唐山地区肝硬化并发上消化道出血的病因及临床特点分析
2017-05-13杨美荣张国顺吴贵恺高宝霞
杨美荣, 刘 斌,张国顺, 尚 华, 吴贵恺, 高宝霞
(1 华北理工大学附属医院 a.血液内科; b.消化内科, 河北 唐山 063000; 2 唐山市传染病医院, 河北 唐山 063000;3 唐山市工人医院, 河北 唐山 063000;4 开滦集团有限责任公司医院, 河北 唐山 063000)
唐山地区肝硬化并发上消化道出血的病因及临床特点分析
杨美荣1a, 刘 斌1b,张国顺1b, 尚 华2, 吴贵恺3, 高宝霞4
(1 华北理工大学附属医院 a.血液内科; b.消化内科, 河北 唐山 063000; 2 唐山市传染病医院, 河北 唐山 063000;3 唐山市工人医院, 河北 唐山 063000;4 开滦集团有限责任公司医院, 河北 唐山 063000)
目的 分析唐山地区近5年来肝硬化并发上消化道出血(UGH)的病因及临床特点,为临床治疗提供参考。方法 抽取2011年1月-2016年1月于华北理工大学附属医院、唐山市传染病医院、唐山市工人医院和开滦集团有限责任公司医院住院的肝硬化并发UGH患者共计462例,所有患者均行胃镜检查明确出血病因。研究出血病因与肝功能Child-Pugh分级之间的关系。计数资料组间比较用χ2检验。结果 肝硬化并发UGH的病因中,食管胃底静脉曲张破裂出血占52.16%;门静脉高压性胃病占27.71%;肝源性溃疡占11.04%;急性胃黏膜病变占4.11%;混合型占3.25%;其他占1.73%。不同病因患者之间,肝功能Child-Pugh B级、C级和A级相比较,差异有统计学意义(χ2=30.12,P=0.007)。结论 肝硬化并发UGH的病因中,食管胃底静脉曲张破裂出血所占的比例最高,其次为门静脉高压性胃病。出血病因与肝功能Child-Pugh分级具有一定关系。
肝硬化; 胃肠出血; 临床特点
上消化道出血(upper gastrointestinal hemorrhage, UGH)是指屈氏韧带以上的消化道,包括食管、胃、胃空肠吻合术后的空肠、十二指肠或胰胆等病变引起的出血,是失代偿期肝硬化最常见的并发症,也是消化系统急危重症之一。主要临床表现为呕血和黑便,起病急、预后差、病死率高,其中40%~70%的患者由于首次出现而死亡[1]。本文对肝硬化并发UGH患者进行了回顾性研究,以期了解其病因及临床特点。
1 资料与方法
1.1 研究对象 抽取2011年1月-2016年1月于华北理工大学附属医院、唐山市传染病医院、唐山市工人医院和开滦集团有限责任公司医院住院的肝硬化并发UGH患者共计462例,男275例,女187例,男女比为1.47∶1;年龄31~76岁,平均(58.34±11.52)岁。纳入标准:(1)经病史、症状和体征,B超或CT等辅助检查确诊为肝硬化,诊断均符合《慢性乙型肝炎防治指南(2015年版)》[2]、《丙型肝炎防治指南(2015年版)》[3]与《酒精性肝病诊疗指南(2010年版)》[4];(2)均为肝硬化基础上出现的UGH。诊断标准:(1)UGH的主要症状为呕血或黑便,化验大便分析:潜血阳性;(2)出血的确诊依靠食管胃十二指肠镜检查。排除标准:(1)进食食物导致的黑便;(2)心肝肾等重要脏器的功能异常;(3)消化系统肿瘤引起的出血。
