23]Zeng X,Xu C,He D,et al.Performance of several simple,noninvasive models for assessingsignificant liverfibrosis in patients with chronic hepatitis B.Croat Med J,2015,56(3):272-279.
[24]Liang XE,Zhong C,Huang L,et al.Optimization of hepatitis B cirrhosis detection by stepwise application of transient elastography and routine biomarkers.J Gastroenterol Hepatol,2017,32:459-465.
(收稿:2017-04-21)
(本文编辑:陈从新)
Evaluation of liver fibrosis by non-invasive diagnostic indexes in patients with chronic hepatitis B
Zhang Zhiqiao,Huang Liwen,Chen Yongpeng. Department of Infectious Disease&Hepatology Unit,Nanfang Hospital,Southern Medical University,Guangzhou 510515,Guangdong Province
Chen Yongpeng,E-mail:cyp@smu.edu.cn
ObjectiveTo evaluate the diagnostic efficacy of ten noninvasive indexes for liver fibrosis in patients with chronic hepatitis B.MethodsThe data of 1362 patients with chronic hepatitis B between January 2008 and December 2014 were collected and statistically analyzed.ResultsFor significant fibrosis diagnosis,the best AUROCs of S index,GPRI and APRI were 0.745,0.736 and 0.681,respectively;For cirrhosis diagnosis,the best AUROCs were S index(0.716),FIB-4 (0.708)and GPRI 0.707,respectively;In diagnosing liver cirrhosis,the cut-off value of S index was 0.03,with a sensitivity of 98.8%,a negative predictive value of 97.0% and a negative likelihood ratio of 0.14;and the cut-off value 1.5 showed a specificity of 99.5%,a positive predictive value of 70.0%and a positive likelihood ratio of 10.1;For significant fibrosis diagnosis,the cut-off value of S index was 0.89,with a specificity of 99.5%,a positive predictive value of 98.5%and a positive likelihood ratio of 11.5;the cut-off value 0.02 showed a sensitivity of 97.7%,a negative predictive value of 40.0%and a negative likelihood ratio of 0.26.Conclusions S index has a relatively good accuracy and is superior to other nine noninvasive diagnostic indexes in diagnosing significant liver fibrosis in patients with chronic hepatitis B.
Hepatitis B;Liver fibrosis;Routine serum biomarker;Noninvasive indexes
10.3969/j.issn.1672-5069.2017.06.014
广东省卫生与计划生育委员会科研资助项目(编号:A2016450/A2013695)
510515广州市 南方医科大学南方医院感染内科
张志侨,男,37岁,大学本科,副主任医师。主要从事乙型肝炎和肝硬化临床研究。E-mail:sdgrxjbk@163.com
陈永鹏,E-mail:cyp@smu.edu.cn