严重前囊膜浑浊的新式手术方法疗效分析
2017-07-13张智科李学民
张智科++李学民
[摘要] 目的 探索一种新式的治疗严重前囊膜浑浊(ACO)的安全、简便的手术方法。 方法 方便选取2010年11月—2015年11月期间6例白内障超声乳化吸除联合人工晶状体(IOL) 植入术后发生严重ACO的患者(北京大学第三医院3例,中日友好医院3例),前囊膜与IOL间注入玻璃酸钠,使用囊膜剪轮辐状放射状 剪开 纤维组织及前囊膜,形成足够大小的前囊口。随访患者术后1周强炎症反应情况,术后1个月、6个月的矫正视力及前囊口大小情况。 结果 术后1周患者前节无明显炎症反应,术后1个月视力0.25~0.5,较术前提高5~8行,术后6个月时视力0.3~0.5,较术前提高6~8行,术后1个月及6个月时前囊口直径由术前的0~1 mm扩大至5~7 mm。 结论 新的手术方式可有效解除前囊膜的收缩,解除中央纤维组织的遮挡,显著提高视力,术后炎症反应轻,且对悬韧带损伤小,是一种安全有效的手术方式。
[关键词] 前囊浑浊;前囊收缩;放射状切开
[中图分类号] R4 [文献标识码] A [文章编号] 1674-0742(2017)05(b)-0102-03
[Abstract] Objective To explore a safe and simple operation method of anterior capsular turbidity. Methods 6 cases of severe ACO patients after the phacoemulsification and intraocular lens implantation from November 2010 to November 2015 were convenient selected(3 cases were in the third hospital of Beijing University and 3 cases were in the China-Japan Friendship Hospital), and the sodium hyaluronate was injected in the anterior capsule and IOL, and the fiber tissue and anterior capsule were cut thus forming the large enough anterior capsular opening, and the inflammatory reactions at 1 weeks after operation, correctional eyesight and anterior capsular opening size in 1 months and 6 months after operation of patients were followed-up. Results There were no obvious inflammatory reactions of patients in 1 weeks after operation, and the vision increased from 0.25 to 0.5, increasing by 5~8 lines compared with that before operation, and the vision in 6 months after operation was 0.3~0.5, increasing by 6~8 lines compared with that before operation, and the anterior capsular opening diameter in 1 month and 6 month after operation increased from 0~1 mm before operation to 5~7 mm after operation. Conclusion The new operation method can effectively release the contraction of anterior capsule and occlusion of central filamentary microstructure and obviously improve the vision with mild postoperative inflammatory reactions and small injury to suspensory ligament, and it is a safe and effective operation method.