1.2 治疗方法 所有患者于入院后24~48 h内行胃镜检查,对于大出血、休克等病情危重的患者,先给予输血、补充血容量、抗休克等治疗,待病情稳定后,再行胃镜检查。食管静脉曲张的诊断及分度参照《食管胃底静脉曲张内镜下诊断和治疗规范试行方案》[5]。门静脉高压性胃病的诊断参照Mc Cormack标准[6]。
1.3 统计学方法 采用SPSS19.0统计学软件处理数据。计数资料组间比较用χ2检验。P<0.05为差异有统计学意义。
2 结果
2.1 肝硬化并发UGH的病因分布 462例患者中,食管胃底静脉曲张破裂出血241例(其中203例为食管静脉曲张,38例为食管和胃底静脉曲张),占52.16%;门静脉高压性胃病128例,占27.71%;肝源性溃疡出血51例(胃溃疡24例,十二指肠溃疡21例,复合性溃疡6例),占11.04%;急性胃黏膜病变19例,占4.11%;混合型(静脉曲张破裂出血同时又合并有溃疡出血)15例,占3.25%;其他8例,占1.73%。
2.2 临床表现 217例患者以呕血为主要表现,占46.97%;125例患者以黑便为主要表现,占27.06%;120例患者呕血同时伴有黑便,占25.97%。
2.3 出血病因与肝功能之间的关系 不同肝硬化并发出血的病因之间其肝功能Child-Pugh分级分布,差异有统计学意义(χ2=30.12,P=0.007)(表1)。
3 讨论
肝硬化患者由于门静脉高压的存在,侧支循环的广泛形成,食管胃底静脉曲张破裂出血成为其常见的并发症[7]。有研究[8-11]显示肝硬化并发UGH病因中,食管胃底静脉曲张破裂出血占50%~80%,是导致肝硬化患者死亡的主要原因之一;临床表现以呕血为主。随着近年来胃镜技术的发展,不少患者临床表现以呕吐咖啡样物质为主,为非静脉曲张破裂出血[12],主要以门静脉高压性胃病和肝源性溃疡为常见,占30%~40%[13]。此外,肝源性胃肠功能衰竭、胃窦毛细血管扩张症以及异位静脉曲张等也可导致UGH的发生[14]。因此积极探寻肝硬化并发UGH的病因以及临床特点,有助于临床医师针对性个体化治疗,改善患者的预后。
门静脉高压性胃病是指门静脉高压引起的、胃黏膜屏障破坏导致的胃黏膜病变,好发于近端胃体及胃底,马赛克征或蛇皮样改变是其镜下主要特征。无论何种原因引起门静脉高压,将促使门静脉高压性胃病、食管胃底静脉曲张的形成,二者可单独存在或共存[15]。目前发病机制考虑与门静脉压力升高引起胃黏膜血管扩张,血液淤积、循环血量不足,胃黏膜屏障破坏以及肝功能恶化导致肝脏灭活作用下降等有关。临床多表现为隐匿性出血,病情危重时,可危及患者生命。
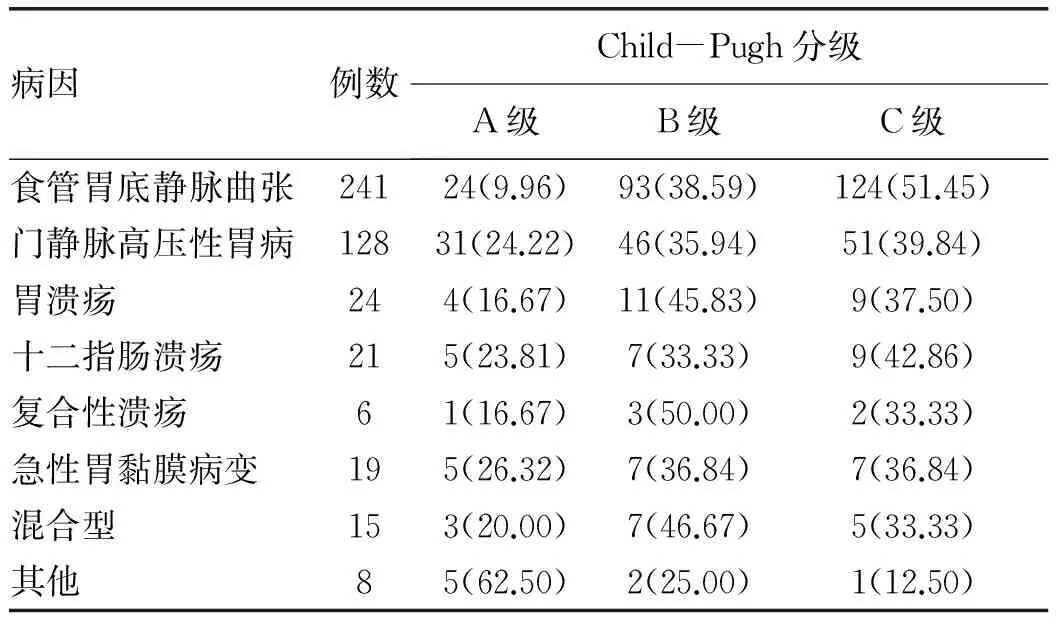
表1 不同病因患者肝功能比较 [例(%)]
