Cytokines are early diagnostic biomarkers of graft-versus-host disease in liver recipients
2017-02-10
Hangzhou, China
Cytokines are early diagnostic biomarkers of graft-versus-host disease in liver recipients
Xue-Qin Meng, Xin-Hua Chen, Zayd Sahebally, Yu-Ning Xu, Sheng-Yong Yin, Li-Ming Wu and Shu-Sen Zheng
Hangzhou, China
BACKGROUND: Graft-versus-host disease (GVHD) is associated with high mortality. Early diagnosis is essential to start treatment and to improve outcomes. Because of the infammatory nature, we hypothesis that cytokine profle of patients with GVHD may serve as diagnostic markers. The present study was to evaluate the role of cytokine profle in the diagnosis of GVHD.
METHODS: An immunoassay was used to detect 29 cytokines simultaneously in the serum; the measuring sensitivity of allcytokines was pg/mL. Healthy subjects undergoing annual routine physical examinations served as negative controls;23 patients with hepatocellular carcinoma (HCC) who had undergone liver transplantation (the LT group) comprised the test subjects. A total of 22 kidney recipients with biopsyconfrmed GVHD (the RT group) were included for comparison. HCC patients with radical surgery (the HCC group,n=22) served as positive control. The liver contents of the three cytokines, IL-2, IL-18, and IFN-γ, were detected with immunohistochemistry. Serum granzyme B and perforin were measured by fow cytometry.
RESULTS: Of the 29 cytokines, the levels of IL-2 and IL-18 were increased signifcantly in liver recipients with GVHD compared with healthy controls (P<0.05). The serum levels of these three cytokines in the healthy, HCC, LT, and RT groups were IL-2: 0.90±0.02, 4.14±0.61, 5.10±0.89, and 1.48 ±0.09 pg/mL; IL-18: 80.61±9.35, 109.51±10.93, 230.11±12.92, and 61.98±7.88 pg/mL; IFN-γ: 24.06±3.88, 24.84±3.21, 40.37±5.88, and 15.33±4.72 pg/mL, respectively. Immunohistochemistry showed that these 3 cytokines expressions in the liver were parallel to the serum cytokine. After standard anti-GVHD treatment, the expressions of IL-2, IL-18, and IFN-γ were decreased in the liver (P<0.05). Serum granzyme B and perforin were signifcantly increased in GVHD patients (P<0.05).
CONCLUSIONS: IL-2, IL-18 and IFN-γ were from liver and might serve as biomarkers for monitoring GVHD development and the effects of anti-GVHD treatment. Granzyme B and perforin may play a role in increasing IL-2, IL-18, and IFN-γ levels in GVHD patients.
(Hepatobiliary Pancreat Dis Int 2017;16:45-51)
cytokines;
graft-versus-host disease;
transplantation;
multiplex immunoassay;
high-throughput
Introduction
Graft-versus-host disease (GVHD) is a medical complication following the receipt of transplanted tissue from a genetically different person. It is the ffth cause of death following liver transplantation. Data from liver transplant registries[1-3]show that China has the largest number of patients with HCC on transplant waiting lists; almost half of all liver transplants are performed in patients with HCC. Previously, we reviewed follow-up data on 6012 Chinese patients with HCC who underwent liver transplantation and found that the major causes of death post-transplantation were hemorrhage, infection, graft failure, multiple organdysfunction syndrome, and GVHD. Of these conditions, GVHD is very challenging for clinicians, as it is diffcult to diagnose due to similarities between the clinical presentations of drug reactions or viral infections, especially cytomegalovirus (CMV) disease.[4]Early non-invasive diagnostic biomarkers for GVHD are urgently needed.
GVHD after orthotopic liver transplantation (OLT) is a severe complication. The incidence is 1%-2% and the mortality rate 85%-90%. Recent studies have found that cytokines modulate both T-helper type 1 (Th1) and Th2 responses. Cytokine storms are evident in patients with GVHD.[5,6]The serum concentrations of many cytokines (e.g., IL-18) are elevated in experimental models of GVHD.[5]However, the cytokine profle of the cytokine storm has not been defned. Most relevant studies have used dedicated sample processing, time-consuming fow cytometry, and complicated data analysis;[7-9]hindering early diagnosis and treatment. In this study, we established a cytokine examination protocol using routine blood samples. We described a high-throughput method that simultaneously measures the levels of multiple cytokines. This is especially valuable for early non-invasive diagnosis of GVHD in patients after transplantation. We also analyzed an HCC cohort that had not undergone transplantation, and healthy controls. We describe serum diagnostic platform for GVHD after organ transplantation; this is not organ-specifc and is not compromised by any underlying disease.