[Key words] Anterior capsular turbidity; Anterior capsular contraction; Radial incision
前囊膜渾浊(anterior capsular opacification,ACO)或囊膜收缩综合征(capsular contraction syndrome,CCS)是连续环形撕囊(continuous curvilinear capsulorhexis, CCC)的并发症之一。ACO引起白内障超声乳化吸除联合人工晶状体(intraocular lens, IOL) 植入术后前囊口缩小、前囊膜浑浊、IOL位置改变等,导致视力下降、眩光等症状。ACO是由残余晶状体上皮细胞增殖,向肌纤维母细胞转化,产生多过的胶原组织引起的[1]。在这些纤维细胞中平滑肌细胞α肌动蛋白可导致前囊收缩,甚至可导致撕囊口完全闭塞。严重的ACO采用激光等传统方法治疗效果不佳,且易产生并发症,该文方便选取2010年11月—2015年11月就诊的6例患者,探讨一种新的严重ACO的手术方法,并对手术效果进行评价,现报道如下。
1 资料与方法
1.1 一般资料
方便选取发生于白内障超声乳化联合IOL植入术后的严重ACO患者6例(6眼),其中3例就诊于北京大学第三医院,3例就诊于中日友好医院;男性4例,女性2例,右眼5例,左眼1例。患者均表现为白内障手术后视力逐渐下降,就诊时白内障术后6个月~3年,视力均低于0.1。6例患者均有前囊膜致密浑浊,囊袋收缩,前囊口近关闭。
1.2 方法
患者A手术过程为例:充分散瞳,2%利多卡因球后麻醉,做3.2 mm透明角膜切口及侧切口。前方注入玻璃酸钠后在前囊纤维膜中央刺一小孔。前囊与IOL间注入玻璃酸钠使前囊与IOL分离,用囊膜剪在前囊膜做數个轮辐状放射切口,长约3 mm。做近侧放射切口时,先在远离中心位置刺一小孔,再自小孔向中心剪开。修剪锯齿状切缘的尖端。自动注吸清除残余组织及粘弹剂。术毕瞳孔中央恢复透明。
1.3 观察指标
术前及术后1、6个月观察并记录患者的矫正视力及前囊口直径,前囊直径据裂隙灯裂隙宽度标尺测量水平最大径。观察术中是否有悬韧带撕裂、人工晶体脱位等并发症,并记录术后1周观察眼前节炎症反应情况。
2 结果
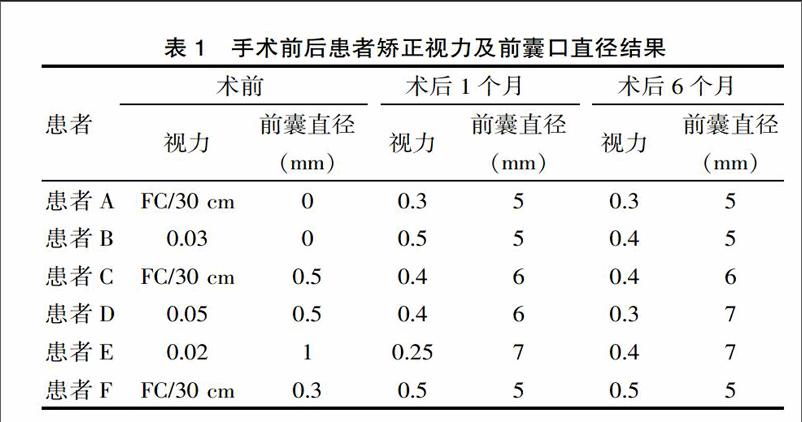
6例患者手术过程顺利,无术中严重并发症。术后前囊口大致呈圆形,直径5~7 mm,未散瞳时虹膜遮盖前囊口。术后1周无明显炎症反应。6例患者术后1个月、6月视力较术前提高5~8行,前囊口直径达到5~7 mm,6例患者术后6个月较术后1个月时囊袋直径无缩小。术后1个月手术前后比较结果见表1。
3 讨论
在高度近视、假性囊膜剥脱、葡萄膜炎、眼外伤、色素性视网膜炎、肌强直性营养不良、高龄患者中ACO更易发生。ACO的发生也与IOL的植入[2]及IOL的材料、设计等有关[3-4]。
Nd:YAG激光囊膜切开能显著降低前囊口的张力[5],进而治疗ACO,但Nd:YAG激光切开严重ACO需要较高的能量,增加了并发症的风险,所以并不推荐其用于严重ACO[6]。激光后游离的囊膜组织及碎片可导致炎症,释放出TGF-β2等众多与ACO发生有关的细胞因子[7],增加了复发的风险。但Page等[8]对13例ACO患者进行Nd:YAG激光囊膜切开治疗发现,术前视力0.05~0.6,治疗后视力提高2~4行,有1例患者复发;应用该研究的方法选取患者的ACO程度严重,术前视力≤0.05,术后视力可提高5~8行,术后6个月时前囊口直径均无明显缩小。因此,该研究采取的新方法针对严重ACO有效,复发可能性较小。有报道[9]对3例患者进行环形撕除纤维膜来治疗ACO,术后视力提高0~3行,但对悬韧带薄弱的病例采用此方法可导致悬韧带损伤,造成人工晶体脱位。而该研究的方法不对囊膜施加向心拉力,对悬韧带损伤小,降低了手术风险。有采用玻切头环形切除纤维组织治疗ACO的病例报告[10]。使用该技术可清除囊膜组织及残余晶状体上皮细胞,防止放射状撕裂口扩大,但该报告选取患者ACO较轻,术前视力0.3,增生组织较薄。该研究中的6例严重的ACO纤维组织显著增生,质地坚韧,前囊口直径0~1 mm,应用玻切头难以有效切割囊膜组织,因此应用玻切头有一定局限性。
该研究采用轮辐状放射切开的方法能安全、简便地治疗严重的ACO。放射切开阻断了纤维组织切线方向的收缩力,可有效解决前囊向心收缩。这些病例中悬韧带往往被收缩的囊袋口牵拉到近中央位置,放射状切开可避免切断悬韧带,保留其对囊袋的离心牵拉作用。悬韧带的拉力使轮辐状放射切开所形成的锯齿状切缘向周边扩大,中央形成足够的透明区域,术后视力0.3~0.5,均较术前明显提高。
