不同ADP受体拮抗剂对冠心病血小板功能疗效差异的网状Meta分析
2016-12-14于利平
于利平
不同ADP受体拮抗剂对冠心病血小板功能疗效差异的网状Meta分析
于利平
目的 用贝叶斯网状模型比较ADP (Adenosine diphosphate)受体拮抗药clopidogrel、prasugrel、ticagrelor、clopidogrel+others、prasugrele及其他药物(Atorvastatin、lansoprazol)治疗冠心病患者时对血小板功能的作用差异。方法 运用贝叶斯网状模型拟合直接和间接证据分析ADP受体拮抗药对PRU、IPA、PRI影响的差异,并评估各指标的累积排序概率。结果 共纳入10篇文献。结果显示,给药后(6±2)h,clopidogrel、prasugrel、ticagrelor的PRU低于placebo;prasugrel、ticagrelor的PRU值低于clopidogrel。给药2、4、(9±3)h后,prasugrel和Ticagrelor的IPA高于placebo。给药2 h后,prasugrel和ticagrelor的PRI低于placebo与clopidogrel;给药24 h后,ticagrelor的PRI较placebo和clopidogrel降低。结论 ADP受体拮抗药clopidogrel、prasugrel、ticagrelor均有抑制血小板功能的作用,且prasugrel、ticagrelor的抑制效果优于clopidogrel,prasugrel优于ticagrelor。
ADP受体拮抗剂;冠心病;贝叶斯网状模型;血小板功能;随机对照试验
0 引言
冠心病(Coronary artery disease,CAD)是由于冠状动脉血管发生粥样硬化病变,引起血管腔狭窄或阻塞,导致心肌缺血、缺氧或坏死而引起的心脏疾病[1]。CAD是当今世界威胁人类健康的重要疾病之一,我国心血管病的发病和病死率呈现逐年递增的趋势,每年约有350万人死于心血管病,居各疾病致死原因之首[2-3]。心血管疾病重要的病理基础是血栓的形成与发展,其在冠心病患者病情的进展与急性发作过程中,起着非常重要的作用,常导致心肌梗死甚至死亡等严重后果[4]。随着对动脉粥样硬化认识的不断深入,发现血小板在冠心病和急性冠状动脉综合征的发生发展中起关键性作用,其可以与损伤血管处的黏连蛋白结合,并使之活化、变形、聚集,启动血栓的形成[5]。因此,抗血小板治疗是防治冠心病的重点之一。
抗血小板药物可以通过阻断血小板的黏附、活化、变形、聚集,从而减少心血管事件的发生,对治疗冠心病具有重要作用[6]。常用的抗血小板药物有二磷酸腺苷(Adenosine diphosphate,ADP)受体拮抗剂、磷酯酶抑制剂(PDE)、环氧化酶抑制剂等[7]。ADP在血小板活化过程中,可以激活血小板膜糖蛋白Ⅱb/Ⅲa受体,介导血小板与纤维蛋白原的结合,因此,在血小板的整个活化过程中,ADP起重要作用[8]。ADP受体拮抗剂包括氯吡格雷(Clopidogrel)、普拉格雷(Prasugrel)和替格瑞洛(Ticagrelor)等。其中,Clopidogrel和Prasugrel为噻吩并吡啶类ADP受体拮抗剂,需经过生物肝细胞酶代谢成为活性药物,并且其与ADP受体的结合具有不可逆性[9]。