先天性马蹄内翻足患儿 Ponseti 法矫正后距骨-跟骨角和胫骨-跟骨角的变化
2017-08-10刘振江严维张立军李祁伟
刘振江 严维 张立军 李祁伟
. 临床研究与实践 Clinical research and practice .
先天性马蹄内翻足患儿 Ponseti 法矫正后距骨-跟骨角和胫骨-跟骨角的变化
刘振江 严维 张立军 李祁伟
目的 探讨利用 Ponseti 方法 ( 手法矫正+系列石膏固定+经皮跟腱切断术+足外展矫形支具 )治疗先天性马蹄内翻足 ( congenital talipes equinovarus,CTEV ) 后,足部站立位侧位 X 线片上距骨-跟骨角和胫骨-跟骨角的变化。方法 回顾性分析 2013年 1月至 2015年 12月,应用 Ponseti 方法在我院小儿骨科治疗,且最近一次随访时拍摄双足站立位侧位 X 线片的 24例 CTEV 患儿。男 19例,女 5例;左侧 4例,右侧12例,双侧 8例。5例 ( 10足 ) 正常儿童作为双侧病例的对照组。全部患儿的 Ponseti 系列石膏矫形和经皮跟腱切断术 ( percutaneous achilles tenotomy,PAT ) 均由同一医生完成。临床评价指标包括:初始治疗时年龄、性别、单 ( 双 ) 侧、治疗前和最近一次随访时 Pirani 严重性评分、石膏次数和是否行 PAT。影像学评估指标包括:( 1) 侧位距骨-跟骨角 ( lateral talocalcaneal angle,LTCA );( 2) 侧位胫骨-跟骨角 ( lateral tibiocalcaneal angle,LTiCA );( 3) 距骨长轴比,即患侧距骨长轴 / 健侧距骨长轴×100%。单侧病例取其健侧作为对照组,双侧病例取正常儿童作为对照组。本研究得到中国医科大学附属盛京医院医学伦理委员会批准,患儿家长均签署知情同意书。结果 单侧病例:初始治疗时年龄 3~94天。平均随访 14.75( 6~35) 个月。治疗前与最近一次随访 Pirani 严重性评分比较,P50:6.0~0,P25:5.25~0,P75:6.0~0.375,P=0.000。LTCA:患侧27.81° ( 14°~40° ),健侧 51.25° ( 38°~66° ),P=0.000。LTiCA:患侧 82.19° ( 51°~102° ),健侧 79.00° ( 57°~89° ),P=0.35。距骨长轴比 81.94% ( 71.97%~96.70% )。双侧病例:初始治疗时年龄 8~173天,平均随访 21.63( 3~71) 个月。治疗前与最近一次随访 Pirani 严重性评分比较,左足 P50:6.0~0分,P25:4.75~0分,P75:6.0~0分,P=0.000;右足 P50:6.0~0分,P25:5.63~0分,P75:6.0~0.375分;P=0.000。左足LTCA:患侧 30.38° ( 19°~46° ),对照组 53.40° ( 46°~66° ),P=0.001;右足 LTCA:患侧 33.75° ( 20°~53° ),对照组 57° ( 45°~70° ),P=0.001。左足 LTiCA:患侧 83.75° ( 50°~111° ),对照组 76.60° ( 65°~86° ),P=0.456;右足 LTiCA:患侧 80.75° ( 60°~97° ),对照组 76.80° ( 69°~88° ),P=0.588。结论 Ponseti 方法治疗CTEV 后,足部外观和 Pirani 评分显著改善。患足距骨变小,距骨-跟骨角仍小于正常值,而胫骨-跟骨角恢复接近正常值。
