雷莫司琼与昂丹司琼预防成人术后恶心呕吐的Meta分析
2017-07-09张忠华张光涛李蕴潜
张忠华 张光涛 李蕴潜
术后恶心呕吐(PONV)是术后最常见的并发症之一[1-9]。有关研究表明术后恶心呕吐的发生率为1%~43%[1-2,4,7-8]。术后恶心呕吐的发生于手术类型、手术时间、麻醉方法、性别、年龄、体质量、饮食习惯、既往术后呕吐及孕吐的病史等因素有关[1-2,4-8]。术后恶心呕吐可造成许多临床并发症,如伤口崩裂、Mallory-Weiss综合征、食道裂孔疝、乏力、脱水以及水电解质紊乱等[1-3,7]。由于麻醉后患者气道反应减低,呕吐还可造成吸入性肺炎[2,7]。另外,术后恶心呕吐还会使住院时间延长,住院费用增加[1,7-8]。迄今为止,已有多种止吐药应用于临床预防或治疗术后恶心呕吐,但尚缺乏一种普遍有效的药物以及标准的用药方案[7-10]。
目前,5羟色胺受体拮抗药为最常用的预防术后恶心呕吐的药物。然而这一类药物在药代动力学和药效动力学上存在相当大的差异。通过文献检索可检索到比较不同5羟色胺受体拮抗药物疗效的多项研究,但不同的研究并未得出相同的结论。本研究试图用Meta分析的方法系统性地比较两个最常用的5羟色胺受体拮抗药,即雷莫司琼和昂丹司琼,预防术后恶心呕吐的疗效。
资料与方法
一、纳入与排除标准
为获取符合要求的文献,在检索之前制定了文献的纳入与排除标准。