严重的ACO纤维膜较厚,与前囊紧密粘连,使用传统的方法难以有效去除,强行剥除易造成囊膜撕裂及周围组织损伤;而轮辐状放射切开法操作简单,能有效清除影响视力的中央部浑浊,不强行撕扯纤维膜,保证了手术安全性。
[参考文献]
[1] Wormstone IM. Eldred JA: Experimental models for posterior capsule opacification research[J].Exp Eye Res,2016(142):2-12.
[2] Aose M, Matsushima H, Mukai K,et al.Influence of intraocular lens implantation on anterior capsule contraction and posterior capsule opacification[J].J Cataract Refract Surg, 2014, 40(12):2128-2133.
[3] Johansson B.Glistenings, anterior/posterior capsular opacification and incidence of Nd:YAG laser treatments with two aspheric hydrophobic acrylic intraocular lenses-a long-term intra-individual study[J].Acta Ophthalmol, 2017.
[4] Kahraman G, Schrittwieser H, Walch M,et al.Anterior and posterior capsular opacification with the Tecnis ZCB00 and AcrySof SA60AT IOLs: a randomised intraindividual comparison[J].Br J Ophthalmol, 2014, 98(7):905-909.
[5] Wang YL, Wang ZZ, Zhao L,et al.Finite element analysis of neodymium: yttrium-aluminum-garnet incisions for the prevention of anterior capsule contraction syndrome[J].Chin Med J (Engl),2013, 126(4):692-696.
[6] Balestrazzi A, Malandrini A, Martone G,et al.Capsule contraction syndrome with a microincision foldable hydrophilic acrylic intraocular lens: two case reports and review of the literature[J].Case Rep Ophthalmol,2014, 5(3):329-335.
[7] Zhang K, Zhu X, Chen M,et al.Elevated Transforming Growth Factor-beta2 in the Aqueous Humor: A Possible Explanation for High Rate of Capsular Contraction Syndrome in High Myopia[J].Journal of ophthalmology,2016(7):1-6.
[8] Page TP, Whitman J.A stepwise approach for the management of capsular contraction syndrome in hinge-based accommodative intraocular lenses[J].Clin Ophthalmol, 2016(10):1039-1046.
[9] Panagopoulos A, Chalioulias K, Kirkby GR. A new approach in the surgical management of anterior capsular phimosis syndrome[J].Ophthalmic Res, 2009(42):221-223.
[10] Yeh PC, Goins KM, Lai WW. Managing anterior capsule contraction by mechanical widening with vitrector-cut capsulotomy[J].J Cataract Refract Surg, 2002(28):217-220.
(收稿日期:2017-02-14)