马蹄内翻足;足畸形,先天性;距骨跟骨角;胫骨跟骨角;Ponseti
先天性马蹄内翻足 ( congenital talipes equinovarus,CTEV ) 是最常见的骨关节先天畸形,发生率约为 1‰[1-3]。CTEV 是一种三维畸形,表现为冠状位后足内翻,水平位前足内收,矢状位踝关节跖屈畸形[4]。Ponseti 系列石膏矫形技术极大改善了 CTEV的治疗效果[5-6],逐渐被越来越多的儿童骨科医生所接受[7-10]。经过 Ponseti 系列石膏矫形后,虽然绝大多数患儿的足部外观和功能表现正常,但是患足的 X 线影像学指标是否得到恢复,仍有待研究。本研究目的是探讨应用 Ponseti 方法治疗 CTEV 后,在站立位、侧位 X 线片上侧位距骨-跟骨角 ( lateral talocalcaneal angle,LTCA ) 和侧位胫骨-跟骨角( lateral tibiocalcaneal angle,LTiCA ) 的变化。
资料与方法
一、纳入与排除标准
1. 纳入标准:( 1) 2013年 1月至 2015年 12月应用 Ponseti 方法在我院接受治疗的 CTEV 者;( 2) 最近一次随访时拍摄双足站立位、侧位 X 线片的患儿。
2. 排除标准:( 1) 综合征性马蹄内翻足;( 2) 神经源性马蹄内翻足 ( 脊髓栓系,脊髓脊膜膨出,遗传性运动性感觉神经病等所致 );( 3) 多发性关节挛缩症所致马蹄内翻足;( 4) 外伤性马蹄内翻足。
本研究得到中国医科大学附属盛京医院医学伦理委员会批准,患儿家长均签署知情同意书。
二、一般资料
本组共 24例 ( 32足 )。其中男 19例,女 5例;左侧 4例,右侧 12例,双侧 8例;5例 ( 10足 ) 正常儿童作为双侧病例的对照组。石膏次数为 4~12次,平均 5.8次。全部 32足均接受经皮跟腱切断术 ( percutaneous achilles tenotomy,PAT ),术后石膏固定 3周 ( 表 1)。
三、临床评价指标
包括初始治疗时年龄、性别、单 ( 双 ) 侧、治疗前和最近一次随访 Pirani 严重性评分、石膏次数以及是否行 PAT。
四、X 线片测量指标
包括 LTCA、LTiCA ( 图 1) 和距骨长轴比( 图 2)。单侧病例取对侧作为对照组,双侧病例取正常儿童作为对照组。
五、Ponseti 治疗方法
1. 患儿安静后平卧 ( 家长安抚、喂奶和音乐 ),去除尿不湿。
2. 手法矫正:治疗者拇指按压在距骨头外侧,前足外展旋后位,提升第一序列足弓,不能固定跟骰关节,持续 1min。不能强力背屈踝关节。
3. 石膏固定:软石膏绷带,从足趾开始缠绕至大腿根部。屈膝 90° 防止石膏脱落。每周更换一次石膏。经过石膏连续矫形,高弓足,前足内收,跟骨内翻均已纠正,仅残留跟腱挛缩尚未纠正。
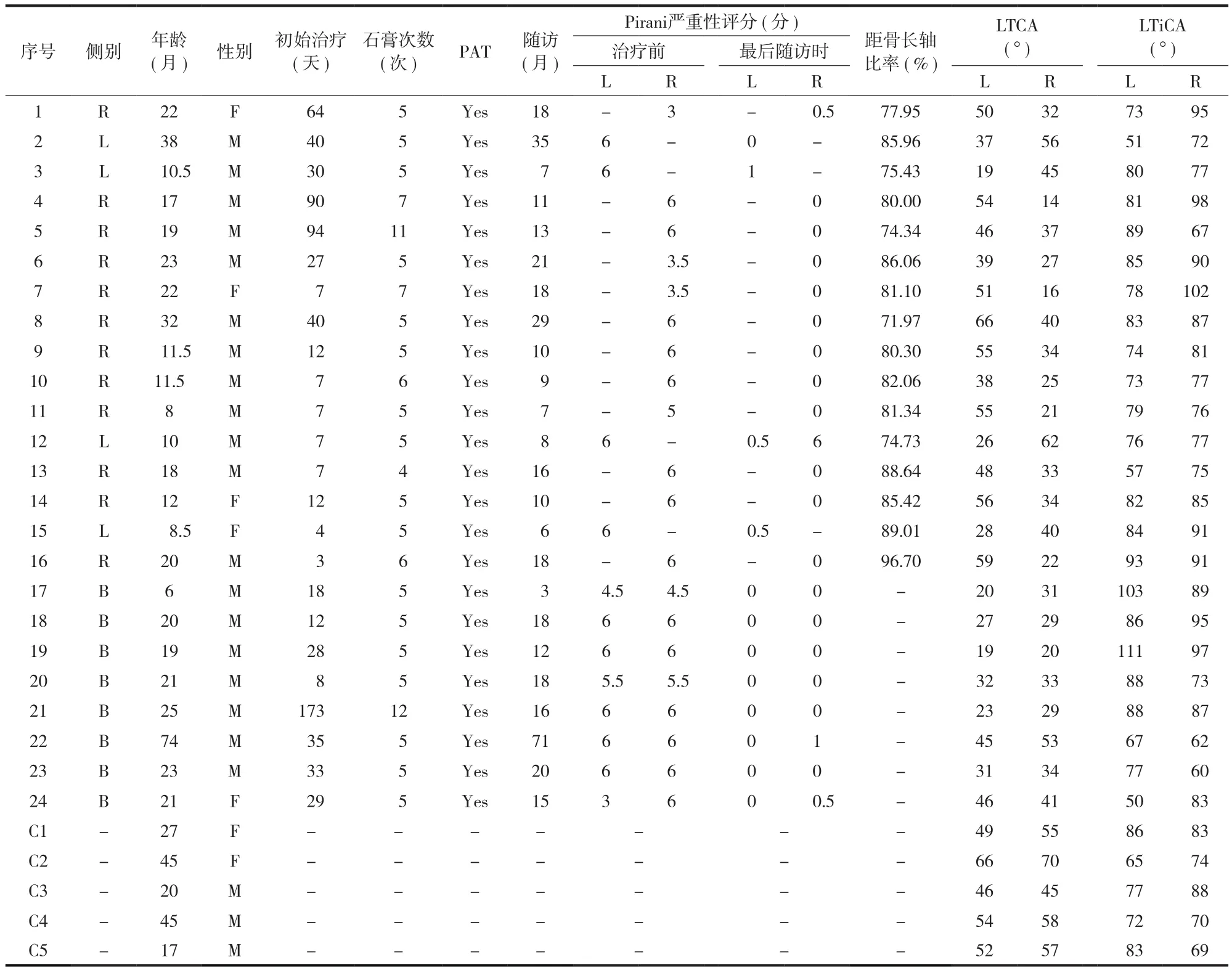