1.纳入标准:(1)直接比较雷莫司琼(0.3 mg)和昂丹司琼(4 mg)预防术后恶心呕吐的有效性;(2)随机对照实验研究;(3)能够提取术后恶心呕吐(PONV)在某一时间段的发生率。
2.排除标准如下:(1)研究对象不是成年患者;(2)实验设计不严谨;(3)相关数据无法提取。
二、检索策略
通过计算机检索PubMed/Medline、Web of Science、Cochrane Library、Google scholar等数据库,搜集关于用姜预防术后恶心呕吐的文献。应用的检索词为“ramosetron,YM 060,nasea,ondansetron,SN-307,GR38032F, Zofran,PONV,POV,nausea,vomiting,and postoperative nausea and vomiting”。为防止漏检,再进行手工检索。最后1次检索于2015年5月10日进行。
三、文献质量的评价
对随机对照研究,应用Jadad量表[11]来评价满足纳入排除标准的随机对照研究。如果得分≥4分标记为“A”,≤3分则标记为“B”。这一过程由2名研究者分别独立完成。
四、统计指标与统计学分析
提取和分析的数据为固定时间段内术后恶心呕吐的发生率。统计学方法:数据为二分变量,采用R统计(R-3.1.3)软件Meta程序包对数据进行分析。