Methods
Patients
We screened the medical records of patients who underwent organ transplantation in our center and included 87 patients for whom long-term follow-up data were available. Forty-fve transplantation patients [23 HCC patients who underwent liver transplantation (the LT group) and 22 patients who underwent renal transplantation (the RT group)] with biopsy-confrmed GVHD were included. HCC patients who had not undergone transplantation (HCC group,n=22) and healthy subjects (healthy control,n=20) served as positive and negative controls, respectively. GVHD was confrmed histologically after physical examination and virus and microbiology screening to exclude differential diseases such as continuing bacterial and fungal infections. Treatment for GVHD: methylprednisolone (0.5 g/d) for 3 days and 2 doses of Zenapax (50 mg).
This study was approved by the Ethics Committee of the First Affliated Hospital, Zhejiang University School of Medicine. Written informed consent for blood sample collection was obtained in advance. All clinical information was retrieved from the Transplant Recipients Database described in previous publications.[11,12]
Cytokine measurements by multiplex immunoassay
Cytokine levels were measured using the Procarta Plex™ Multiplex Immunoassay Kit (Affymetrix; Foster City, CA, USA) as described in the Procarta manual and previous publications.[13-15]In this assay, multianalyteprofling beads are used to detect multiple cytokines employing fuorescent dye technology. The use of two lasers and digital signal processing effectively allows multiplexing of up to 50 unique assays within a single sample. Blood samples were centrifuged at 1000 g at 4 ℃ for 10 minutes, and the sera were stored below -20 ℃ prior to simultaneous one-time cytokine measurements. Twentyfve μL of serum from each patient were incubated with antibodies against human cytokines in 96-well plates. After rinsing, the plates were incubated with multiple antibodies and the reactions detected using a streptavidinphycoerythrin combination; data were quantifed using the Luminex200system (Bio-Rad; Shanghai, China). Quality control featured plotting standard curves plotted using dilutions of the reconstituted antigens; the curves were constructed using Certifcate Analysis Software.
Pathological confrmation andin-situimmunocytochemistry
Pathological slides containing biopsy material collected at the time of the initial diagnosis (GVHD onset) were compared with those containing material collected at the time of the second biopsy (after standard anti-GVHD therapy). Tissues were fxed in 10% (v/v) buffered formalin overnight and embedded in paraffn. Antibodies against IL-2, IL-18, and IFN-γ (Santa Cruz Biotechnology, Santa Cruz, CA, USA) were used for immunohistochemistry. The quality control was samples from patients with infammatory bowel disease, in which IL-2, IL-18, and IFN-γ are expressed at stable levels. Staining was quantifed using Image J software (the Chinese version developed by the National Institutes of Health).
GVHD diagnosis and blood sample collection
After liver or renal transplantation, GVHD generally develops when donor lymphocytes mount an alloreactive response against host histocompatibility antigens. Patients develop fever, rash, diarrhea, and pancytopenia. Blood tests are run and biopsies are performed when GVHD is suspected. Blood samples were collected from patients who developed fever or a rash after liver or renal transplantation; GVHD was confrmed by biopsy.[16]We found that GVHD developed several months posttransplantation. Thus, control blood samples from HCC patients were collected at a similar time after radical surgery, ensuring that surgical intervention in the controls would have the same impact as that in the transplantation groups.
Quantifcation of granzyme B and perforin levels using fow cytometry
We used fow cytometry to measure the levels of monoclonal antibodies binding to granzyme B and perforin (BD Pharmingen, San Jose, CA, USA). Blood samples (100 μL) were added to tubes containing 5 μL of antibody solutions against granzyme B or perforin, mixed in the dark, and incubated at room temperature for 15 minutes. Flow cytometry using a Beckman Coulter platform employed both live and logical gating strategies. Data on a minimum of 10 000 fuorescent dots were analyzed.
Statistical analysis
All data are expressed as means±SD. Comparisons were performed using Student'sttest. APvalue of <0.05 was considered statistically signifcant. One-way ANOVA was used to compare among-group differences. All analyses were performed using SPSS software, version 17.0 (Chicago, IL, USA).
Results
Baseline clinical characteristics
Patients from the four groups were matched in terms of age, gender, and serum storage time. The clinical characteristics of the patients are summarized in Table.
