Intensive patient—doctor relationship in China
2017-03-24ChengJiangSiriTel
Cheng+Jiang+Siri+Tellier


1 Background of Chinese Health System
1.1 Track of Chinese health system reform
In the past 30 years, Chinese health system experienced 5 stages of reforming. From 1978 to 1984, in the background of economic reform since 1978, China entered upon the first stage of health reform, which was more like an incubation period of recovering and completing the weak health system rather than substantive reforming. [6] 1985-1992, influenced by the economic reform, Chinese government introduced market economic model to cut the investment on health care, which started the health insurance transaction to parts of out-of-pocket medical costs from free public medical care. [6] At the third stage of health system reform, 1992-2000, the main objective of this reform was to hence the quality of health services. It is because that government had to face the complaint on the increase about the health care quality from the patients. During the last stage, health sectors started to transform to market-oriented, which had caused the increase the proportion of out-of-pocket money and the decrease of health quality. 2000-2005, in the forth stage, it contributed to the first step of reform of health institution property rights. Accompanied with deepening market-based economic reform, various conflicts from different social groups woke up after the breaking of SARS (Severe Acute Respiratory Syndromes) in 2003. In 2005, it was reported that Chinese government admitted the failure of the past health care reform. [6] A new reform based on the lessons was built up and have been being completed since then. In 2009, the State Council announced the goal to achieve universal health care coverage by 2020. [7] At the end of 2011, in Qun Mengs study, the insurance had achieved 95.7% covered already, comparing to the 29.7% covered in 2003. [8] The latest health reform engaged in 5 aspects: service delivery, essential medicines, public health, insurance, and public hospital reform. [9]
In China, the health reform had experienced 30 years, accompanied with the affects by social and economic changing. Meanwhile, the health system including 6 blocks, leadership and governance, financing, service delivery, health workforce, information, medical, products, vaccines and technologies are reconstructing. The interrelationships of impacts among the 6 blocks as well as the social economic factors hampered the effects of health reform, and brought new problems and concerns.
1.2 Key issues in Current health care system:
In spite of the advancement of the latest health care reform in China, it still has to face the conflicts and issues bellow.
No reasonable system for disease burden transitions. As the demographic aging is an unavoidable emergency, chronic diseases have a high prevalence and mortality in aging China. [10] According to WHOs data, Non-communicable diseases (NCDs) are estimated to account for 83% of all deaths in China which holds one fifth of the world population. [39] More over, in January 2012, urban population the first time exceeded the rural population. Urbanization is another social risk factor of Non-communicable diseases (NCDs). [11] However, the health system reform is just starting. The old system under such complicated social economic environment has to face numerous conflicts and needs time to constantly improve. Currently, it seems that the health system could not take responsibilities of such new disease burdens.
Inequality. Health inequality issues are among different population, including populations of different areas, and social-economic statuses. [12] Most studies and policies focused on urban population in big cities like Beijing and Shanghai. Pilots of new policies in rural area prefer to choose Guangdong province, [12] one of which provinces has the highest GDP per capita over the country. [13] It somehow brings the unbalanced development of both economy and health care.