Clopidogrel可降低心肌梗死及脑卒中发生率[10],但其发挥最大抑制效果至少要在服药6 h后[11];Prasugrel抗血小板聚集作用优于氯吡格雷,主要表现在其起效快,非应答率低,个体差异小[12]。而Ticagrelor是一类环戊基三唑嘧啶,为非噻吩并吡啶类ADP受体拮抗剂,与ADP受体的结合具有可逆性,且具有起效快、作用时间短的特点[13]。然而,目前没有关于Clopidogrel、Prasugrel和Ticagrelor直接对比的临床数据。
网状Meta分析作为一种新的临床证据生产方法,可以清晰地呈现各干预措施间存在的直接比较和间接比较,进而选择最优治疗方案[14]。本研究通过贝叶斯网状模型,比较ADP受体拮抗药Clopidogrel、Prasugrel、Ticagrelor、Clopidogrel+其他、Prasugrel+其他(其他包括Atorvastatin、Lansoprazol)治疗冠心病患者时对血小板功能的作用差异,为合理选择治疗CAD提供证据支持。
1 资料与方法
1.1 检索策略 计算机检索PubMed数据库,采用关键词和自由词相结合的原则制定严格的检索策略,检索关键词:Coronary artery disease(CAD)、Randomized controlled trial、Purinergic P2Y receptor antagonists、Clopidogrel、Prasugrel等,检索年限范围从建库起至2015年12月。
1.2 纳入与排除标准 纳入标准:①数据完整的随机临床对照试验;②研究人群均为冠心病患者;③研究分组为2组及以上,且必有一组为ADP受体拮抗药物如Clopidogrel、Prasugrel、Ticagrelor、Ticlopidine及Cangrelor等;④存在血小板功能评估的结局指标,如PRU (Plate reactivity units)、IPA(Inhibition of platelet aggregation)、PRI (Platelet reactivity index)。排除标准:①重复发表试验;②非人类研究文献;③非英语语言描述文献;④会议报道、系统评价、摘要及病例报告类文献;⑤出血性疾病史人群;⑥30 d内发生ACS或外周动脉血管闭塞人群;⑦30 d内用质子泵抑制剂或PCI进行过治疗人群;⑧有严重的肾部损伤或者近期有手术史人群。
1.3 数据提取与质量评价 采用统一制定的数据收集表,由两位研究者分别独立提取纳入文献数据资料,数据提取过程中若出现争议,则通过与多个研究人员讨论协商直至达成共识。由2个以上的研究者根据Cochrane风险偏倚评估工具[15]评价随机对照试验,该工具包括6个变量,即随机分配、分配隐藏、盲法、丢失结局数据、选择结局报告及其他偏倚。上述变量中分别有“是”、“否”、“不清楚”3个选项,分别表示偏倚的低风险、高风险和未知风险。据量表结果,1个以内“不”或“不清楚”选项的视为低度偏倚,2~3个“不”或“不清楚”选项的视为中度偏倚,4个及以上“不”或“不清楚”选项的视为高度偏倚[16]。使用Review Manager 5 (RevMan5.2.3,Cochrane Collaboration,Oxford,UK)对偏倚进行定量分析。
