Xingnao Kaiqiao needling method for acute ischemic stroke: a meta-analysis of safety and efficacy
2017-09-04ZhixinYangJiahongXieDingdingLiu
Zhi-xin Yang, Jia-hong Xie, Ding-ding Liu
1 Department of Traditional Chinese Medicine, Chengde Medical University, Chengde, Hebei Province, China
2 Key Laboratory of Traditional Chinese Medicine Research and Development, Institute of Traditional Chinese Medicine, Chengde Medical University, Chengde, Hebei Province, China
3 School of Traditional Chinese Medicine, North China University of Science and Technology, Tangshan, Hebei Province, China
Xingnao Kaiqiao needling method for acute ischemic stroke: a meta-analysis of safety and efficacy
Zhi-xin Yang1,*, Jia-hong Xie2, Ding-ding Liu3
1 Department of Traditional Chinese Medicine, Chengde Medical University, Chengde, Hebei Province, China
2 Key Laboratory of Traditional Chinese Medicine Research and Development, Institute of Traditional Chinese Medicine, Chengde Medical University, Chengde, Hebei Province, China
3 School of Traditional Chinese Medicine, North China University of Science and Technology, Tangshan, Hebei Province, China
How to cite this article:Yang ZX, Xie JH, Liu DD (2017) Xingnao Kaiqiao needling method for acute ischemic stroke: a meta-analysis of safety and ef fi cacy. Neural Regen Res 12(8):1308-1314.
OBJECTIVE: To evaluate the ef f ectiveness and safety of theXingnao Kaiqiaoneedling method for treating acute ischemic stroke.
DATA SOURCES: We retrieved relevant randomized controlled trials involvingXingnao Kaiqiaoacupuncture for treatment of acute ischemic stroke. The China National Knowledge Infrastructure, Weipu Information Resources System, Wanfang Medical Data System, Chinese Biomedical Literature Database, Cochrane Library, and PubMed were searched from June 2006 to March 2016.
DATA SELECTION: We analyzed randomized and semi-randomized clinical controlled trials that comparedXingnao Kaiqiaoacupuncture with various control treatments, such as conventional drugs or other acupuncture therapies, for treatment of acute ischemic stroke.e quality of articles was evaluated according to the Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1), and the study was carried out using Cochrane system assessment methods. RevMan 5.2 was used for the meta-analysis of the included studies.
RESULTS: Twelve studies met the inclusion criteria for this review.e meta-analysis showed that betweenXingnao Kaiqiaoacupuncture and the control treatment,Xingnao Kaiqiaoacupuncture reduced the disability rate [risk ratio (RR) = 0.51, 95% conf i dence interval (CI) = 0.27–0.98,z= 2.03,P< 0.05], elevated the activities of daily living (weighted mean dif f erence = 12.23, 95%CI: 3.66–20.08,z= 2.80,P< 0.005), and had greater clinical ef fi cacy (RR= 1.61, 95%CI: 1.23–2.09,z= 3.53,P< 0.0004). However, there was no signif i cant dif f erence in mortality rate (RR= 0.61, 95%CI: 0.15–2.45,z= 0.70,P> 0.05).
CONCLUSION: TheXingnao Kaiqiaoneedling method is effective and safe for acute ischemic stroke. However, there was selective bias in this study, and the likelihood of measurement bias is high.us, more high-quality randomized controlled trials are needed to provide reliable evidence of the ef fi cacy and safety ofXingnao Kaiqiaoacupuncture in the treatment of acute ischemic stroke.
nerve regeneration; Xingnao Kaiqiao needling method; acute ischemic stroke; meta-analysis; systematic review; activities of daily living; Barthel index; mortality; disability rate; clinical ef fi cacy; neural regeneration
Introduction
Stroke is a leading cause of death and long-term disability in adults worldwide (Goldstein et al., 2011; Cheng et al., 2013). More than 80% of strokes originate from ischemic damage to the brain caused by an acute reduction in the blood supply, causing neurological def i cits and functional impairment (Przybylowski et al., 2014).e acute and subacute stages are the most important periods in the course of stroke rehabilitation (Lackland et al., 2014).