表1 先天性马蹄内翻足和对照组临床资料及测量参数Tab.1Clinical data of the clubfoot group and control group
4. PAT:全部患儿均在手术室内,全身麻醉下进行 PAT。PAT 术后立即给予长腿软石膏绷带固定,保持患足外旋 70°、足背屈 15° 位置,固定 3周。
5. 佩戴 Danis Browne 足外展支具:在 PAT 术后前 3个月内,每天佩戴至少 23h,每 2周门诊随访支具佩戴顺应性;术后 3个月嘱家长尽可能延长支具佩戴时间,保证白天至少 12h,夜间至少 4~6h,直至患儿学会走路,每 3个月门诊随访;患儿学会走路后,要求夜间睡眠和白天午睡时必须佩戴支具,直到 4岁,每 6个月门诊随访。
六、统计学处理
采用 SPSS 22.0,配对 t 检验,P<0.05认为差异有统计学意义。正态分布数据采用±s 表示。非正态分布数据采用四分位数法表示。P25、P50、P75分别表示样本中所有数值由小到大排列后第 25%、第50% 和 75% 的数字。
结 果
一、单侧病例
初始治疗时年龄 3~94天,P50:12天,P25:4天,P75:40天。随访时间 6~35个月,平均( 14.75±8.26) 个月。Pirani 严重性评分,治疗前P50:6.0分,P25:5.25分,P75:6.0分;最近一次随访时 P50:0分,P25:0分,P75:0.375分,P=0.000。患侧 LTCA 平均 ( 27.81± 7.91) ° ( 14°~40° ),健侧 LTCA 平均 ( 51.25± 8.19) ° ( 38°~66° ),P=0.000。患侧 LTiCA 平均 ( 82.19±12.50) ° ( 51°~102° ),健侧 LTiCA 平均 ( 79.00±8.73) ° ( 57°~89° ),P=0.35。距骨长轴比为 ( 81.94± 6.50) % ( 71.97%~96.70% )。
二、双侧病例
初始治疗时年龄 8~173天,P50:28.5天,P25:13.5天,P75:34.5天。随访时间 3~71个月,平均 ( 21.63±20.64) 个月。Pirani 严重性评分,治疗前左足 P50:6.0分,P25:4.75分,P75:6.0分;最近一次随访时左足 P50:0分,P25:0分,P75:0分,P=0.000;治疗前右足 P50:6.0分,P25:5.63分,P75:6.0分;最近一次随访时右足 P50:0分,P25:0分,P75:0.375分,P=0.000。患侧左足 LTCA 平均 ( 30.38±10.45) ° ( 19°~46° ),对照组左足 LTCA平均 ( 53.40±7.67) ° ( 46°~66° ),P=0.001;患侧右足 LTCA 平均 ( 33.75±9.75) ° ( 20°~53° ),对照组右足 LTCA 平均 ( 57±8.92) ° ( 45°~70° ),P=0.001。患侧左足 LTiCA 平均 ( 83.75±19.34) ° ( 50°~111° ),对照组左足 LTiCA 平均 ( 76.60± 8.44) ° ( 65°~86° ),P=0.456;患侧右足 LTiCA平均 ( 80.75±14.25) ° ( 60°~97° ),对照组右足LTiCA 平均 ( 76.80±8.35) ° ( 69°~88° ),P=0.588( 图 1)。