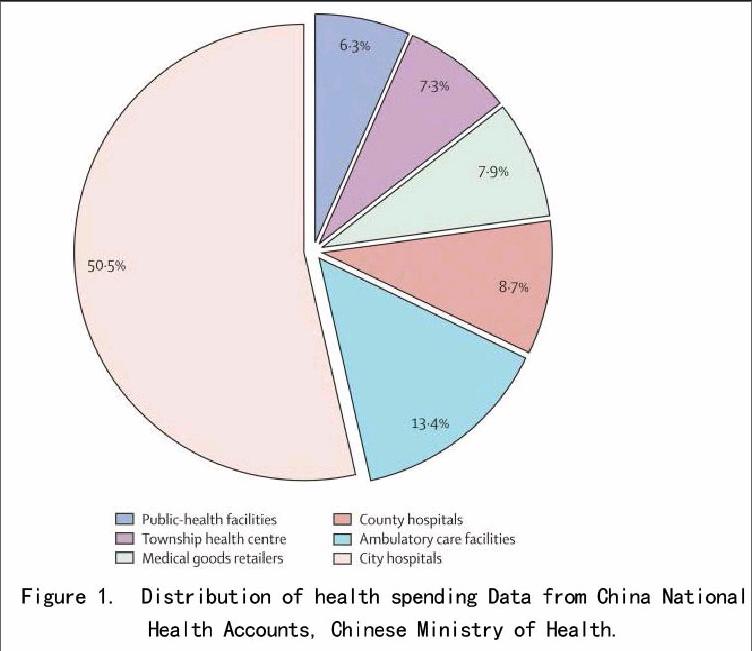
Insufficient health resources and inefficient allocation. In 2011, the Chinese government spends 172.76 billion CNY (1CNY=0.158USD) budget on Health care. [14] It is a huge sum of money. However, comparing to 1.3 billion of population and the rank of GDP per capita mentioned before, [5] 3.18% of the total budget spent on healthcare might be far from enough. [14] In addition, the unbalance exists in allocation. 65% health expenditures went to the secondary and tertiary hospitals. While only 10.8% health expenditures are available for urban communities and rural health sectors. (Figure 1) in 2005. [15] Challenges in Human Resources (HR) management like waste of well skilled health personnel are slowing down the health care progress. [16,17]
Figure 1. Distribution of health spending Data from China National Health Accounts, Chinese Ministry of Health.
Incomplete health structures. As without systematic healthcare rules and long-term policies, government, health sectors, clients and market are not cooperating under a common goal. The incentive mechanism among them is neither stable nor sustainable, most depending on market moving tendency. Over market-based in health care system leads to max interest chasing rather than most benefit health care chasing. It also increases the health care costs without sufficient constraints from governments. For instance, health providers in China are paid on a per-patient-episode basis rather than on a fee-for-service basis like diagnosis-related-grouping programme, which saved 14% costs, 6% stays in hospital, and shifted part of inpatient care to outpatient services compared with facilities out of the programme in South Korea. [18], [19] and [20]
Lack of legislation of public health, evaluation and supervision systems. It is time to formulate public health law in China to complete the Chinese health care system and establish the supervision systems. Public health legislation could be the insurance of benign development of health care. [21]
All the problems existing in Chinese health system contribute to not only health problems but also social issues. Such as the increasingly intensive patient-doctor relationship in China.
2 “Intensive patient-doctor relationship” analysis
Globally, patient satisfaction plays a dominant role in evaluating the quality of medical service and the encounters between medical professional and patient. [22,23,24] In addition, patient satisfaction could not only represent patients assessment of their health services experience but also their perception of the gap between requiring and receiving [25]. In China, the main reason of destroying the relationship is the decreasing patients satisfaction of health service. Analysis could be deduced from the WHO 6 blocks of healthcare system.
2.1 leadership and governance (stewardship)
Whats different from other countries is the one-party system in China, which is the Communist of China. It is a unitary government. The national ministry of health in charge of national health issues is one part of State Council. There are local governments of provinces and several social health organizations directly under the national governance. [26]
In 2005, a new health reforming board was built when facing the failure of last health reform. It is still one part from national MOH. [26]
One challenge of the Chinese health leadership is lacking of an equal power to exam the success of health policies. Policies are made and decided only by MOH. Although ministry of finance and ministry of supervision can supervise the progresses of implementing and finance of health policies, [26] there is no equal right to challenge the benefit or judge the success of the policies.
The other one is that policies are made and implemented from center to local, top to bottom. But issues happen at the bottom. The conflicts between doctors and patients properly reflect the deficiency of policies. As a result of lacking of feedback mechanism and feasible plans at local levels, policies regardless of request from patients and doctors make them the vector under such incomplete health policies.
For quality assurance, China established the law assistant offices under local government. [26] Medias for TV programme and newspapers also complete the supervision mechanism of health service. Generally, society and media are inclined to feel sympathy for the weak, which encourage the patients and society to monitor the quality of health services. At the same time, media and law assistant offices are used in an improper way by someone with purpose of money. [27] Somehow it might be caused by unaffordable health services today. Under such rules, the emotion from doctors to patients are shifting from trying best to treat disease of patients, to avoiding any mistake or complaint from patients. These conflicts may not easy to solve unless completing the whole health system and government.