Acupuncture has been used to treat stroke in China for more than 1,000 years; it has also been recommended by the World Health Organization (2002). Acupuncture has been widely used to improve motor, sensation, language, and other neurological functions in patients with stroke (Ramee and White, 2014). TheXingnao Kaiqiao(XNKQ) needling method is a well-recognized element of acupuncture in China.e XNKQ needling method is based on long-term clinical experiments and was developed in 1972 by Professor Xuemin Shi, an academician of the Chinese Academy of Engineering (Shi, 1998).
Clinical experience and some animal studies have indicated that the XNKQ needling method is signif i cantly ef f ective and safe in stroke management, especially in the treatment of acute ischemic stroke (Wen et al., 2005; Yang et al., 2008; Sun et al., 2009; Shen et al., 2012; Chen and Ni, 2013). Manipulation of the XNKQ needling method varies in accordance with the patient’s condition. In general, the pointsNeiguan(PC6),Renzhong(GV26),Sanyinjiao(SP6),Jiquan(HT1),Weizhong(BL40), andChize(LU5) are involved in therapeutic regimen;Fengchi(GB20),Yifeng(TE17), andWangu(GB12) are used for dysphagia;Hegu(LI4) is applied in patients with fi nger dysfunction;Qiuxu(GB40) andZhao-hai(KI6) are used for pes adductus; andLianquan(CV23) and blood-letting therapy onJinjin(Ex-HN12) andYuye(Ex-HN13) are used for slurred speech.e XNKQ needling method is now a widely accepted intervention for the treatment of acute ischemic stroke; however, comprehensive evaluations and systematic reviews of its ef f ectiveness and safety are lacking. No systematic review of this subject has yet been performed. For this reason, we carried out the present systematic review to critically assess evidence from randomized clinical trials (RCTs) of the XNKQ needling method performed to improve symptoms of acute ischemic stroke.
Methods
Data sources
The following digital databases were searched for relevant studies published from June 2006 to March 2016: the Cochrane Central Register of Controlled Trials (up to the Cochrane Library Issue 03, 2016), MEDLINE, CINAHL, AMED, Embase, and four Chinese databases: China National Knowledge Infrastructure, WEIPU Information Resources System, Wanfang Medical Data System, and Chinese Biomedical Literature Database. In addition, the following journals were searched by manual retrieval:Chinese Acupuncture and Moxibustion,Acupuncture Research,Journal of Traditional Chinese Medicine, Journal of Clinical Acupuncture and Moxibustion,Shanghai Journal of Acupuncture and Moxibustion,Journal of New Chinese Medicine,Tianjin Journal of Traditional Chinese Medicine,Shanghai Journal of Traditional Chinese Medicine,Jiangsu Journal of Traditional Chinese Medicine,Liaoning Journal of Traditional Chinese Medicine, andZhejiang Journal of Traditional Chinese Medicine.
The following terms were used for retrieval of English literature: “Xingnao Kaiqiao,” “stroke,” “ischemic stroke,”“cerebrovascular accident,” “apoplexy,” “ischemia apoplexy,” “cerebral infarction,” “cerebral embolism,” “cerebral thrombosis,” and “transient ischemic attack.”e following terms were used for retrieval of Chinese literature: “Xingnao Kaiqiaoneedling method” and “stroke” (apoplexy, cerebrovascular accidents, ischemic stroke, cerebral infarction, cerebral thrombosis, transient ischemic attack, and cerebral embolism).
Study selection
All clinical RCTs of the XNKQ needling method for acute ischemic stroke were considered. The studies were eligible for inclusion if they met the following inclusion criteria: (1) The diagnosis of stroke met the diagnostic criteria of the World Health Organization (No authors listed, 1989) or National Conference of Cerebrovascular Disease (China) (Chinese Neuroscience Society, 1997). (2) The study was performed irrespective of sex or age but was an RCT in patients with an onset of acute ischemic stroke within 2 weeks (Writing Group of Guidelines for Diagnosis and Treatment of Acute Ischemic Stroke, Cerebrovascular Disease Group, Neurological Section, Chinese Medical Association, 2011). (3) The treatment group underwent the XNKQ needling method alone or combined with other treatment methods, while the control group underwent traditional acupuncture alone or with other treatment methods excluding the XNKQ needling method. (4) Mortality, disability, safety and health, economic indicators, activities of daily living (Barthel index), and clinical ef fi cacy were evaluated. Studies were excluded if traditional acupuncture or other treatments were used in addition to the XNKQ needling method in the treatment group but not in the control group.