1.4 统计学方法 首先,采用固定效应模型或随机效应模型对纳入文献不同药物的结局指标进行直接比较,使用卡方检验或者I2来判断纳入文献是否存在异质性[17]。其次,利用贝叶斯网状模型绘制各个结局指标的网状关系图,后者显示每类结局指标下干预措施的基本信息,以每个节点表示一种干预药物,节点大小表示该干预药物的样本量,节点之间的连线表示该对干预措施下纳入研究数量的多少。然后,对纳入研究中的干预药物进行直接证据或间接证据比较,由于本文的结局指标为连续性变量,所以,比较结果以加权均值差(Weighted mean difference,WMD)表示。通过节点切割法评价各药物间直接证据比较和间接证据比较是否一致,以P>0.05判断为一致,结果选择一致性模型[18];同时根据贝叶斯网状模型下得到的干预药物的累积排序概率,绘制相应药物的累积排序概率曲线,并根据曲线下面积,来判断疗效最佳的药物,曲线下面积越大表示疗效越好[19]。所有的统计分析均使用R (V3.1.2) 软件,于R软件中调用gemtc和JAGS packages 完成贝叶斯网状模型的分析。
2 结果
2.1 纳入研究的基线特征 本研究共检索到相关文献814篇,剔除非英语文献45篇,非人类研究26篇,无法获得全文45篇,会议报道、系统评价、摘要及病例报告类文献122篇;对剩余的576篇通过摘要初步评估,不符合文献纳入标准者556篇,予以剔除,有120篇是非干预药物研究,149篇非冠心病研究,有295篇的研究指标与血小板功能无关;对剩余12篇进行基线信息(包括人群基本特征、干预药物、结局指标)提取后,由于数据信息不完整而剔除2篇文献,最终有10篇文献符合标准纳入本次研究[20-29]。10篇纳入文献的发表时间为2006-2014年,以2014年较多;共包括1 540例CAD患者,男1 123例,女377例;有9项研究的人群来源于欧美人群,1项研究人群来源于亚洲人群;纳入的文献中共有8项是双臂试验,分别有1项3臂和1项4臂试验;纳入研究的基线特征见表1。Cochrane文献质量评价见图1。
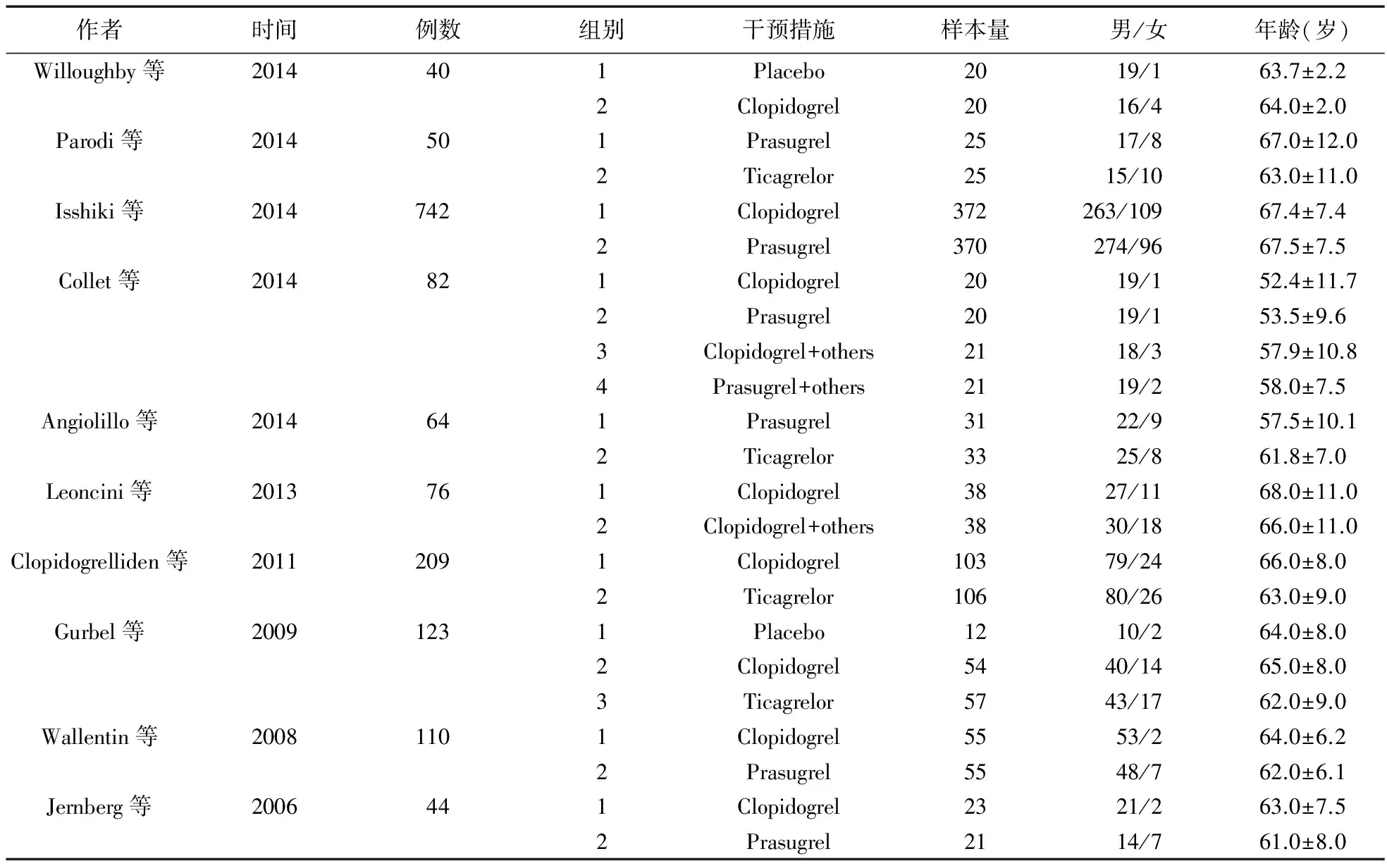
表1 纳入文献基线特征
注:Others包括Atorvastatin、lansoprazole

图1 Cochrane质量评价图
2.2 Pairwise meta-analysis 本文对7种药物治疗冠心病后的血小板功能进行直接配对比较,以PRU、IPA、PRI为结局指标。给药(6±2)h后,Clopidogrel和Ticagrelor的PRU均低于Placebo (WMD=-155.08,95%CI=-178.91~-131.25;WMD=-291.09,95%CI=-314.12~-268.06),Clopidogrel的PRU低于Prasugrel和Ticagrelor (WMD=-154.01,95%CI=-170.10~-137.92;WMD=-156.16,95%CI=-193.67~-118.64),而Prasugrel和Ticagrelor的PRU无显著差异;给药(10±4)d后,Prasugrel的PRU高于Ticagrelor(WMD=47.70,95%CI=26.80~68.60),Clopidogrel的PRU高于Prasugrel+others(WMD=66.00,95%CI=35.00~97.00),Clopidogrel+others的PRU高于Prasugrel+others(WMD=87.00,95%CI=55.44~118.56),而Prasugrel的PRU低于Clopidogrel+others(WMD=-63.00,95%CI=-109.44~-16.56);其余药物之间的直接证据比较差异无统计学意义。
给药2、4、(9±3)h后,Placebo的IPA值低于Clopidogrel、Ticagrelor (WMD=-51.39,95%CI=-62.67~-40.11;WMD=-80.30,95%CI=-89.87~-70.73;WMD=-53.53,95%CI=-63.76 ~-43.30;WMD=-80.43,95%CI=-89.03~-71.83;WMD=-56.53,95%CI=-67.15~-45.91;WMD=-78.80,95%CI=-90.48~-62.17);Clopidogrel的IPA值低于Prasugrel和Ticagrelor(WMD=-34.20,95%CI=-53.23~-15.17;WMD=-28.91,95%CI=-39.15~-18.67;WMD=-38.40,95%CI=-56.47~-20.33;WMD=-26.90,95%CI=-37.39~-16.41;WMD=-38.50,95%CI=-56.77~-20.23;WMD=-78.80,95%CI=-90.48~-62.17);而Prasugrel和Ticagrelor的IPA差异无统计学意义。
给药2、24 h后,Clopidogrel和Ticagrelor的PRI值低于Placebo(WMD=-16.55,95%CI=-22.17~-10.93;WMD=-67.56,95%CI=-73.18~-61.94;WMD=-27.74,95%CI=-31.24~-21.2;WMD=-43.63,95%CI=-53.80~-33.46);Clopidogrel的PRI高于Prasugrel和Ticagrelor(WMD=47.58,95%CI=37.95~57.21;WMD=50.86,95%CI=46.59~55.12;WMD=41.52,95%CI=31.98~51.0;WMD=29.99,95%CI=2.91~57.07)。给药2 h后,Prasugrel和Ticagrelor的PRI无显著差异,但给药24 h后,Prasugrel的PRI较Ticagrelor显著增加(WMD=14.10,95%CI=7.16~21.04);给药(14±4)d后,Clopidogrel的PRI较Prasugrel、Prasugrel+others增加(WMD=20.85,95%CI=8.62~33.07;WMD=12.60,95%CI=1.00~24.20),Prasugrel与Clopidogrel+others相比,PRI显著降低(WMD=-13.00,95%CI=-23.12~-2.88);Clopidogrel+others和Prasugrel+others相比,PRI显著增加(WMD=12.30,95%CI=4.30~20.30);其余药物之间的直接证据比较差异无统计学意义。