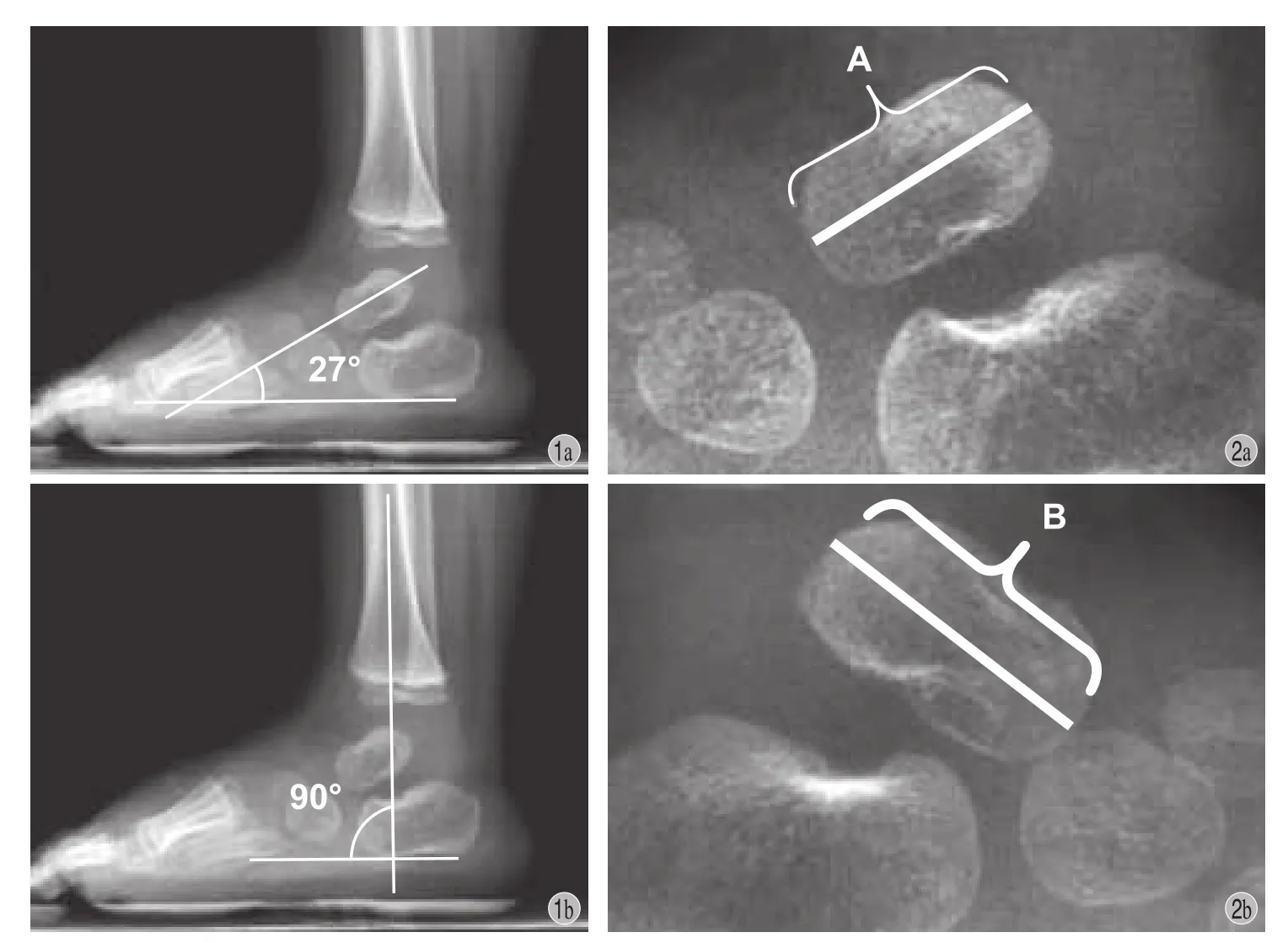
图1 患儿,男,23个月,右侧马蹄内翻足,随访 21个月a:患侧 LTCA 27°,即距骨长轴与跟骨长轴夹角;b:患侧LTiCA 90°,即胫骨长轴与跟骨长轴夹角图2a:患侧距骨长轴;b:健侧距骨长轴 [距骨长轴比 = 患侧距骨长轴 ( A ) / 健侧距骨长轴( B ) × 100%]Fig.1Male, 23-month-old with the right clubfoot. The follow-up was 21months a: The LTCA was 27°. LTCA was the angle between the talar axis and the calcaneal axis; b: The LTiCA was 90°. LTiCA was the angle between the tibial axis and the calcaneal axisFig.2a: The length of the talus long axis of the clubfoot; b: The length of the talus long axis of the normal foot. ( the ratio of the long axis of the talus = A / B × 100% )
讨 论
Ponseti 方法被认为是早期治疗 CTEV 的标准方法。一般经过 4~7次的系列石膏矫形,继而经皮跟腱切断术和足外展支具,可以治愈绝大多数 CTEV[11]。Pirani 严重性评分已经被广泛应用于CTEV 的分类系统中[11],包括 6个部分:后方皱褶( posterior crease,PC )、跖屈角度 ( degree of equinus,E )、空足跟 ( heel emptiness,HE )、内侧皱褶( medial crease,MC )、足外侧缘弯曲 ( curvature lateral border,CLB ) 和距骨头位置 ( talar head position,TH )。按照严重程度,记录为 0分 ( 无畸形 )、0.5分 ( 中度畸形 )、1分 ( 严重畸形 )。本组 Pirani 严重性评分对比,单侧病例组治疗前 5.25~6.0分;治疗后 0~0.375分,P=0.000。双侧病例组:左足治疗前 4.75~6.0分,治疗后 0分,P=0.000;右足治疗前 5.63~6.0分,治疗后 0~0.375分,P=0.000。提示 CTEV 经 Ponseti 方法治疗后,患足外观已经显著改善,Pirani 评分显著降低 ( 图 3)。