本研究发现引起UGH的前4位病因分别是:食管胃底静脉曲张、门静脉高压性胃病、肝源性溃疡、急性胃黏膜病变;以食管胃底静脉曲张为主要病因,与相关文献[8]相符,提示出血病因与肝功能Child-Pugh分级有一定关系。UGH考虑与静脉曲张程度、静脉壁的厚度以及门静脉压力等有关。随着肝硬化病程延长,病情进行性加重,肝损伤日趋严重,肝功能Child-Pugh分级增加,肝脏血窦正常结构破坏加重,引起门静脉血液回流障碍,门静脉压力增加,胃上部侧支循环的血液增多,食管静脉曲张,管壁变薄,最终发生破裂出血。随着肝功能恶化,出血发生的概率将增加,患者预后越差。
肝硬化并发UGH病情危急,变化迅速,补充血容量、抗休克是治疗的关键措施。非选择性β受体阻滞剂、奥曲肽等是临床常用的药物;此外,内镜硬化治疗、气囊压迫止血等亦可用于止血治疗,病情危重时,也可行外科手术[16-17]。由于肝硬化是一种进展性疾病,保护肝功能,去除或减轻肝硬化病因对于预防出血是十分重要的。
综上所述,由于静脉曲张和非静脉曲张破裂出血的治疗方案不同,患者的预后也有所差异。治疗关键在于尽早行胃镜检查,明确出血原因,便于指导临床采取最佳的治疗方案,对于抢救患者生命,提高生活质量,改善预后具有重要的临床意义。
[1] AMITRANO L, GUARDASCIONE MA, MANGUSO F, et al .The effectivness of current acute variceal bleed treatments in unselected cirrhotic patients:refining short-term prognosis and risk factors[J]. Am J Gastroenterol, 2012, 107(12): 1872-1878.
[2] Chinese Society of Hepatology and Chinese Society of Infectious Diseases, Chinese Medical Association. The guideline of prevention andtreatment for chronic hepatitis B: a 2015 update[J]. J Clin Hepatol, 2015, 31(12): 1941-1960. (in Chinese) 中华医学会肝病学分会,中华医学会感染病学分会. 慢性乙型肝炎防治指南(2015年更新版)[J]. 临床肝胆病杂志, 2015, 31(12): 1941-1960.
[3] Chinese Society of Hepatology and Chinese Society of Infectious Diseases, Chinese Medical Association. The guideline of prevention and treatment for hepatitis C: a 2015 update[J]. J Clin Hepatol, 2015, 31(12): 1961-1979. (in Chinese) 中华医学会肝病学分会, 中华医学会感染病学分会. 丙型肝炎防治指南(2015年更新版)[J]. 临床肝胆病杂志, 2015, 31(12): 1961-1979.