After reviewing medical histories, we found that GVHD manifested not as liver or kidney problems but rather as other-organ features such as rash, fever, or diarrhea. The clinical symptoms are critical in terms of differential diagnosis. We found that GVHD developed after recovery from surgery at 253±39 and 192±51 days postliver and post-renal transplantations, respectively. Accurate diagnoses were made using classical histological and immunohistochemical criteria.[16]
Screening for cytokines
Compared with healthy controls, the levels of IL-2 and IL-18 were signifcantly elevated in liver recipients with GVHD (Fig. 1). The levels of these 3 cytokines in the healthy controls, HCC, LT, and RT groups were IL-2: 0.90±0.02, 4.14±0.61, 5.10±0.89, and 1.48±0.09 pg/mL; IL-18: 80.61±9.35, 109.5 1±10.93, 230.11±12.92,and 61.98±7.88 pg/mL; IFN-γ: 24.06±3.88, 24.84±3.21, 40.37 ±5.88, and 15.33±4.72 pg/mL, respectively. The assay sensitivities ranged from 0.5 pg/mL (IL-2) to 1.22 pg/mL (IL-18).
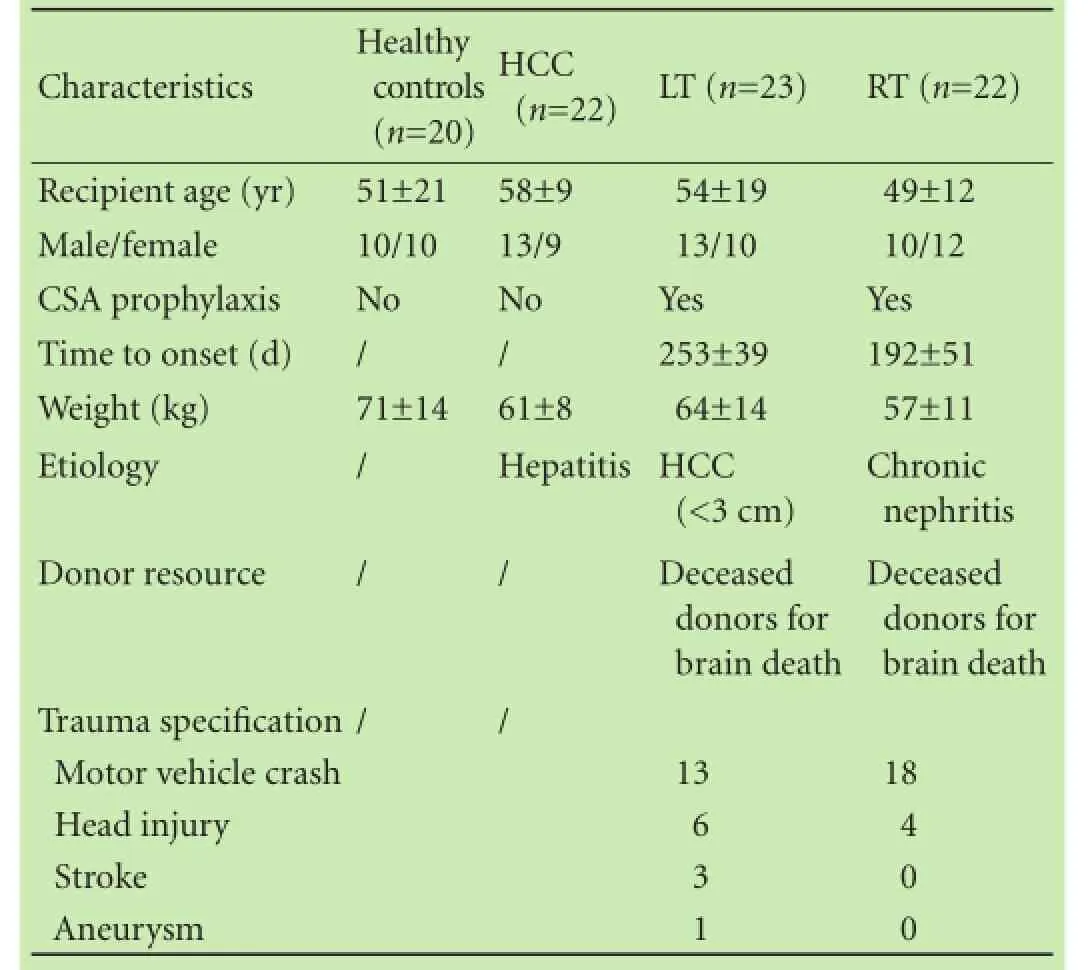
Table. The baseline characteristics of healthy controls and patients in the HCC, LT and RT groups
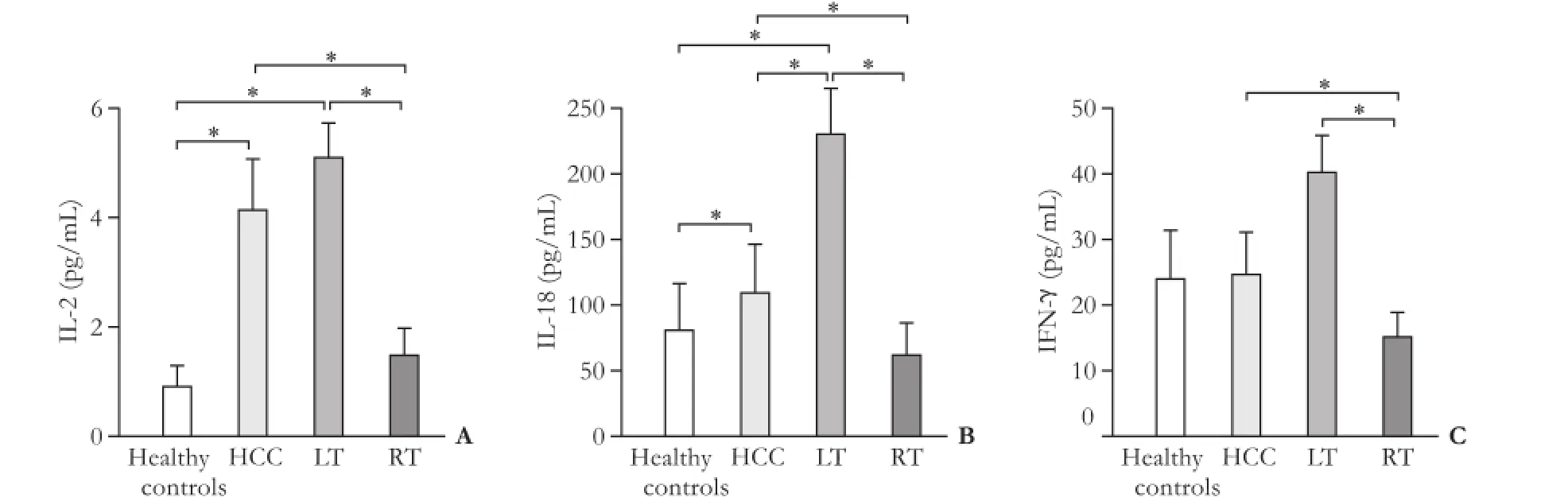
Fig. 1. Serum IL-2 (A), IL-18 (B) and IFN-γ (C) increased signifcantly in liver recipients with GVHD. *:P<0.05, siginifcant difference between pair groups.