Data extraction and assessment of risk of bias
According to the Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1 (Higgins and Green, 2013), the selected articles were evaluated with respect to the following six criteria: sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other issues. Each criterion was judged using one of three answers: “yes,” “no,” or “unclear.”“Yes” indicated a low risk of bias, “no” indicated a high risk of bias, and “unclear” indicated that insuf fi cient information was available for this judgment.
Two independent reviewers screened the titles and abstracts of the articles in each database and searched for relevant articles according to the predefined criteria. The data extraction was carried out and cross checked by two independent reviewers according to the developed criteria. If necessary, the authors of the original articles were contacted to obtain detailed information on implementation of the trial, and disagreements were resolved by discussions between the two reviewers or a third reviewer (Zhan et al., 2013).
Statistical analysis
Cochrane systematic review software RevMan 5.2 (http:// handbook.cochrane.org) (Cochrane systematic review so-ware RevMan 5.2, 2013) was used for the meta-analysis. A clinical and methodological heterogeneity analysis was performed for all included studies, and a subgroup analysis was then performed. The chi-square test was used for the statistical analysis; a probability value of 0.10 was considered to indicate statistical significance, and aPvalue of < 0.10 indicated heterogeneity between the results of the studies. TheI2value was used for quantitative assessment (Higgins et al., 2003). Heterogeneity is not obvious whenI2< 25%, moderate heterogeneity exists whenI2ranges from 25% to 50%, and greater heterogeneity exists whenI2> 50%. Heterogeneous test results are expressed with a random-ef f ects model, and homogeneous test results are expressed with a fi xed-ef f ects model (Higgins et al., 2009).e ef f ect size for ef fi cacy was evaluated using interval estimation and hypothesis testing. The risk ratio (RR) was used for enumeration data, the weighted mean difference (WMD) was used for continuous variables, and interval estimation was performed using the 95% conf i dence interval (CI) (Higgins et al., 2003). TheUtest was used for hypothesis testing, and the resultsare represented byZandPvalues. The level of statistical signif i cance was set at 0.05, and dif f erences between curative ef f ects were statistically signif i cant atP< 0.05.e hypothesis test results are listed in a forest plot. When necessary, a sensitivity analysis was adopted to test the stability of the results (Higgins et al., 2003). Incomplete data were processed by intention analysis (Higgins et al., 2003). Descriptive analysis was adopted if heterogeneity was large between the two groups or the sources of heterogeneity could not be found (Higgins et al., 2003).
Results
Description of study
The literature search revealed 568 potentially relevant articles. Aer screening the titles and abstracts, 442 studies were excluded because they were repeated or were not clinical trials.e full text of the remaining 126 studies were retrieved for further assessment; of these, 114 articles were excluded because they did not meet the inclusion criteria or were RCTs, had invalid data, or were simple case reports. Finally, 12 RCTs were included in this review (Figure 1). All were published in China, and all results showed benef i cial ef f ects of XNKQ acupuncture.
Each study enrolled 20 to 100 patients (1,006 patients in total). All studies focused on the XNKQ needling method, which was accompanied by conventional medicine in some of the studies. In all studies, comparison was performed between the XNKQ needling method and either traditional acupuncture or conventional medicine. Two studies (Liu et al., 2006; Rao et al., 2006) described the mortality and disability rates, four studies (Liu et al., 2006, 2012; Rao et al., 2006; Liu and Chen, 2012) described the safety, four studies (Chen and Li, 2006; Liu et al., 2006; Rao et al., 2006; Xiong et al., 2006) described the activities of daily living (Barthel index), nine studies (Chen and Li, 2006; Xiong et al., 2006; Pi et al., 2007; Wang and Gao, 2008; Xiong et al., 2011; Yang et al., 2011; Guo, 2012; Liu and Chen, 2012; Liu et al., 2012; Wang et al., 2013) described the clinical efficacy, and no studies described the relevant economic indicators. Outcome data of all studies (Chen and Li, 2006; Liu et al., 2006, 2012; Rao et al., 2006; Xiong et al., 2006; Pi et al., 2007; Wang and Gao, 2008; Xiong et al., 2011; Yang et al., 2011; Guo, 2012; Liu and Chen, 2012; Liu et al., 2012) were integrated. All selective outcome reporting judgments were “yes.” Other sources of bias were unclear.e details and features of the included studies are shown in Additional Table 1.