图3 患儿,男,6.2岁,双侧马蹄内翻足,随访 71个月;治疗前 Pirani 评分左侧 6.0分,右侧 6.0分;治疗后左侧 0分,右侧 1分a~b:治疗前外观相;c~d:治疗后外观相Fig.3Male, 6.2years old, bilateral clubfeet. The follow-up was 71months. The Pirani severity score recorded before the treatment was 6points in the bilateral feet. The Pirani severity score recorded in the latest follow-up was 0point in the left foot and 1point in the right foot a - b: The clinical appearance before the initial treatment; c - d: The clinical appearance in the latest follow-up
测量单侧病例的距骨长轴比,即患侧距骨长轴 / 健侧距骨长轴×100%,以此来衡量患足距骨长度变化。距骨长轴比为 ( 81.94±6.50) % ( 71.97%~96.70% ),说明 CTEV 经过 Ponseti 治疗后,虽然患足外观已有明显改善,但是距骨长度约为正常值的80% 左右,未恢复至正常。Pinto 等[12]发现经 Mckay手术治疗的 CTEV,手术侧与对侧的距骨长度比为79% ( 61%~88% )。本组数据与 Pinto 的结果接近。
LTiCA 可以反映出 CTEV 中踝关节真实活动状况,排除了中足被假性矫正的可能[13-14]。Kang和 Park[15]认为对于是否需要行 PAT,LTiCA 是一个更客观的判断指标。当 LTiCA ≤80° 时,即使不行 PAT,也不会出现矢状位畸形的复发;当 LTiCA<80° 时,如果不行 PAT,则矢状位畸形的复发率很高。本组病例均行 PAT,无论在单侧病例还是在双侧病例,术后 LTiCA 均与对照组差异无统计学意义,提示无矢状位畸形的复发。这与术后 Pirani 评分中跖屈角度达到正常值 0分的临床表现相一致。
LTCA 是广泛用于 CTEV 矫正程度的指标[16-17],反映出距骨和跟骨之间的解剖关系。然而 Laaveg等[6]和 Abulsaad 等[18]都认为 CTEV 治疗后的临床效果和 LTCA 之间并无显著性相关,LTCA 对于 CTEV矫正效果的评估并非一个优良的指标。本组数据显示患侧 LTCA 均明显小于对照侧,与临床矫正效果明显改善和 Pirani 评分降低均不符合。提示 LTCA对于判断 CTEV 的矫正效果并不可靠。
[1] Chung CS, Nemechek RW, Larsen IJ, et al. Genetic and epidemiological studies of clubfoot in Hawaii. General and medical considerations[J]. Hum Hered, 1969, 19(4):321-342.
[2] Wallander H, Hovelius L, Michaelsson K. Incidence of congenital clubfoot in Sweden[J]. Acta Orthop, 2006, 77(6): 847-852.