IL-2, IL-18, and IFN-γ infltrate the livers of GVHD patients
GVHD was histologically confrmed using routine methods. Hematoxylin and eosin (H&E)-stained slides of liver biopsy material revealed lymphocytic infltration, damage to vessel ducts, portal space congestion, and duct epithelial destruction (Fig. 2). The levels of IL-2, IL-18, and IFN-γ were signifcantly higher in the GVHD onset patients. After standard treatment for GVHD, the quantitative evaluation of IL-2, IL-18, and IFN-γ were decreased signifcantly (P<0.05, Fig. 3).
Granzyme B and perforin levels increased in GVHD patients
In efforts to defne early diagnostic biomarkers predicting GVHD development, granzyme B and perforin levels were determined in peripheral blood CD8 T cells from healthy controls, HCC patients, and GVHD patients receiving liver/renal transplants. Both granzyme B and perforin levels were elevated in GVHD patients compared with healthy controls (fow counts are shown in Fig. 4A, and numerical data from three repeat experiments are shown in Fig. 4B). These suggested that the granzyme B/perforin pathway is involved in GVHD development.

Fig. 3. The quantitative evaluation of IL-2, IL-18 and IFN-γ by using the Luminex200system. After standard treatment of GVHD, the levels of IL-2, IL-18 and IFN-γ decreased signifcantly compared with GVHD onset patients. *:P<0.05.