用固定效应模型(无异质性或异质性在可接受范围内时)或随机效应模型(异质性较大时)分析数据,用相对风险(Relative Risk,RR)及其95%可信区间(Confidence Interval,CI)对结果进行描述。如果P≤0.05,则认为差异有统计学意义。应用Q检验(若P<0.10,则表示研究间存在异质性)和I2检验(I2>50%表示研究间的异质性较大)来评估纳入文献的异质性程度。采用Begg检验及Egger检验评估纳入文献的偏倚(P≤0.05说明发表偏倚明显)。
结 果
一、文献筛选与病例资料
应用检索策略总共检索到132篇文献,通过筛选,最后确定12篇合格的文献[12-23]。具体检索流程见图1。研究对象共计1 150例,其中雷莫司琼组577例,昂丹司琼组573例。各研究基本信息总结见表1~2。
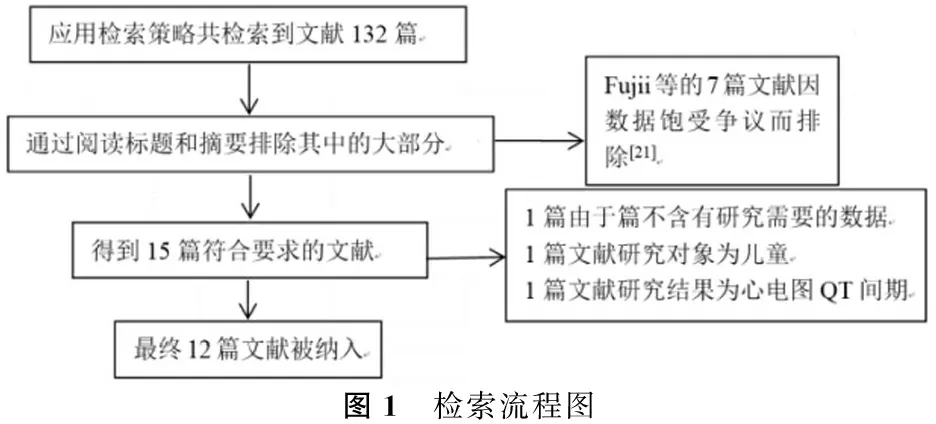
图1 检索流程图
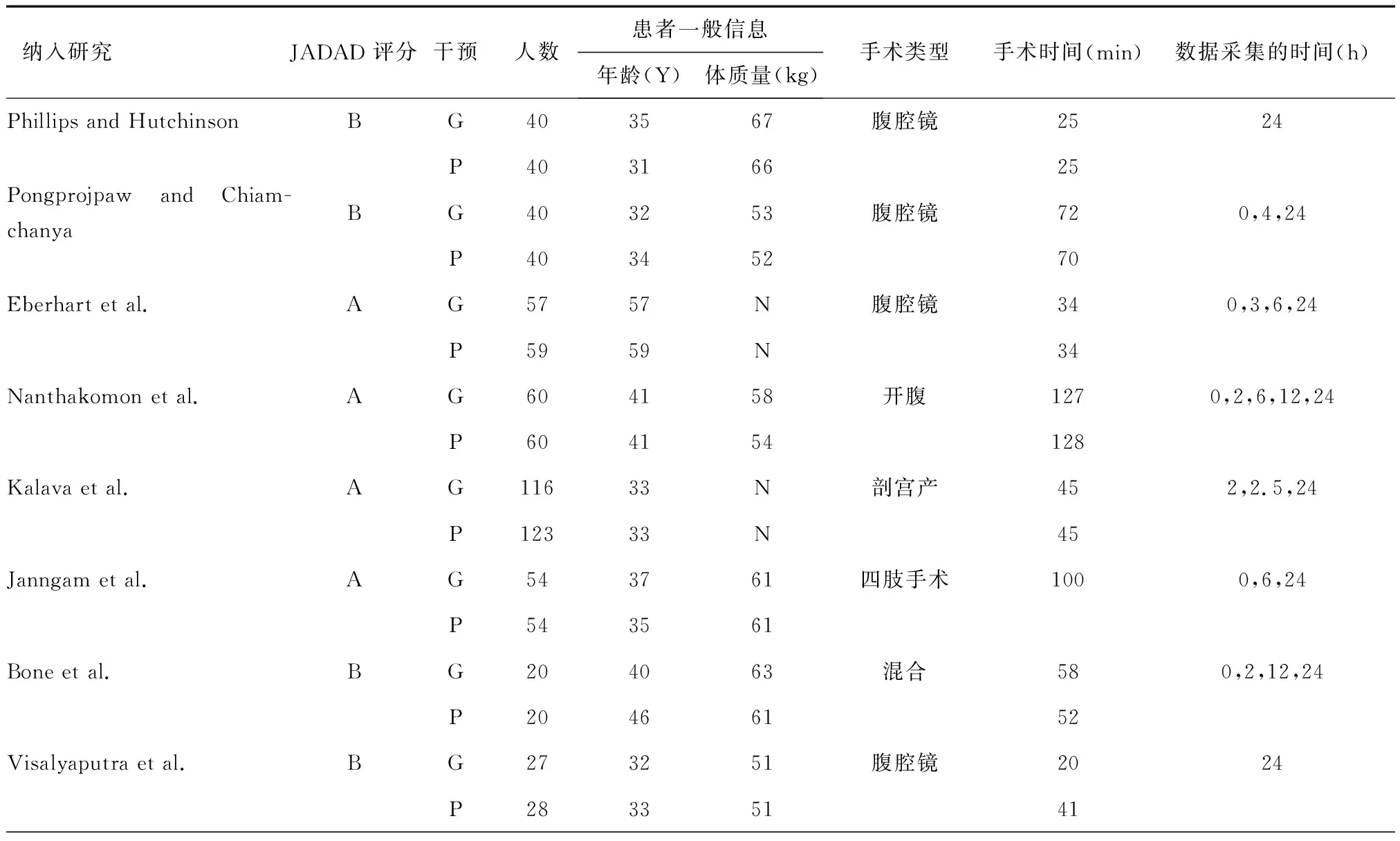
表1 纳入研究的基本信息
注:G表示观察组(姜,ginger);P表示对照组(安慰剂,placebo);N表示数据未报道或无法提取
二、结果分析
为了减少研究间的异质性,严格规定了药物的剂量并且选取了固定的收集数据的时间。规定的药物剂量为雷莫司琼0.3 mg、昂丹司琼4 mg。根据纳入文献的特点,选取的时间段为术后0~2 h、6~24 h、24~48 h。