2.2 financing
Chinese healthcare finance support mainly comes from 2 parts, government budget and social insurance. [28] Social insurance includes urban insurance from the employers and rural new cooperative medical scheme, which completes the huge gap of healthcare insurance coverage and government investment. [29]
As the health reform deeply influenced by market-based economic development, public hospital is at the crossroad of the shifting from public to private ownership. Only 10% of investment for the public health sector comes from government. [30] It means that both public and private hospitals have to survive on their own business, leading to a blind pursuit of profit in result of costs of health service increasing.
Data from China National Health Accounts, Chinese Ministry of Health
On one hand, because of the same issue of inadequate financing support, health providers in China are paid much less than in other countries. [31] The unequal income compared with their work stimulates the desire for extra “bonus”. Some doctors play the roles of “seller” and utilize the “line-item approach” undertaken by some medical companies, which pays a health provider according to the amount of drugs or tests provision, to persuade the patients or clients to take unnecessary expensive test or drugs regardless of quality of health services. [31] Finally, doctors lost the belief from the patients.
On the other hand, either government insurance or social insurance just covers the essential drugs and basic health service. Severe fatal diseases or NCDs like diabetes are not included, which may directly cause the poverty for most households. [30] The out-of-pocket payments for health service are more than 18 times than the payments in 1990. (Figure 2) And high rate compared to other countries (Figure 3) from out-of-pocket money increases the patients requirement of health services quality and treatment results, but unfortunately it is not achieved.
Data from China National Health Accounts, Chinese Ministry of Health
2.3 service delivery
Like most countries, health service delivery is provided by public health sectors, private health sectors, Non-government organization and others. [31] The relationship among them could directly or indirectly influence the quality of health service.
2.3.1 Quality of health services
Quality of medicine and diagnosis obviously advance rapidly attributing to improvement of technology and economic development in China. However, particularly in secondary and tertiary public hospitals, which are the main health service providers in China, doctors rely on high-tech equipments excessively. Distance between doctor and patient widens, and technology adds to finance burden to patients and families. [32]
For the reason that uneven development of primary and higher level health sectors mentioned above, in primary health sectors, considerable health service is not available. While doctors and nurses in secondary and tertiary hospitals are too busy to smile because of high outpatient rate and inpatient rate. Take an example of the First Affiliated Hospital of Sun-yet sun University, which is a comprehensive tertiary hospital in Guangzhou. There are over 4 million outpatient service workloads per year. [32] It is not wild that doctors and nurses in these sectors said no time for them to smile to patients or even go to the toilet. In another word, the unreasonable competition and busy work among doctors today reduced time for them to emotionally communicate with patients.
2.3.2 Affordability, accessibility, and equality of health service
Health costs in China had increased exceeding the per capita income increasing. More than 8-fold in urban areas and 7-fold in rural areas increase on health spending from 1990 to 2002[33]. It reflects the disease burden shifting from infection diseases to chronic diseases based on adoption of new technology and longer treatment. Rapid rising on health care services and limited coverage of health insurance leads to unaffordable for lower income families. [34]
Unsurprisingly, Chinas health system displays considerable inequalities in utilization and outcomes between rural and urban areas and across income groups. [35] Government focuses on treatment rather than prevention. As it mentioned above in quality of health service, inaccessibility exists in both in primary health sectors and higher sectors for contrast reasons.
Unaffordable, inaccessible and unequal health service gradually pushes the patients standing up to the opposite side of health sectors.
2.4 health workforce
The challenges of health workforce in China are uneven payment for health providers related to over working load, and unreasonable HR management in health sectors. High-end talents go abroad under the international HR competition, not only for a higher salary, but also for a better career development. Domestically, qualified and well educated health providers crowd to urban tertiary hospitals for the same reason under the market-oriented Chinese health system, leaving the even short of talents in rural area or primary health sectors. Although government now is trying hard to introduce talents abroad, like “985” “211” programs, providing accommodation and researching fund for high-end talents.[36] It undoubtedly helps developing the medical research in China but rarely does for the retention of clinical medical workers.
Uneven allocation of HR and financing resource worsen the quality and accessibility situation of health service.