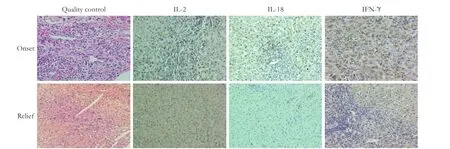
Fig. 2. Immunohistochemistry shows that IL-2, IL-18 and IFN-γ positive cells increased in livers biopsied from GVHD onset patients. GVHD standard treatment signifcantly decreased the number of IL-2, IL-18 and IFN-γ positive cells. Original magnifcation ×40.
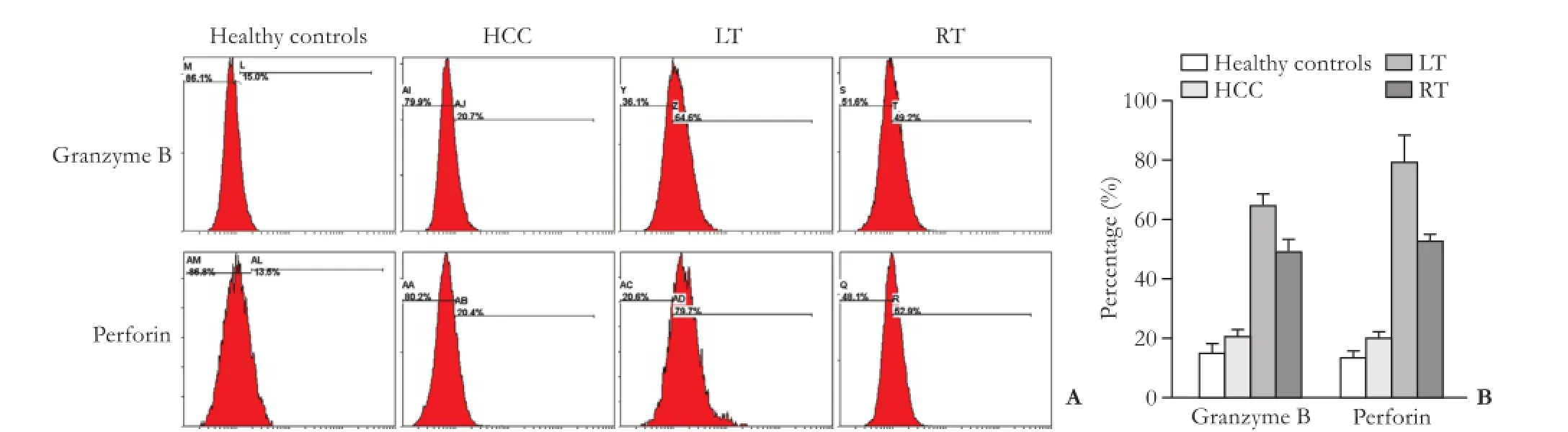
Fig. 4. The expressions of granzyme B and perforin increased in CD8 T cells of GVHD patients. A: fow cytometry; B: the numerical data from 3 dependent repeats.
Discussion
In our liver and renal transplantation practice, the recognization of GVHD is based on specifc clinical and biopsy fndings, rather than onset time. The clinical signs in skin, gastrointestinal tract, and liver are always correlated with pathological features. The routine pathological exam (H&E, Masson trichrome stain and periodic acidschiff) can provide the fundamental proof of the hepatic damage and the involvement of biliary epithelium.
As emphasized above, GVHD diagnosis should be based on characteristic clinical symptoms of the target organ and pathological data on biopsy. In clinical practice, however, the most frequent GVHD symptoms (rash, fever, and diarrhea) are so nonspecifc that it becomes very diffcult to differentiate GVHD from a drug rash, general infection, venous occlusive disease, viral resurrection, or treatment-associated toxicity. Laboratory assays for human leukocyte antigen (HLA), DNA studies, and invasive biopsies require time, specialized equipment, and professional expertise, compromising a timely diagnosis and delaying treatment. It is thus urgent to develop an objective, non-invasive and quantitative method for GVHD diagnosis.
Immune system analyses post-transplantation are effective to this end but are diffcult to perform. Analyses of multiple immune markers are very time-consuming and require many reagents, decreasing the accuracy of parallel comparisons. Here, we offered a solution by identifying cytokine biomarkers of early GVHD and providing reference baseline data. Serum cytokine levels and pathological data afford comprehensive evaluation, making it unnecessary to explore organ specifcity or underlying disease.
Previous studies in mice suggested that IL-18 induces the cytokine storm and is critical in terms of GVHD-induced injury,[5,6]as well as injuries associated with other infammatory diseases.[17-23]Thus, we measured the levels of IL-18 and other cytokines in human patients with GVHD. To optimize the use of small amounts of serum, a multiplex immunoassay was used to measure many cytokines in a single run. This minimizes blood sample requirements (only 25 μL of serum are required), avoids among-group variation, and maximizes quality control.