[4] Fatty Liver and Alcoholic Liver Disease Study Group of the Chinese Liver Disease Association, Chinese Medical Association.Guidelines for prevention and treatment of alcoholic liver disease (revised version 2010)[J]. J Clin Hepatol, 2010, 26(3): 229-232.(in Chinese) 中华医学会肝病学分会脂肪肝和酒精性肝病学组. 酒精性肝病诊疗指南(2010年修订版)[J]. 临床肝胆病杂志, 2010, 26(3): 229-232.
[5] Chinese Society of Digestive Endoscopy. A scheme for endoscopic diagnosis and treatment of esophageal and gastric varices[J]. Chin J Dig Endosc, 2000, 17(4): 498.(in Chinese) 中华消化内镜学分会. 食管胃底静脉曲张内镜下诊断和治疗规范试行方案[J]. 中华消化内镜杂志, 2000, 17(4): 498.
[6] NG NB, KARTHIK SV, AW MM, et al. Endoscopic evaluation in children with end-stage liver disease-associated portal hypertension awaiting liver transplant[J]. J Pediatr Gastroenterol Nutr, 2016, 63(3): 365-369.
[7] WU CS, ZHANG L, ZHOU W, et al. A clinical observation of hepatic vein pressure gradient and flow rate after Octreotide treatment of bleeding esophageal varices[J]. Chin J Clin Pharmacol Ther, 2015, 20(4): 441-444. (in Chinese) 吴春松, 张玲, 周玮, 等. 奥曲肽治疗对食管胃底静脉曲张出血的肝静脉压力梯度及血流速度的影响[J]. 中国临床药理学与治疗学, 2015, 20(4): 441-444.
[8] LIU B, ZHANG GS, YANG MR, et al. Risk factors for gastroesophageal variceal bleeding and portal vein thrombosis in patients with liver cirrhosis[J]. World Chin J Dig, 2016, 24(18): 2892-2897.(in Chinese) 刘斌, 张国顺, 杨美荣, 等. 肝硬化并发食管胃底静脉曲张破裂出血与门静脉血栓形成的危险因素[J]. 世界华人消化杂志, 2016, 24(18): 2892-2897.
[9] YANG MR, ZHANG GS, LIU B, et al. Analysis of the influence factors of cirrhosis complicated with upper gastrointestinal hemorrhage[J]. Clin Med China, 2016, 32(3): 235-238. (in Chinese) 杨美荣, 张国顺, 刘斌, 等. 肝硬化患者并发上消化道出血的影响因素分析[J]. 中国综合临床, 2016, 32(3): 235-238.
[10] GAO CG, XIE F, FENG YD. Effect of somatostatin combined with pantoprazole in treatment of liver cirrhosis with upper gastrointestinal hemorrhage[J].J Clin Hepatol, 2016, 32(2): 284-287.(in Chinese) 高成广, 谢峰, 冯亚东. 生长抑素联合泮托拉唑治疗肝硬化合并上消化道出血的效果观察[J]. 临床肝胆病杂志, 2016, 32(2): 284-287.
[11] HOU Y. The clinical comparison of cirrhosis patients with different etiological upper digestive tract hemorrhage[J]. J Clin Exp Med, 2015, 14(12): 999-1001.(in Chinese) 侯昀.肝硬化不同病因上消化道出血患者的临床对比[J]. 临床和实验医学杂志, 2015, 14(12): 999-1001.
[12] MAROT A, TRÉPO E, DOERIG C, et al. Liver stiffness and platelet count for identifying patients with compensated liver disease at low risk of variceal bleeding[J]. Liver Int, 2016, 11(18): 1428-1431.
[13] LI XL, CHEN MS, GAN QR, et al. Risk factors for antibiotic prophylaxis failure in patients with liver cirrhosis and upper gastrointestinal bleeding[J]. J Clin Hepatol, 2016, 32(2): 288-291.(in Chinese) 李孝楼, 陈明胜, 甘巧蓉, 等. 肝硬化上消化道出血预防性抗感染治疗失败的影响因素[J]. 临床肝胆病杂志, 2016, 32(2): 288-291.