纳入的12篇文献中分别有5篇文献报道了术后0~2 h恶心呕吐的发生率,7篇文献报道了术后6~24 h恶心呕吐的发生率,9篇文献报道了术后24~48 h恶心呕吐的发生率。分析结果表明,在术后3个时间段雷莫司琼组术后恶心呕吐的发生率均低于昂丹司琼组,差异有统计学意义(P<0.05)。(0~2 h:RR=0.56,CI为0.36~0.87,P=0.009 9;异质性检验P=0.100 1,I2=48.6%;6~24 h:RR=0.80,CI为0.66~0.96,P=0.021 1;异质性检验P= 0.098 1,I2=43.9%;24~48 h:RR=0.65,CI为0.51~0.82,P=0.000 3;异质性检验P=0.141 5,I2=34.5%)。见图2~4。
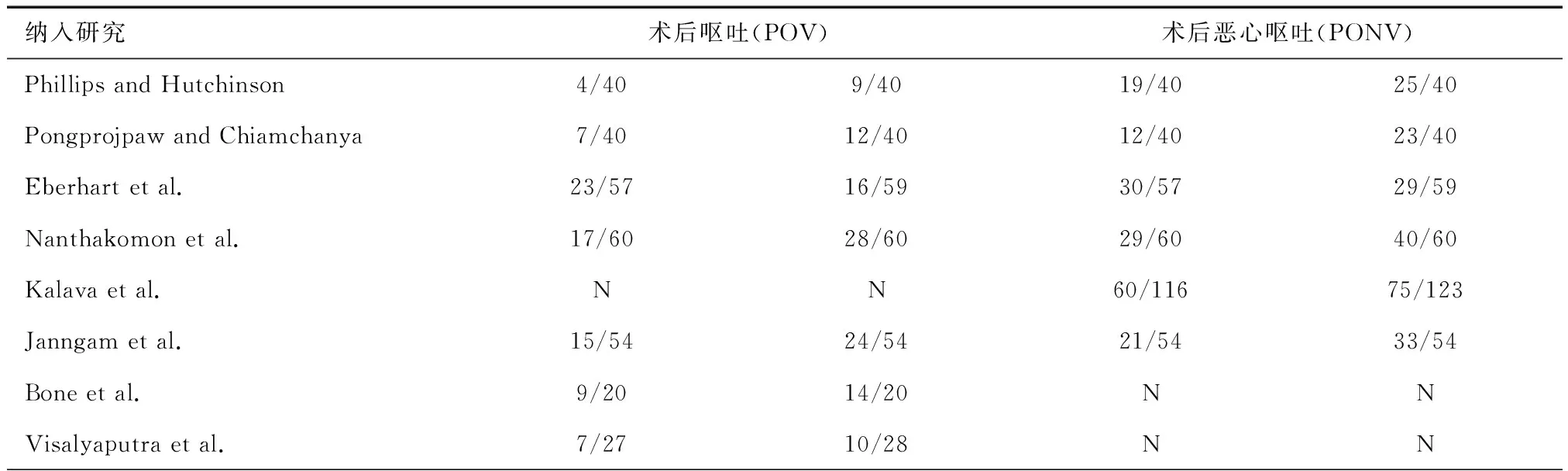
表2 纳入研究的实验结果
注:N表示数据未报道或无法提取
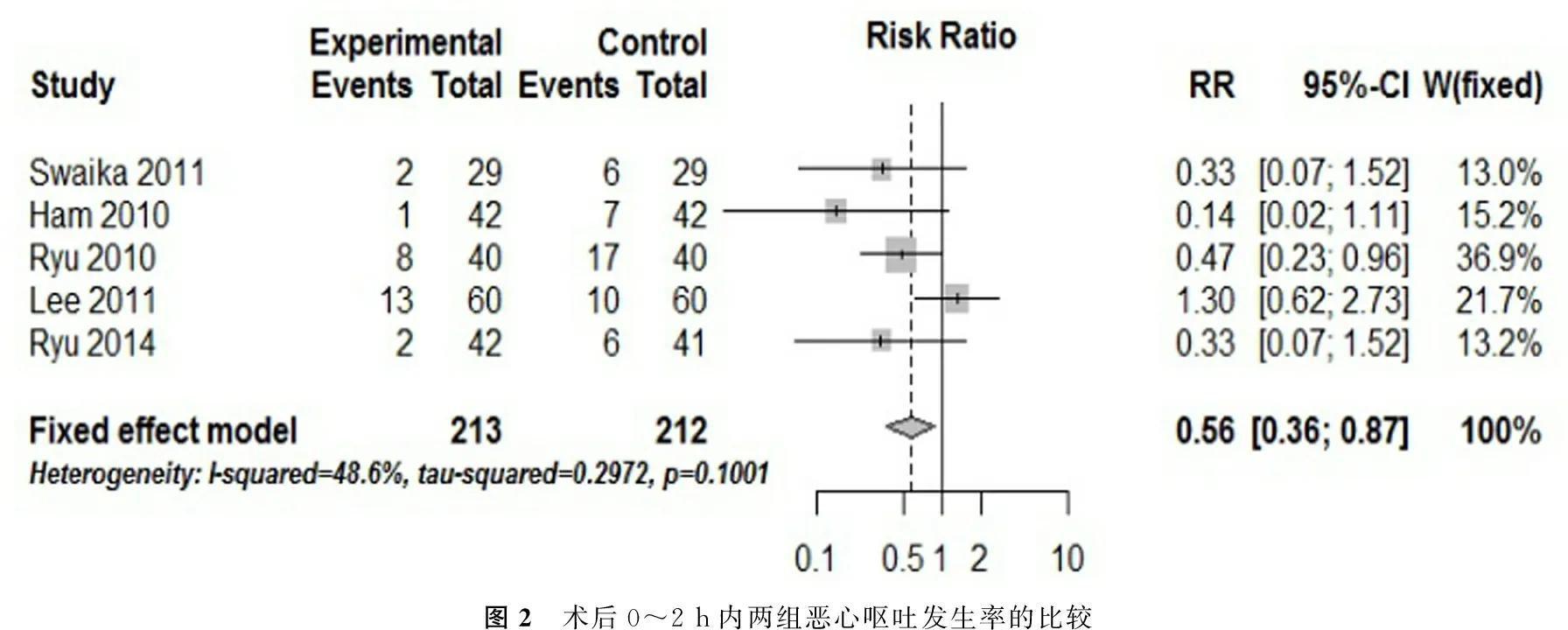
图2 术后0~2 h内两组恶心呕吐发生率的比较
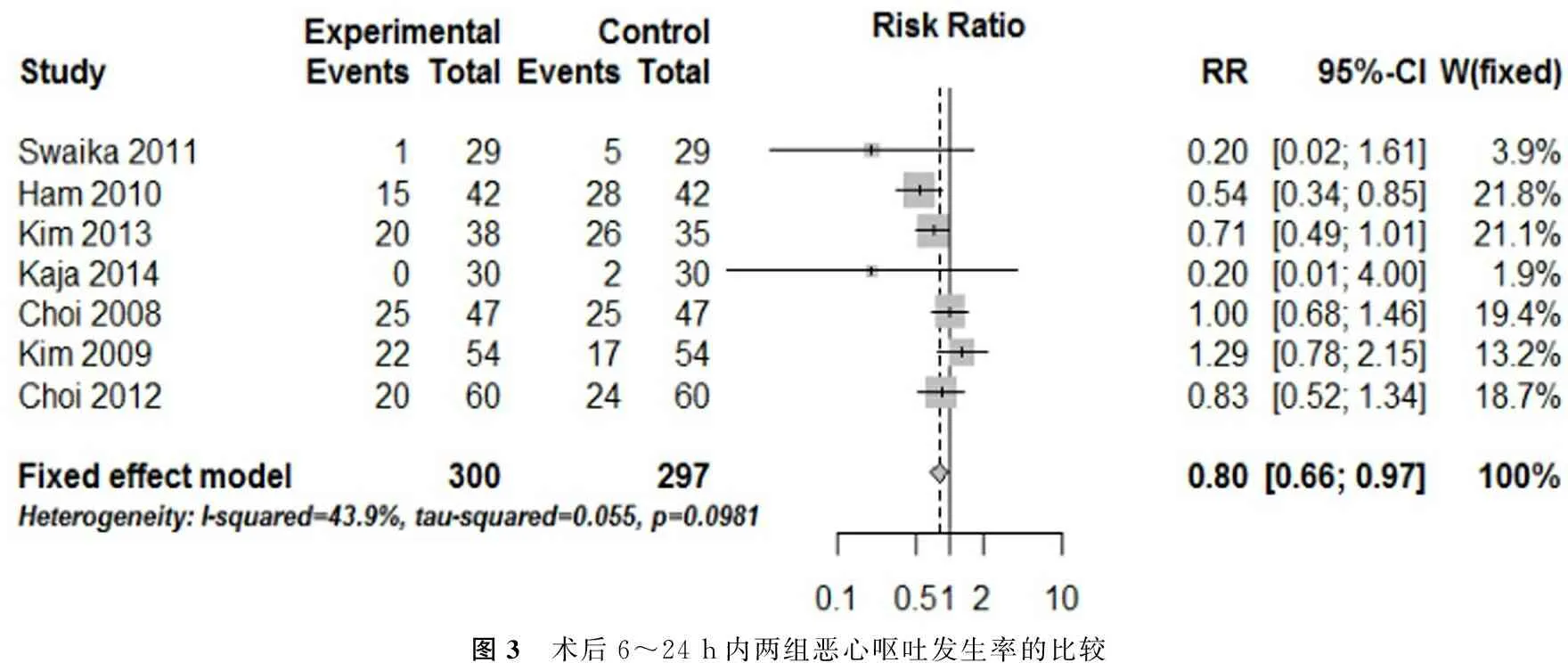
图3 术后6~24 h内两组恶心呕吐发生率的比较
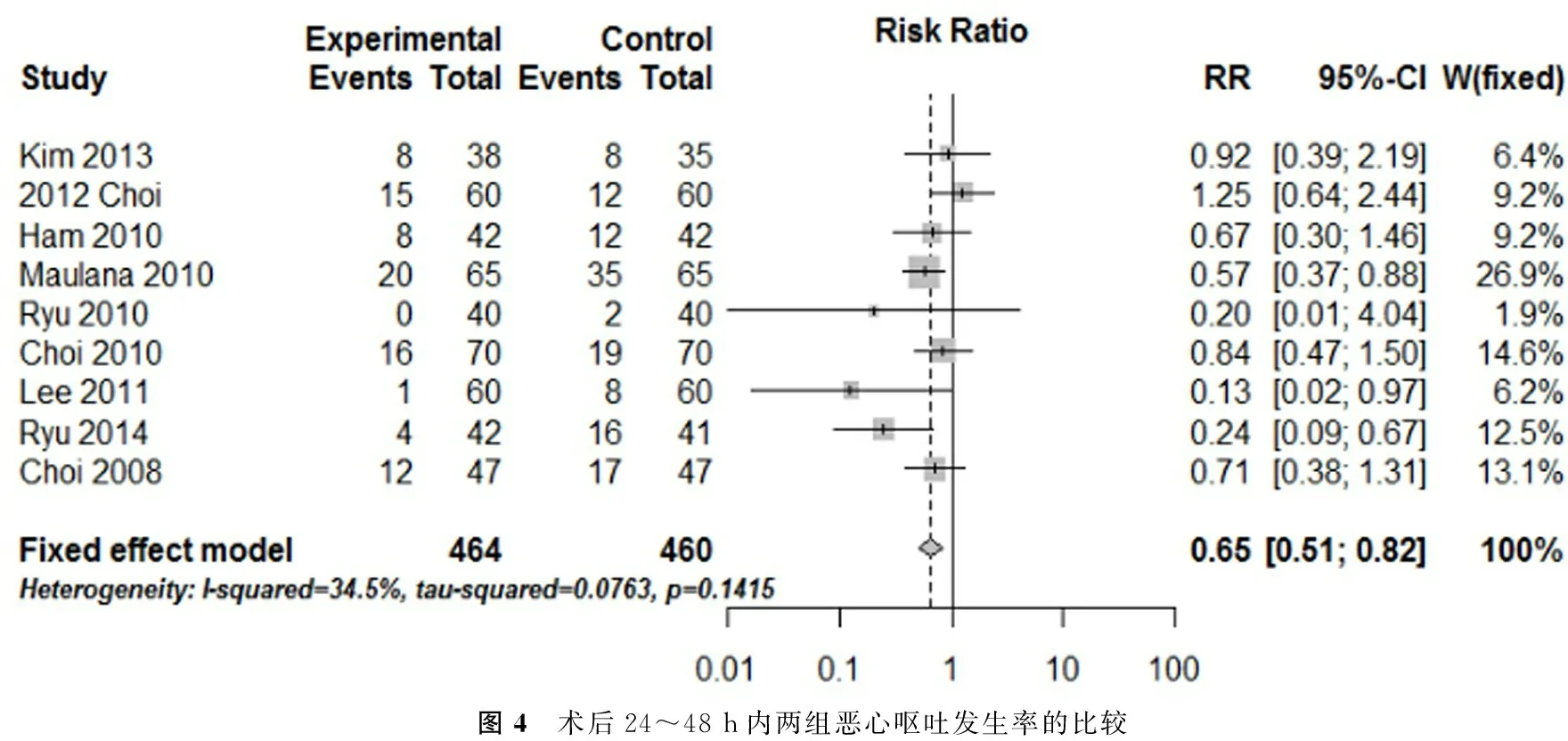
图4 术后24~48 h内两组恶心呕吐发生率的比较