IL-2 and IL-18 levels were all signifcantly higher in liver recipients with GVHD compared with those in healthy controls (P<0.05). Pathology showed that the cytokines were expressed principally in infammatory cells infltrating the portal space of GVHD patients. After treatment of GVHD, IL-2, IL-18 and IFN-γ levels decreased signifcantly (P<0.05). Our study sheds light on the roles played by IL-2, IL-18, and IFN-γ in the context of liver GVHD.
From an immunological perspective, GVHD is the rejection of the donor organ by host T-cells; cytotoxic T-lymphocytes also play an important role. In addition, the failure of regulatory mechanisms may play a role in GVHD. However, the role played by CD4 is relatively clear: CD4 T-cells exert a benefcial immunosuppressive effect in GVHD patients. Thus, we focused only on CD8. Because granzyme B and perforin mediate rejection, we also measured the levels of these two key proteins. Granzyme B and perforin expression levels were elevated in GVHD patients, supporting the role of T-cell-mediated cytotoxicity in GVHD and explaining the increased cytokine levels.
As the diagnosis of GVHD depends principally on nonspecifc clinical symptoms, prompt identifcation and treatment of GVHD are often delayed. Laboratory biomarkers are crucial for early GVHD identifcation. Currently, biomarker investigations are limited principally to patients receiving blood stem cell transplants. Many clinically relevant biomarkers of biological, pathogenic, or pharmacological responses have been defned.[24]Ideal biomarker for GVHD should be specifc, sensitive to the stage of GVHD, capable of being measured noninvasively, and rapid, simple, accurate, and inexpensive to assay in a standardized manner.[25-29]The same biomarker should be useful for not only early diagnosis but also defning prognostic outcomes.
Our study extends exploratory research on GVHD biomarkers from patients undergoing blood stem cell transplantation to those receiving solid organs. We found that GVHD development in solid organs was associated with elevated levels of the cytokines IL-2, IL-18, and IFN-γ, perhaps predisposing the patient to GVHD. Sampling at a time close to GVHD onset may provide clues as to which biological events initiate GVHD development. Due to the low occurrence, there were few reports comparing cytokines in GVHD post solid organ transplantation. Our current study provides some initial insights in the matter of cytokines with different background and baselines. As shown in Fig. 1, serum IL-2 and IL-18 increased in liver recipients with GVHD compared with healthy controls. We are carrying out further HLA matching degree analysis in larger cohort to investigate the underlying mechanism. Most importantly, an early non-invasive blood test may permit timely therapeutic intervention.
There are some limitations of the study. GVHD has been found most often after allogenic hematopoietic stem cell transplantation and much less frequently after transplantation of immunologically active solid organs such as the liver, kidney, and small intestine.[25-29]We provide frst-hand data on GVHD after solid organ trans-plantation. The formation of appropriate control groups was very challenging. We did not include other parallel baseline controls such as renal transplantation patients lacking GVHD, liver transplantation patients without GVHD, small intestine transplantation patients with/ without GVHD, or hematopoietic stem cell transplantation patients with/without GVHD. Further investigations on reasonable numbers of patients with GVHD of various organs, after careful randomization and matching, are required.
A total of 45 GVHD patients that developed after liver or renal transplantation were evaluated. We focused on baseline rather than time-course data. The fndings require confrmation, and data from other patients treated in other centers are required. In the absence of a cohort differing from our current cohort in terms of baseline cytokine levels, diagnostic performance is diffcult to evaluate. We thus present initial data on baseline cytokine levels. We suggest that a cytokine panel, rather than a single cytokine, should be measured to explore the etiology of GVHD.
In conclusion, IL-2 and IL-18 levels were increased signifcantly in the livers of patients with GVHD,[2]paralleling their increased levels in serum.[3]Such expression was associated with portal space congestion, epithelial cell destruction, and bile duct damage.[4]After anti-GVHD treatment, the liver expression levels decreased signifcantly, suggesting that IL-2, IL-18 and IFN-γ are involved in liver GVHD, likely contributing to tissue damage.
Acknowledgements:The authors thank Dr. Jared Balaich from Princeton University for proof-reading the manuscript.