[3] Kancherla V, Romitti PA, Caspers KM, et al. Epidemiology of congenital idiopathic talipes equinovarus in Iowa, 1997-2005[J]. Am J Med Genet A, 2010, 152A(7):1695-1700.
[4] Herzenberg JE, Carroll NC, Christofersen MR, et al. Clubfoot analysis with three-dimensional computer modeling[J]. J Pediatr Orthop, 1988, 8(3):257-262.
[5] Herzenberg JE, Radler C, Bor N. Ponseti versus traditional methods of casting for idiopathic clubfoot[J]. J Pediatr Orthop, 2002, 22(4):517-521.
[6] Laaveg SJ, Ponseti IV. Long-term results of treatment of congenital club foot[J]. J Bone Joint Surg Am, 1980, 62(1): 23-31.
[7] Lehman WB, Mohaideen A, Madan S, et al. A method for the early evaluation of the Ponseti (Iowa) technique for the treatment of idiopathic clubfoot[J]. J Pediatr Orthop B, 2003, 12(2):133-140.
[8] Dobbs MB, Corley CL, Morcuende JA, et al. Late recurrence of clubfoot deformity: a 45-year followup[J]. Clin Orthop Relat Res, 2003, (411):188-192.
[9] Ippolito E, Farsetti P, Caterini R, et al. Long-term comparative results in patients with congenital clubfoot treated with two different protocols[J]. J Bone Joint Surg Am, 2003, 85-A(7): 1286-1294.
[10] Bor N, Herzenberg JE, Frick SL. Ponseti management of clubfoot in older infants[J]. Clin Orthop Relat Res, 2006, 444: 224-228.
[11] O’Halloran CP, Halanski MA, Nemeth BA, et al. Can radiographs predict outcome in patients with idiopathic clubfeet treated with the ponseti method[J]? J Pediatr Orthop, 2015, 35(7):734-738.