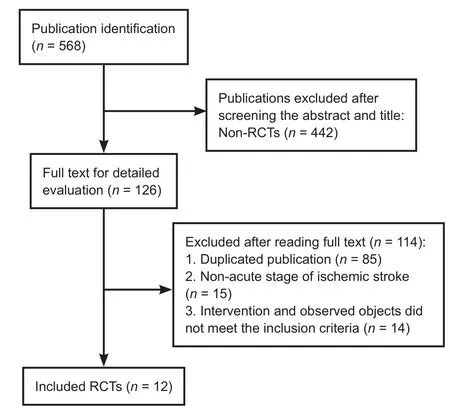
Figure 1 Flow chart of selection of studies included in the review. RCTs: Randomized controlled trials.
Assessment of risk of bias

Figure 2 Risk of bias summary: review of authors’ judgments about each risk of bias item for each included study.
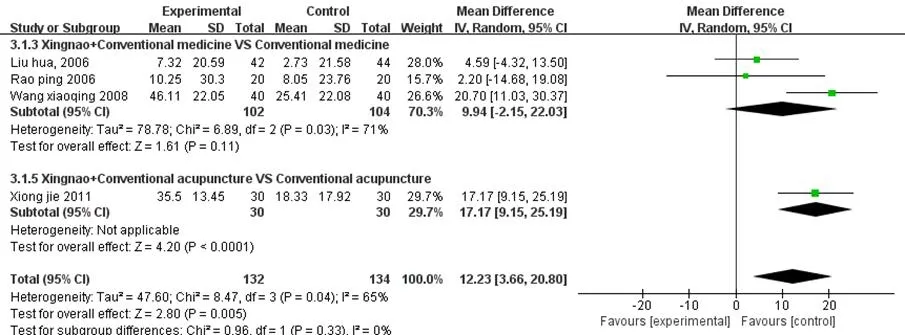
Figure 3 Forest plot presenting the study and subgroup meta-analysis for activities of daily living (Barthel index) of theXingnao Kaiqiaoneedling method for acute ischemic stroke.
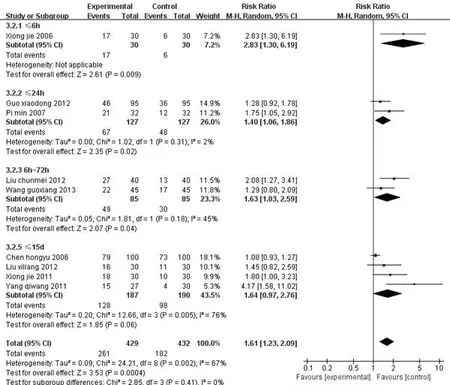
Figure 4 Forest plot presenting the study and subgroup meta-analysis for the clinical efficacy of theXingnao Kaiqiaoneedling method for acute ischemic stroke.
Results of meta-analysis
Among the three studies (Liu et al., 2006, 2012; Rao et al., 2006) that indicated the mortality and disability rates at the end of treatment or final follow-up (≥3 months), no clinical or statistical heterogeneity was present. A fi xed-effects model was adopted for the meta-analysis (Yang et al., 2015), and signif i cant dif f erences were found in the disability rate but not in mortality. Nevertheless, for mortality, the horizontal line of the combined effect size RR intersected and was located to the left side of the equivalent vertical line.ese results indicate that among patients with ischemic stroke, the XNKQ needling method more ef f ectively reduced mortality and disability than did other treatments in the control group.
Adverse reactions
No adverse reactions were reported in the three studies (Liu et al., 2006, 2012; Rao et al., 2006).