三、发表偏倚
纳入文献的Begg检验及Egger检验结果各组数据均未见明显的发表偏倚。见表3。
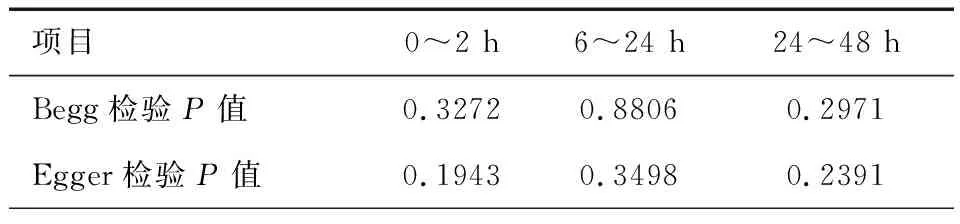
表3 各组数据偏倚的评价
讨 论
本研究比较了两个常用的5羟色胺拮抗剂雷莫司琼和昂丹司琼应用于预防术后恶心呕吐的作用。研究结果表明,在所选取的时间段内,应用雷莫司琼0.3 mg预防术后恶心呕吐的作用强于昂丹司琼。
目前已有多种5羟色胺拮抗剂应用与临床用用来预防术后恶心呕吐的发生。普遍认为5羟色胺拮抗剂有相似的作用机制,即选择性地与5羟色胺受体结合,并且认为这类药物彼此作用效果和安全性相当。在这类药物中,发现最早研究最多的是昂丹司琼有文献报道,雷莫司琼与5羟色胺受体的亲和力较强,这就导致了与之前研制的5羟色胺拮抗剂比较,雷莫司琼的止吐效果较强,止吐作用持续时间较长。(hahm9~20)并且与昂丹司琼比较,雷莫司琼的半衰期较长。
5羟色胺拮抗剂最常见的不良反应为头痛、眩晕、嗜睡。
本篇Meta分析的限制性:Meta分析的质量受限于所纳入文献的质量,本篇研究纳入的文献相对较少,较小的样本数。
[1] Islam S, Jain PN. Post-operative nausea and vomiting (PONV):a review article[J]. Indian Journal of Anaesth 2004;48:253-8.