[12] Pinto JA, Hernandes AC, Buchaim TP, et al. Radiographic abnormalities of the talus in patients with clubfoot after surgical release using the mckay technique[J]. Rev Bras Ortop, 2015, 46(3):293-298.
[13] Radler C, Manner HM, Suda R, et al. Radiographic evaluation of idiopathic clubfeet undergoing Ponseti treatment[J]. J Bone Joint Surg Am, 2007, 89(6):1177-1183.
[14] de Gheldere A, Docquier PL. Analytical radiography of clubfoot after tenotomy[J]. J Pediatr Orthop, 2008, 28(6): 691-694.
[15] Kang S, Park SS. Lateral tibiocalcaneal angle as a determinant for percutaneous achilles tenotomy for idiopathic clubfeet[J]. J Bone Joint Surg Am, 2015, 97(15):1246-1254.
[16] Bensahel H, Dimeglio A, Souchet P. Final evaluation of clubfoot[J]. J Pediatr Orthop B, 1995, 4(2):137-141.
[17] Simons GW. A standardized method for the radiographic evaluation of clubfeet[J]. Clin Orthop Relat Res, 1978, (135): 107-118.
[18] Abulsaad M, Abdelgaber N. Correlation between clinical outcome of surgically treated clubfeet and different radiological parameters[J]. Acta Orthop Belg, 2008, 74(4):489-495.
为支持多中心协作研究项目,可以在论文首页下方脚注“各协作单位第一作者均为本文的第一作者”。
Evaluation of the lateral talocalcaneal angle and lateral tibiocalcaneal angle after using the Ponseti method for congenital clubfoot
LIU Zhen-jiang, YAN Wei, ZHANG Li-jun, LI Qi-wei.
Department of Pediatric Orthopedics, Shengjing Hospital of China Medical University, Shenyang, Liaoning, 110004, China Corresponding author: ZHANG Li-jun, Email: franklj@sj-hospital.org
Objective To investigate the changes of the lateral talocalcaneal angle ( LTCA ) and the lateral tibiocalcaneal angle ( LTiCA ) seen on lateral radiographs taken in the standing position of the patients undergoing treatment for congenital talipes equinovarus by the Ponseti method ( serial manipulation, casting, tenotomy of the Achilles tendon and a foot abduction brace ). Methods From January 2013to December 2015, 24patients with congenital talipes equinovarus were treated by the Ponseti method in our department, whose clinical data were retrospectively analyzed. The lateral radiographs of bilateral feet were taken in the standing position of all the patients at the latest follow-up. The Ponseti manipulations, series of castings and percutaneous Achilles tenotomies ( PAT ) were performed by the same pediatric orthopedic surgeon. Clinical assessment indicators included age at the time of initial treatment, sex, unilateral clubfoot or bilateral clubfeet involvement, and numbers of castings as well as PAT determinedby the Pirani severity score system before treatment and at the latest follow-up. Radiographic indicators included LTCA, LTiCA and the ratios of the long axis of the talus, which were calculated by measuring the talus long axis of the clubfoot and then dividing this by the talus long axis of the normal foot. For the patients with a unilateral clubfoot, the normal side was used as the control. For the patients with bilateral clubfeet, normal children were chosen to be the control group. The Medical Ethics Committee of Shengjing Hospital of China Medical University approved this study, and informed consents were obtained from all the patients as well as from the children of the needed control group. Results A total of 24patients ( 32feet ), 19males and 5females, were included in the study. Four patients presented with a left clubfoot, 12patients with a right clubfoot and 8patients with bilateral clubfeet. Five normal children ( 10feet ) were chosen to be the control group for the patients with bilateral clubfeet. The mean number of castings were 5.8times ( range: 4- 12times ). PAT were performed on all 32clubfeet, and the immobilization time with casting was 3weeks. In the patients with a unilateral clubfoot, the age at the time of initial treatment varied from 3to 94days. The average time of follow-up was 14.75months ( range: 6- 35months ). The Pirani severity scores were compared between pre-treatment and in the latest follow-up: 6.0versus 0points ( P50), 5.25versus 0points ( P25) and 6.0versus 0.375points ( P75), P = 0.000. The average LTCA of the affected feet was 27.81° ( range: 14° - 40° ), and the average LTCA of the normal feet was 51.25° ( range: 38° - 66° ), P = 0.000. The average LTiCA of the affected feet was 82.19° ( range: 51° - 102° ), and the average LTiCA of the normal feet was 79.00° ( range: 57° - 89° ), P = 0.35. The ratio of the long axis of the talus was 81.94% ( range: 71.97% - 96.70% ). In the patients with bilateral clubfeet, the age at the time of initial treatment varied from 8to 173days. The average time of follow-up was 21.63months ( range: 3- 71months ). The Pirani severity scores recorded between pre-treatment and in the latest follow-up in the left foot of this group were 6.0versus 0points ( P50), 4.75versus 0points ( P25), and 6.0versus 0points ( P75), P = 0.000; the Pirani severity scores recorded between pre-treatment and in the latest follow-up in the right foot of this group were 6.0versus 0points ( P50), 5.63versus 0points ( P25), and 6.0versus 0.375points ( P75), P = 0.000. The average LTCA of the left foot in the bilateral clubfeet patient group was 30.38° ( range: 19° - 46° ), and the average LTCA of the normal left foot in the control group was 53.40° ( range: 46° - 66° ), P = 0.001. The average LTCA of the right foot in the bilateral clubfeet patient group was 33.75° ( range: 20° - 53° ), and the average LTCA of the normal right foot in the control group was 57° ( range: 45° - 70° ), P = 0.001. The average LTiCA of the affected left foot in the bilateral clubfeet patient group was 83.75° ( range: 50° - 111° ), and the average LTiCA of the normal left foot in the control group was 76.60° ( range: 65° - 86° ), P = 0.456. The average LTiCA of the affected right foot in the bilateral clubfeet patient group was 80.75° ( range: 60° - 97° ), and the normal right foot of the control group was 76.80° ( range: 69° - 88° ), P = 0.588. Conclusions The Pirani severity scores are signif i cantly improved for the congenital talipes equinovarus treated by the Ponseti method, as well as the foot appearance. The dimensions of the affected talus are reduced. The LTCA is smaller than normal value and the LTiCA is closed to the normal value on the standing lateral radiographs of the feet after the treatment with the Ponseti method.
Equinovarus; Foot deformities, congenital; Lateral talocalcaneal angle ( LTCA ); Lateral tibiocalcaneal angle ( LTiCA ); Ponseti method
10.3969/j.issn.2095-252X.2017.08.011
R682.1, R687
110004 沈阳,中国医科大学附属盛京医院小儿骨科
张立军,Email: franklj@sj-hospital.org
2017-03-27)
( 本文编辑:李慧文 )
关于作者姓名、单位在论文中的脚注方法
因毕业、工作调动或进修结束等情况单位变动时,论文署名单位应为原单位,介绍信也应由原单位加盖公章批准。刊出时可另行注明第一作者现在工作单位及相应的科室、邮编。
2. 集体署名作者:凡集体署名的论文,于文末写出“ ( ××× ××× ×××整理 ) ”的同时,一律在论文首页下方脚注通讯作者有关信息。通讯作者由投稿者自行决定。( 1) 署名单位只有一个时,脚注中只列出通讯作者的姓名、邮政编码、Email 地址。署名单位超过一个时,脚注中还应加列通讯作者的工作单位。( 2) 协作组署名时,需在文末参考文献前列出整理者姓名 ( 方法同前 ) 及协作组成员。在“协作组成员:”字后列出协作组各单位名称,单位名称后括号内列出参加者姓名。同时脚注:“通讯作者:姓名,单位,邮政编码、Email 地址”。
1. 个人作者署名:在论文首页下方进行脚注。“作者单位:”后面列出邮政编码、城市和作者单位 ( 具体到科室 )。个人作者超过一位时,可请作者自行指定一位通讯作者 ( corresponding author ),亦即对选题、科研设计起主要作用者,参与论文撰写并能解答编辑部、读者疑问,对论文负全部责任者;在按原格式列出各位作者单位后,另起一行在“通讯作者:”字样后列出通讯作者姓名、邮政编码、单位名称、Email 地址。