Health-economic indicators
None of the included studies (Chen and Li, 2006; Liu et al., 2006, 2012; Rao et al., 2006; Xiong et al., 2006; Pi et al., 2007; Wang and Gao, 2008; Xiong et al., 2011; Yang et al., 2011; Guo, 2012; Wang et al., 2013) reported the cost or other health-economic indicators.
Activities of daily living (Barthel index) at end of treatment or fi nal follow-up (≥3 months)
Clinical ef fi cacy at end of treatment or fi nal follow-up (≥3 months)
Discussion
Summary of the main results
Potential inf l uencing factors
In the primary outcome analysis, XNKQ acupuncture had no significant benefit with respect to the mortality rate. However, this result should be interpreted with caution because it relies on data from only three trials (Liu et al., 2006, 2012; Rao et al., 2006) with small sample sizes and low methodological quality. Additionally, dif f erent degrees of neurologic impairment may have dif f erent ef f ects on the mortality of stroke. Because most of the included studies did not provide a detailed description of the characteristics of the patients’ neurological dysfunction, we were unable to explore this issue further. Finally, the follow-up periods (≤6 months) were relatively shorter than in trials testing various surgical or nonsurgical interventions for acute ischemic stroke, which assessed 2-year outcomes aer the treatment intervention (Wei et al., 2011).us, the longer-term ef f ects of the XNKQ needling method could not be assessed in our analyses.
Study limitations
Although this review provides many useful findings, it has several limitations. First, no economic evaluation data were provided in the included studies; therefore, no economic reference is available for clinicians and health policy makers. At present, the treatment expense due to stroke is one of the greatest burdens on the health care system in both developed and developing countries. In the future, health policy should focus on shortening hospital stays and reducing the disability rate (Kaur et al., 2014). Second, although strong efforts were made to find all relevant trials in many databases, our comprehensive search may not have removed all publication- or language-related bias. Third, the included trials were applied in various ways; they dif f er in terms of the study design, sample size, outcome measurement, and characteristics of patients (Magin et al., 2013; Lee et al., 2014). Finally, these trials lacked standard outcome tools. Only a few trials employed objective measures, and no study used a sham group for comparison. Comparison of trials is dif ficult when the choice of outcomes is so heterogeneous. Future trials should be thoroughly focused on the experimental design. Large-scale RCTs with elaborate designs are needed to further verify the ef ficacy and safety of the XNKQ needling method in patients with acute ischemic stroke.
Directions for future research
The current study shows that the XNKQ needling method is safe and ef f ective for acute ischemic stroke. However, the total number of included RCTs and methodological quality was too low to draw a fi rm conclusion, and the strength of the current analysis may have been affected by the limitations. More evidence-based studies should be carried out to provide more reliable data.
Author contributions:ZXY participated in the study concept, design and wrote the paper. JHX and DDL were responsible for data integration and analysis. All authors approved the fi nal version of the manuscript.
Conf l icts of interest:None declared.
Data sharing statement:
Plagiarism check:Checked twice by ienticate.
Peer review:Externally peer reviewed.
Open access statement:
Additional fi le:Additional Table 1 Characteristics of trials included in this review.
Chen HY, Li MW (2006)e analysis of the treatment of Xingnao Kaiqiao acupuncture method and Huatan-tongluo decoction on ischemic apoplexy. Liaoning Zhongyi Zazhi 33:738.
Chen ZL, Ni GX (2013)e new clinical advancement of Xingnao Kaiqiao needling method. Tianjin Zhongyiyao 30:765-768.
Cheng SC, Lin CH, Chang YJ, Lee TH, Ryu SJ, Chen CH, Chang HK, Chang CJ, Hu WL, Hung YC (2013) Fire-heat and Qi deficiency syndromes as predictors of short-term prognosis of acute ischemic stroke. J Altern Complement Med 19:721-728.
Chung KF, Yeung WF, Kwok CW, Yu YM (2014) Risk factors associated with adverse events of acupuncture: a prospective study. Acupunct Med 32:455-462.
Cochrane systematic review soware RevMan 5.2 (2013)e Cochrane Collaboration. http://techcochraneorg/revman/download.