Contributors:YSY and ZSS conceived and designed the experiments. CXH collected samples. YSY contributed reagents. MXQ and XYN performed the experiments. WLM analyzed the data. MXQ and CXH wrote the manuscript. All authors contributed to the design and interpretation of the study and to further drafts. ZSS is the guarantor.
Funding:The research is supported by grants from the National Natural Science Foundation of China (81372425, 81572954, 81421062, 91542205 and 81401319).
Ethical approval:This retrospective study was approved by the Ethical Committee of the First Affliated Hospital, Zhejiang University School of Medicine.
Competing interest:No benefts in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Center MM, Jemal A, Lortet-Tieulent J, Ward E, Ferlay J, Brawley O, et al. International variation in prostate cancer incidence and mortality rates. Eur Urol 2012;61:1079-1092.
2 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011;61:69-90.
3 Xu X, Lu D, Ling Q, Wei X, Wu J, Zhou L, et al. Liver transplantation for hepatocellular carcinoma beyond the Milan criteria. Gut 2016;65:1035-1041.
4 Chaib E, Silva FD, Figueira ER, Lima FR, Andraus W, D'Albuquerque LA. Graft-versus-host disease after liver transplantation. Clinics (Sao Paulo) 2011;66:1115-1118.
5 Min CK, Maeda Y, Lowler K, Liu C, Clouthier S, Lofthus D, et al. Paradoxical effects of interleukin-18 on the severity of acute graft-versus-host disease mediated by CD4+ and CD8+ T-cell subsets after experimental allogeneic bone marrow transplantation. Blood 2004;104:3393-3399.
6 Reddy P, Teshima T, Kukuruga M, Ordemann R, Liu C, Lowler K, et al. Interleukin-18 regulates acute graft-versus-host disease by enhancing Fas-mediated donor T cell apoptosis. J Exp Med 2001;194:1433-1440.
7 Grönberg H, Adolfsson J, Aly M, Nordström T, Wiklund P, Brandberg Y, et al. Prostate cancer screening in men aged 50-69 years (STHLM3): a prospective population-based diagnostic study. Lancet Oncol 2015;16:1667-1676.
8 Lombard C, André F, Paul J, Wanty C, Vosters O, Bernard P, et al. Clinical Parameters vs cytokine profles as predictive markers of IgE-mediated allergy in young children. PLoS One 2015;10:e0132753.
9 Ott LE, Carson S. Immunological tools: engaging students in the use and analysis of fow cytometry and enzyme-linked immunosorbent assay (ELISA). Biochem Mol Biol Educ 2014;42: 382-397.
10 Peng W, Liu G, Xie W, Huang H, Wu J, Shou Z, et al. Interleukin-2 receptor antagonist compared with antithymocyte globulin induction therapy in kidney transplantation from donors after cardiac death. Int J Clin Pract Suppl. 2015;(183):23-28.
11 Zhou J, Hu Z, Zhang Q, Li Z, Xiang J, Yan S, et al. Spectrum of de novo cancers and predictors in liver transplantation: analysis of the scientifc registry of transplant recipients database. PLoS One 2016;11:e0155179.
12 Wei Q, Xu X, Wang C, Zhuang R, Zhuang L, Zhou L, et al. Effcacy and safety of a steroid-free immunosuppressive regimen after liver transplantation for hepatocellular carcinoma. Gut Liver 2016;10:604-610.
13 Staples E, Ingram RJ, Atherton JC, Robinson K. Optimising the quantifcation of cytokines present at low concentrations in small human mucosal tissue samples using Luminex assays. J Immunol Methods 2013;394:1-9.
14 Pranzatelli MR, Tate ED, McGee NR, Colliver JA. Pediatric reference ranges for proinfammatory and anti-infammatory cytokines in cerebrospinal fuid and serum by multiplexed immunoassay. J Interferon Cytokine Res 2013;33:523-528.
15 de Koning L, Liptak C, Shkreta A, Bradwin G, Hu FB, Pradhan AD, et al. A multiplex immunoassay gives different results than singleplex immunoassays which may bias epidemiologic associations. Clin Biochem 2012;45:848-851.
16 Murali AR, Chandra S, Stewart Z, Blazar BR, Farooq U, Ince MN, et al. Graft versus host disease after liver transplantation in adults: a case series, review of literature, and an approach to management. Transplantation 2016 Aug 3.
17 Inoue T, Aoyama-Ishikawa M, Kamoshida S, Nishino S, Sasano M, Oka N, et al. Endogenous interleukin 18 regulates testicular germ cell apoptosis during endotoxemia. Reproduction 2015;150:105-114.