In competitive urban hospitals, which mostly are teaching hospitals, doctors and nurses are required to be omnipotent on treatment and teaching as well as research. And because more attention was paid for research by policies, and research weighs more in individual evaluation, the focus of doctors job is moving from treating and caring patients to doing research. [32]
2.5 information
2.5.1 As the information technology develops, more and more Chinese health facilities utilize advanced hospital information system (HIS) to manage and improve efficiency. [37] But the problem is that no uniform database was used. In the long run, it is difficult for the national department to establish a complete health database. For the patient level, it is also inconvenient that different hospitals cannot share the information for the same patient. [40]
2.5.2 Another issue about health information is that the situation of information asymmetry between doctors and patients may be changed. Most patients now in China are well educated. [27] Internet, books and media help people know about disease they concern quickly. Sometimes the authority of the doctors is being challenged. Furthermore, medias for attentions may prefer to report or exaggerate the negative news (e.g. corruption among doctors), and the internet helps the rapid dispersal of it. Doctors become the minority against the majority of compassion for patients, who can represent the most population, in result of alienating the relationship between doctors and patients.
2.6 medical, products, vaccines and technologies
Medical, products, vaccines and technologies develops fast under the market-based economy and with the progress of era as well as people strict request. However, coin has two sides. Under the intensive relationship between doctors and patients, doctors are afraid of taking responsibility of misdiagnosis. Technology is excessively used for unnecessary tests. It also brings the high costs and lower accessibility of health services as mentioned in other blocks.
3 Conclusion
The failure of the past reform and incomplete health system left a lot of social issues to China. Maybe Chinas government could learn from Thailand according to the similar situation to shift more funding to clinics, showing encouraging results in terms of improving Thai health systems. [38]
References:
[1]. “Countries of the world ordered by land area”. http://www.listofcountriesoftheworld.com/area-land.html. Retrieved 27 April 2010.
[2]. Walton, Greg. International Centre for Human Rights and Democratic Development (2001). “Executive Summary”. Chinas golden shield: Corporations and the development of surveillance technology in the Peoples Republic of China. Rights & Democracy. Retrieved in 2009.
[3]. Constitution of the Peoples Republic of China”.Peoples Daily Online. Retrieved 23 November 2009. “Article 138. The capital of the Peoples Republic of China is Beijing.”
[4]. “Output, prices and jobs”. The Economist. 28 January 2012. Retrieved 28 January 2012.
[5]. Altucher, James (8 January 2010). “Theres no stopping China”. New York Post. Retrieved 2 August 2010.
[6]. Chen X, Cao Y. A Study on the Value Orientation and Realization Mechanism of the Reform of Chinas Healthcare System. Shandong University. 2011; 11(in Chinese)
[7]. Communist Party of China Central Committee. State Council.Opinions of the Communist Party of China Central Committee and the State Council on Deepening the Health Care System Reform. Beijing: Government of the Peoples Republic of China, 2009.
[8]. Meng Q, Xu L, Zhang Y, Qian J, Cai M, Xin Y, etc. Trends in access to health services and financial protection in China between 2003 and 2011: a cross-sectional study. The Lancet. 2012; 379: 805-814.
[9]. Communist Party of China Central Committee. State Council implementation plan for the recent priorities of the health care system reform (2009–2011). Beijing: Government of the Peoples Republic of China, 2009.
[10]. who.int[Internet]. Geneva: World Health Organization Online Resources, Inc.; c2011-01 [cited 2012 Jan 19]. Available from: http://www.who.int/chp/chronic_disease_report/media/china.pdf
[11]. Editorial. What can be learned from Chinas health system? The Lancet. 2012;379: 777.
[12]. Zhang X, Kanbur R. Spatial inequality in education and health care in China. China Economic Review. 2005;16(2):189-204.
[13]. OECD, 2010. OECD Territorial Reviews: Guangdong, China 2010. Retrieved: 2011/Jul/19. Available at: doi:10.1787/9789264090088-en.
[14]. www.ihs.com[internet]. Englewood: HIS Online Resources, Inc.; c2012-01[cited 2012 Mar 10]. Available from:http://www.ihs.com/products/global-insight/industry-economic-report.aspx?id=1065929162
[15]. YX Zhao, Q Wan, YZ Ying, SH Zhang. The results of total health expenditure in China in 2005 and financing basic health services. China Health Econ J, 2007;26:10–14.