Dong QJ, Yang ZX (2013) Systematic review of resuscitation needling technique for wind stroke. Zhongguo Zhen Jiu 33:475-480.
Goldstein LB, Bushnell CD, Adams RJ, Appel LJ, Braun LT, Chaturvedi S, Creager MA, Culebras A, Eckel RH, Hart RG, Hinchey JA, Howard VJ, Jauch EC, Levine SR, Meschia JF, Moore WS, Nixon JV, Pearson TA, American Heart Association Stroke Council, Council on Cardiovascular Nursing, et al. (2011) Guidelines for the primary prevention of stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 42:517-584.
Higgins JP, Green S (2013) Cochrane handbook for systematic reviews of interventions. Version 5.1.0. In: http://www.cochrane-handbook. org.
Kaur P, Kwatra G, Kaur R, Pandian JD (2014) Cost of stroke in low and middle income countries: a systematic review. Int J Stroke 9:678-682.
Lackland DT, Roccella EJ, Deutsch AF, Fornage M, George MG, Howard G, Kissela BM, Kittner SJ, Lichtman JH, Lisabeth LD, Schwamm LH, Smith EE, Towfighi A; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; Council on Functional Genomics and Translational Biology (2014) Factors inf l uencing the decline in stroke mortality: a statement from the American Heart Association/American Stroke Association. Stroke 45:315-353.
Lee JS, Ahn S, Lee KH, Kim JH (2014) Korean translation of the CONSORT 2010 Statement: updated guidelines for reporting parallel group randomized trials. Epidemiol Health 36:e2014029.
Liu CM, Chen JQ (2012) Ef f ect of modif i ed Xingnao Kaiqiao acupuncture combined with low molecular weight heparin calcium injection on progressive cerebral infarction. Hebei Zhongyi 34:384-386.
Liu H, Wang Y, Ren H, Wang WM, Ma SP (2006) An ef f ect of acupuncture on ADL and cognitive function in patients with ischemic stroke. Zhongguo Kangfu Yixue Zazhi 21:444-448.
Liu XL, Yao HJ, Xu GY, Wang YW, Wang XJ (2012) Early intervention of Xingnao Kaiqiao needling method on stroke neural function. Yixue Xinxi 25:58-59.
Magin P, Victoire A, Zhen XM, Furler J, Pirotta M, Lasserson DS, Levi C, Tapley A, van Driel M (2013) Under-reporting of socioeconomic status of patients in stroke trials: adherence to CONSORT principles. Stroke 44:2920-2922.
No authors listed (1989) Stroke--1989. Recommendations on stroke prevention, diagnosis, and therapy. Report of the WHO Task Force on Stroke and other Cerebrovascular Disorders. Stroke 20:1407-1431.
Pi M, Rao XD, Cao XM, Wu LX, Peng JH, Liu YS, Yu HB, Yang ZX (2007) Different acupuncture on CRP levels of patients with acute cerebral infarction: a clinical study. Zhenjiu Linchuang Zazhi 23:1-4.
Przybylowski CJ, Ding D, Starke RM, Durst CR, Crowley RW, Liu KC (2014) Evolution of endovascular mechanical thrombectomy for acute ischemic stroke. World J Clin Cases 2:614-622.
Ramee SR, White CJ (2014) Acute stroke intervention. Curr Probl Cardiol 39:59-76.
Rao P, Zhou L, Mao M, Bai Y, Wen TM, Tang YH, Guo WL (2006) A randomized controlled trial of acupuncture treatment of acute ischemic stroke. Zhongguo Zhen Jiu 26:694-696.
Shen PF, Kong L, Ni LW, Guo HL, Yang S, Zhang LL, Zhang ZL, Guo JK, Xiong J, Zhen Z, Shi XM (2012) Acupuncture intervention in ischemic stroke: a randomized controlled prospective study. Am J Chin Med 40:685-693.
Shi XM (1998) Stroke and Xingnao Kaiqiao Needling Method. Tianjin: Tianjin Science and Technology Press.