[2] Haynes G R, Bailey M K. Postoperative nausea and vomiting: review and clinical approaches[J]. Southern medical journal, 1996, 89(10): 940-949.
[3] vanWijk MG, Smalhout B. A postoperative analysis of the patient′s viewof anaesthesia in a Netherlands′ teaching hospital.[J]. Anaesthesia, 1990,45(8):679-682.
[4] Gan TJ. Postoperative nausea and vomiting—Can it be eliminated?[J].Jama, 2002, 287(10): 1233-1236.
[5] Korttila K. The study of postoperative nausea and vomiting[J]. British journal of anaesthesia, 1992, 69(7): 20S-23S.
[6] Apfel CC, Roewer N. Postoperative nausea and vomiting[J]. Der Anaesthesist, 2004, 53(4): 377-89; quiz 390-1.
[7] McCracken G, Houston P, Lefebvre G. Guideline for the management of postoperative nausea and vomiting[J]. Journal of obstetrics and gynaecology Canada: JOGC= Journal d'obstetrique et gynecologie du Canada: JOGC, 2008, 30(7): 600-7, 608-16.
[8] Tramèr MR. Treatment of postoperative nausea and vomiting: Betterdata, improved control have been achieved during recent years[J]. BMJ:British Medical Journal, 2003, 327(7418): 762.
[9] Kenny GNC. Risk factors for postoperative nausea and vomiting[J].Anaesthesia, 1994, 49(1): 6-10.