18 Jung SS, Moon JS, Xu JF, Ifedigbo E, Ryter SW, Choi AM, etal. Carbon monoxide negatively regulates NLRP3 infammasome activation in macrophages. Am J Physiol Lung Cell Mol Physiol 2015;308:L1058-1067.
19 Choudhry MA, Li X, Chaudry IH. A role for corticosterone in impaired intestinal immunity and barrier function in a rodent model of acute alcohol intoxication and burn injury. J Neuroimmune Pharmacol 2006;1:428-434.
20 Li X, Rana SN, Schwacha MG, Chaudry IH, Choudhry MA. A novel role for IL-18 in corticosterone-mediated intestinal damage in a two-hit rodent model of alcohol intoxication and injury. J Leukoc Biol 2006;80:367-375.
21 O'Brien LC, Mezzaroma E, Van Tassell BW, Marchetti C, Carbone S, Abbate A, et al. Interleukin-18 as a therapeutic target in acute myocardial infarction and heart failure. Mol Med 2014;20:221-229.
22 Paczesny S. Discovery and validation of graft-versus-host disease biomarkers. Blood 2013;121:585-594.
23 Macgregor JN, Li Q, Chang AE, Braun TM, Hughes DP, Mc-Donagh KT. Ex vivo culture with interleukin (IL)-12 improves CD8(+) T-cell adoptive immunotherapy for murine leukemia independent of IL-18 or IFN-gamma but requires perforin. Cancer Res 2006;66:4913-4921.
24 Gatza E, Braun T, Levine JE, Ferrara JL, Zhao S, Wang T, et al. Etanercept plus topical corticosteroids as initial therapy for grade one acute graft-versus-host disease after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant 2014;20:1426-1434.
25 Chang L, Frame D, Braun T, Gatza E, Hanauer DA, Zhao S, et al. Engraftment syndrome after allogeneic hematopoietic cell transplantation predicts poor outcomes. Biol Blood Marrow Transplant 2014;20:1407-1417.
26 Kitko CL, Levine JE, Storer BE, Chai X, Fox DA, Braun TM, et al. Plasma CXCL9 elevations correlate with chronic GVHD diagnosis. Blood 2014;123:786-793.
27 Choi SW, Braun T, Chang L, Ferrara JL, Pawarode A, Magenau JM, et al. Vorinostat plus tacrolimus and mycophenolate to prevent graft-versus-host disease after related-donor reducedintensity conditioning allogeneic haemopoietic stem-cell transplantation: a phase 1/2 trial. Lancet Oncol 2014;15:87-95.
28 Vander Lugt MT, Braun TM, Hanash S, Ritz J, Ho VT, Antin JH, et al. ST2 as a marker for risk of therapy-resistant graftversus-host disease and death. N Engl J Med 2013;369:529-539.
29 Choi SW, Stiff P, Cooke K, Ferrara JL, Braun T, Kitko C, et al. TNF-inhibition with etanercept for graft-versus-host disease prevention in high-risk HCT: lower TNFR1 levels correlate with better outcomes. Biol Blood Marrow Transplant 2012;18:1525-1532.
Received June 12, 2016
Accepted after revision September 30, 2016
Author Affliations: Key Laboratory of Combined Multi-organ Transplantation, Ministry of Public Health, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, the First Affliated Hospital, Zhejiang University School of Medicine, 79 Qingchun Road, Hangzhou 310003, China (Meng XQ, Chen XH, Sahebally Z, Xu YN, Yin SY, Wu LM and Zheng SS)
Shu-Sen Zheng, MD, PhD, FACS, Key Laboratory of Combined Multi-organ Transplantation, Ministry of Public Health, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, the First Affliated Hospital, Zhejiang University School of Medicine, 79 Qingchun Road, Hangzhou 310003, China (Tel: +86-571-87236570; Fax: +86-571-87236466; Email: shusenzheng@zju. edu.cn)
© 2017, Hepatobiliary Pancreat Dis Int. All rights reserved.
10.1016/S1499-3872(16)60157-1
Published online December 28, 2016.
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Instructions for Authors
- The consensus on liver autotransplantation from an international panel of experts
- Associating liver partition and portal vein ligation for staged hepatectomy: the current role and development
- Right hepatectomy in living donors with previous abdominal surgery
- Diagnosis and outcomes of collateral arterial formation after irreversible early hepatic artery thrombosis in pediatric liver recipients
- Resection of T4 hepatocellular carcinomas with adjacent structures, is it justifed?