Sun LJ, Zhang ZL, Ji XQ (2009) Clinical advancement of needling method of open the orif i ces on each stage of wind stroke. Liaoning Zhongyi Zazhi 36:153-154.
Wang GX, Huang ZC, Bi JR, Wang XS, Liu ZB, Yu SH (2013) Acupuncture combined butyl phthalide socapsule in the treatment of cerebral infarction curative ef f ect research. Zhongyi Xuebao 28:1368-1369.
Wang XQ, Gao C (2008)e treatment of Xingnao Kaiqiao acupuncture combined with rehabilitation training on apoplexy hemiplegia. . Hebei Yike Daxue Xuebao 29:559-560.
Wei YC, Sun MF, Chang KC, Chang CJ, Hung YC, Lin YJ, Chiu HH (2011) Pilot scheme of health policy in stroke adjuvant acupuncture therapy for acute and subacute ischemic stroke in taiwan. Evid Based Complement Alternat Med 2011:689813.
Wen JR, Zhao XF, Wang S, Shi XM (2005)e clinical advancement of Xingnao Kaiqiao needling method. Zhenjiu Linchuang Zazhi 21:40-41.
World Health Organization (2002) Acupuncture: Review and Analysis Reports on Controlled Clinical Trials. Geneva, Switzerland.
Xiong J, Nin LN, Zhang W (2011)e clinical observation of acupuncture on the recovery of neurological function of patients with acute cerebral infarction. Jilin Zhongyiyao 31:237-238.
Xiong J, Zhang W, Li YD, Guo J, Shi XM (2006) Clinical efficacy of Xingnao Kaiqiao acupuncture therapy on neurological impairment in super-early stage acute cerebral infarction. Wujing Yixue 17:416-417.
Yang QW, Zhang DS, Wang SX (2011)e treatment of Sihai Zhishu acupuncture points for 29 cases of acute ischemic apoplexy. Shaanxi Zhongyi 32:206-208.
Yang YQ, Ji XQ, Zhang ZL (2008)e clinical advancement of Xingnao Kaiqiao needling method. Liaoning Zhongyi Zazhi 35:762-763.
Yang ZX, Shi XM (2007) Systematic evaluation of the therapeutic effect and safety of Xingnao Kaiqiao needling method in treatment of stroke. Zhongguo Zhen Jiu 27:601-608.
Yang ZX, Xie JH, Liu YP, Miao GX, Wang YH, Wu SM, Li Y (2015) Systematic review of long-term Xingnao Kaiqiao needling ef f cacy in ischemic stroke treatment. Neural Regen Res 10:583-588.
Zhan M, Liu X, Lu J, Xu T (2013) Erlotinib for elderly patients with non-small-cell lung cancer: A systematic review. Zhongguo Xunzheng Yixue Zazhi 13:1084-1089.
Chinese Neuroscience Society (1997)e diagnosis outline of all kinds of cerebrovascular disease. Zhongguo Shiyong Neike Zazhi 17:312.
Writing Group of Guidelines for Diagnosis and Treatment of Acute Ischemic Stroke, Cerebrovascular Disease Group, Neurological Section, Chinese Medical Association, 2011) (2011)e 2010 guide of diagnosis and treatment of acute ischemic stroke in China. Zhongguo Linchuang Yisheng 39:67.
Copyedited by Morben A, Raye W, Yu J, Li CH, Qiu Y, Song LP, Zhao M
*< class="emphasis_italic">Correspondence to: Zhi-xin Yang, Ph.D., yzx19972003@163.com.
Zhi-xin Yang, Ph.D., yzx19972003@163.com.
orcid: 0000-0003-3755-5977 (Zhi-xin Yang)
10.4103/1673-5374.213551
Accepted: 2017-06-26
杂志排行

中国神经再生研究(英文版)的其它文章
- Transcriptional inhibition in Schwann cell development and nerve regeneration
- A progressive compression model of thoracic spinal cord injury in mice: function assessment and pathological changes in spinal cord
- Effects of estrogen receptor modulators on cytoskeletal proteins in the central nervous system
- Optogenetics and its application in neural degeneration and regeneration
- Live-cell imaging: new avenues to investigate retinal regeneration
- Neurotrophic factors and corneal nerve regeneration