[14] WU KC. Interpretation of experts' consensus on non variceal upper gastrointestinal bleeding in Asia Pacific Region (three): Remedial measures for endoscopic hemostasis[J]. Chin J Dig, 2012, 32(2): 82-83.(in Chinese) 吴开春. 亚太地区非静脉曲张性上消化道出血专家共识意见解读(三):内镜止血的补救措施[J]. 中华消化杂志, 2012, 32(2): 82-83.
[15] TOUARSA F, NASSAR I, AJANA A, et al. Upper gastrointestinal bleeding in portal hypertensive gastropathy reveals a wandering spleen[J]. Presse Med, 2016, 45(10): 935-937.
[16] HANAFY AS, EI HAWARY AT. Efficacy of argon plasma coagulation in the management of portal hypertensive gastropathy[J]. Endosc Int Open, 2016, 4(10): e1057-e1062.
[17] ACHIM AC, VESA SC, DUMITRU E. The efficacy of virtual chromoendoscopy in the diagnosis of portal hypertensive gastropathy[J]. J Gastrointestin Liver Dis, 2016, 25(3): 289-293.
引证本文:YANG MR, LIU B, ZHANG GS, et al. Causes and clinical features of liver cirrhosis complicated by upper gastrointestinal bleeding in Tangshan, China[J]. J Clin Hepatol, 2017, 33(3): 476-478. (in Chinese)
杨美荣, 刘斌, 张国顺, 等. 唐山地区肝硬化并发上消化道出血的病因及临床特点分析[J]. 临床肝胆病杂志, 2017, 33(3): 476-478.
(本文编辑:朱 晶)
Causes and clinical features of liver cirrhosis complicated by upper gastrointestinal bleeding in Tangshan, China
YANGMeirong,LIUBin,ZHANGGuoshun,etal.
(DepartmentofHematology,TheAffiliatedHospitalofNorthChinaUniversityofScienceandTechnology,Tangshan,Hebei063000,China)
Objective To investigate the causes and clinical features of liver cirrhosis complicated by upper gastrointestinal bleeding in Tangshan, China in the past 5 years, and to provide a reference for clinical treatment. Methods A total of 462 patients with liver cirrhosis complicated by upper gastrointestinal bleeding who were hospitalized in The Affiliated Hospital of North China University of Science and Technology, Tangshan Municipal Hospital of Infectious Diseases, Tangshan Workers′ Hospital, and The Affiliated Hospital of Kailuan Group Limited Liability Corporation were enrolled, and all the patients underwent gastroscopy to clarify the cause of bleeding. The association between the cause of bleeding and Child-Pugh class was analyzed. The chi-square test was used for comparison of categorical data. Results Among the causes of liver cirrhosis complicated by upper gastrointestinal bleeding, esophagogastric variceal bleeding, portal hypertensive gastropathy, hepatogenic ulcer, acute gastric mucosal lesion, and mixed type accounted for 52.16%, 27.71%, 11.04%, 4.11%, and 3.25%, respectively, and other causes accounted for 1.73%. There were significant differences in Child-Pugh class between the patients with different causes (χ2=30.12,P=0.007). Conclusion Among the causes of liver cirrhosis complicated by upper gastrointestinal bleeding, esophagogastric variceal bleeding is the most common one, followed by portal hypertensive gastropathy. The cause of bleeding is associated with Child-Pugh class.
liver cirrhosis; gastrointestinal hemorrhage; clinical features
10.3969/j.issn.1001-5256.2017.03.016
2016-10-31;
2016-12-07。
国家自然科学基金项目(81370477)
杨美荣(1975-),女,主治医师,主要研究血液消化系统疾病。
R575.2
A
1001-5256(2017)03-0476-03