[10] Alkaissi A, Gunnarsson H, Johnsson V, et al. Disturbing postoperative symptoms are not reduced by prophylactic antiemetic treatment in patients at high risk of post‐operative nausea and vomiting[J]. Acta anaesthesiologica scandinavica, 2004, 48(6): 761-771.
[11] Jadad AR, Moore R A, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary?[J].Controlled clinical trials, 1996, 17(1): 1-12.
[12] Kaja S, Giri RS, Tugave DV, et al. A randomized clinical trial comparing the efficacy and safety of ramosetron versus ondansetron in patients undergoing abdominal surgery under general anesthesia[J]. Saudi journal of anaesthesia, 2014, 8(1): 59.
[13] Ryu JH, Lee JE, Lim YJ, et al. A prospective, randomized,double-blind, and multicenter trial of prophylactic effects of ramosetronon postoperative nausea and vomiting (PONV) after craniotomy:comparison with ondansetron[J]. BMC anesthesiology, 2014, 14(1): 1-8.
[14] Choi YS, Shim JK, Ahn SH, et al. Efficacy comparison of ramosetron with ondansetron on preventing nausea and vomiting in high-risk patients following spine surgery with a single bolus of dexamethasone as an adjunct[J]. Korean journal of anesthesiology, 2012, 62(6): 543-547.
[15] Lee JW, Park HJ, Choi J, et al. Comparison of ramosetron′s and ondansetron′s preventive anti-emetic effects in highly susceptible patients undergoing abdominal hysterectomy[J]. Korean journal of anesthesiology, 2011, 61(6): 488-492.
[16] Choi DK, Chin JH, Lee EH, et al. Prophylactic control of post-operative nausea and vomiting using ondansetron and ramosetron after cardiac surgery[J]. Acta anaesthesiologica Scandinavica, 2010, 54(8):962-969.
[17] Ryu J, So YM, Hwang J, et al. Ramosetron versus ondansetron for the prevention of postoperative nausea and vomiting after laparoscopic cholecystectomy[J]. Surgical endoscopy, 2010, 24(4): 812-817.
[18] Ansari MM, Siddiqui OA, Haleem S, et al. Comparison of ramosetron and ondansetron for control of post-operative nausea and vomiting following laparoscopic cholecystectomy[J]. Indian journal of medical sciences, 2010, 64(6): 272.
[19] Hahm TS, Ko JS, Choi SJ, et al. Comparison of the prophylactic anti-emetic efficacy of ramosetron and ondansetron in patients at high-risk for postoperative nausea and vomiting after total knee replacement[J]. Anaesthesia, 2010, 65(5): 500-504.
[20] Kim SI, Kim SC, Baek YH, et al. Comparison of ramosetron with ondansetron for prevention of postoperative nausea and vomiting in patients undergoing gynaecological surgery[J]. British journal of anaesthesia, 2009, 103(4): 549-553.
[21] Choi YS, Shim JK, Jeon DH, et al. Effect of ramosetron on patient-controlled analgesia related nausea and vomiting after spine surgery in highly susceptible patients: comparison with ondansetron[J].Spine, 2008, 33(17): E602-E606.
[22] Kim SH, Hong JY, Kim WO, et al. Palonosetron has superior prophylactic antiemetic efficacy compared with ondansetron or ramosetron in high-risk patients undergoing laparoscopic surgery: a prospective,randomized, double-blinded study[J]. Korean journal of anesthesiology,2013, 64(6): 517-523.
[23] Swaika S, Pal A, Chatterjee S, et al. Ondansetron, ramosetron, or palonosetron: Which is a better choice of antiemetic to preventpostoperative nausea and vomiting in patients undergoing laparoscopic cholecystectomy?[J]. Anesthesia, Essays and Researches, 2011, 5(2): 182.
张忠华,张光涛,李蕴潜.雷莫司琼与昂丹司琼预防成人术后恶心呕吐的Meta分析[J/CD].中华心脏与心律电子杂志,2017,5(3):144-148.