2.3 证据网络 本文纳入研究分析的药物以ADP受体拮抗剂为主,分别为Placebo、Clopidogrel、Prasugrel、Ticagrelor、Clopidogrel+others、Prasugrel+others(Others包括Atorvastatin、Lansoprazol)。就PRU而言,用Clopidogrel、Prasugrel、Ticagrelor的例数较多,其中以使用Clopidogrel的例数最多,而Placebo和Prasugrel+others的用药例数最少,用药(6±2)h后的PRU指标中,直接比较Clopidogrel和Prasugrel、Prasugrel和Clopidogrel的研究最多;用药(10±4)d后,以Clopidogre与Placebo、Ticagrelor、Clopidogre+others的研究最多见(图2A)。针对IPA,虽然研究的时间点有差别,但纳入研究的文献一致,用Clopidogrel、Ticagrelor的患者例数最多,其次是Prasugrel,且药物之间两两比较研究数无显著差异(见图2C~图2E)。就PRI而言,以服用Clopidogrel、Ticagrelor的例数最多,Prasugrel其次,且药物间直接比较以Clopidogrel和Ticagrelor、Clopidogrel和Prasugrel[给药(14±4)d]的研究数最多(见图2F~图2H)。
2.4 不一致性检验 用节点切割法分析PRU、IPA、PRI直接证据比较和间接证据比较的一致性,结果见表2,可见除(10±4)d PRU指标的Ticagrelor与Placebo节点外,其余一致性检验均显示P>0.05,因此,网状分析采用一致性模型,而(10±4)d PRU指标的Ticagrelor与Placebo结果采用不一致性模型分析(P=0.049)。
2.5 网状Meta分析主要结果 如图3和表3所示,贝叶斯网状模型的分析结果显示,给药后(6±2) h,Clopidogrel、Prasugrel、Ticagrelor的PRU低于Placebo(WMD=-145.94,95%CI=-268.82~-24.89;WMD=-303.54,95%CI=-451.69~-169.01;WMD=-300.16,95%CI=-417.76~-175.51;)Prasugrel、Ticagrelor的PRU值低于Clopidogrel(WMD=-157.69,95%CI=-257.84~-67.28;WMD=-154.36,95%CI=-230.26~-68.24)。
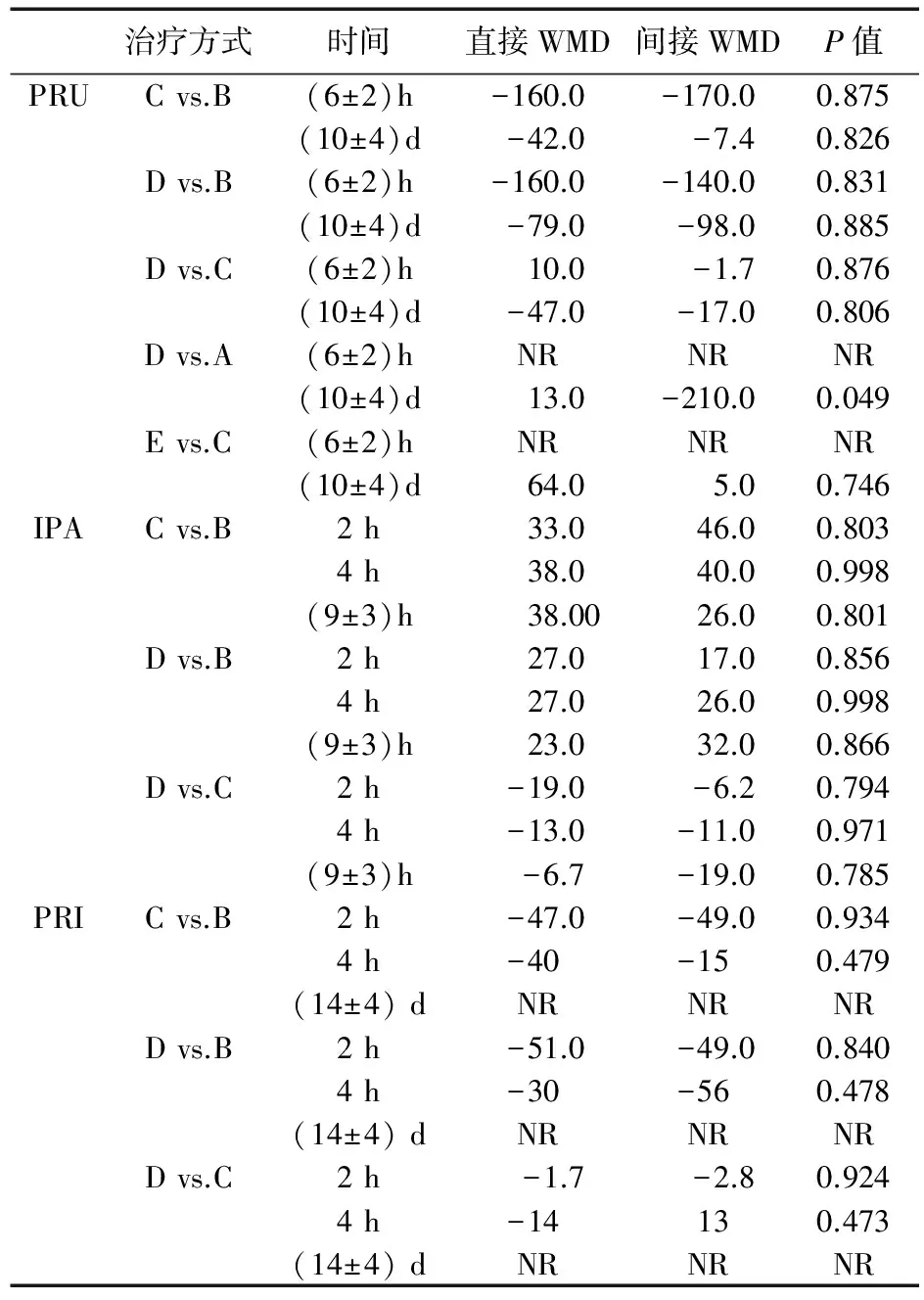
表2 六种治疗手段下PRU、IPA、PRI指标的直接和间接比较
注:A=Placebo,B=Clopidogrel,C=Prasugrel,D=Ticagrelor,E=Clopidogrel+others,F=Prasugrel+others
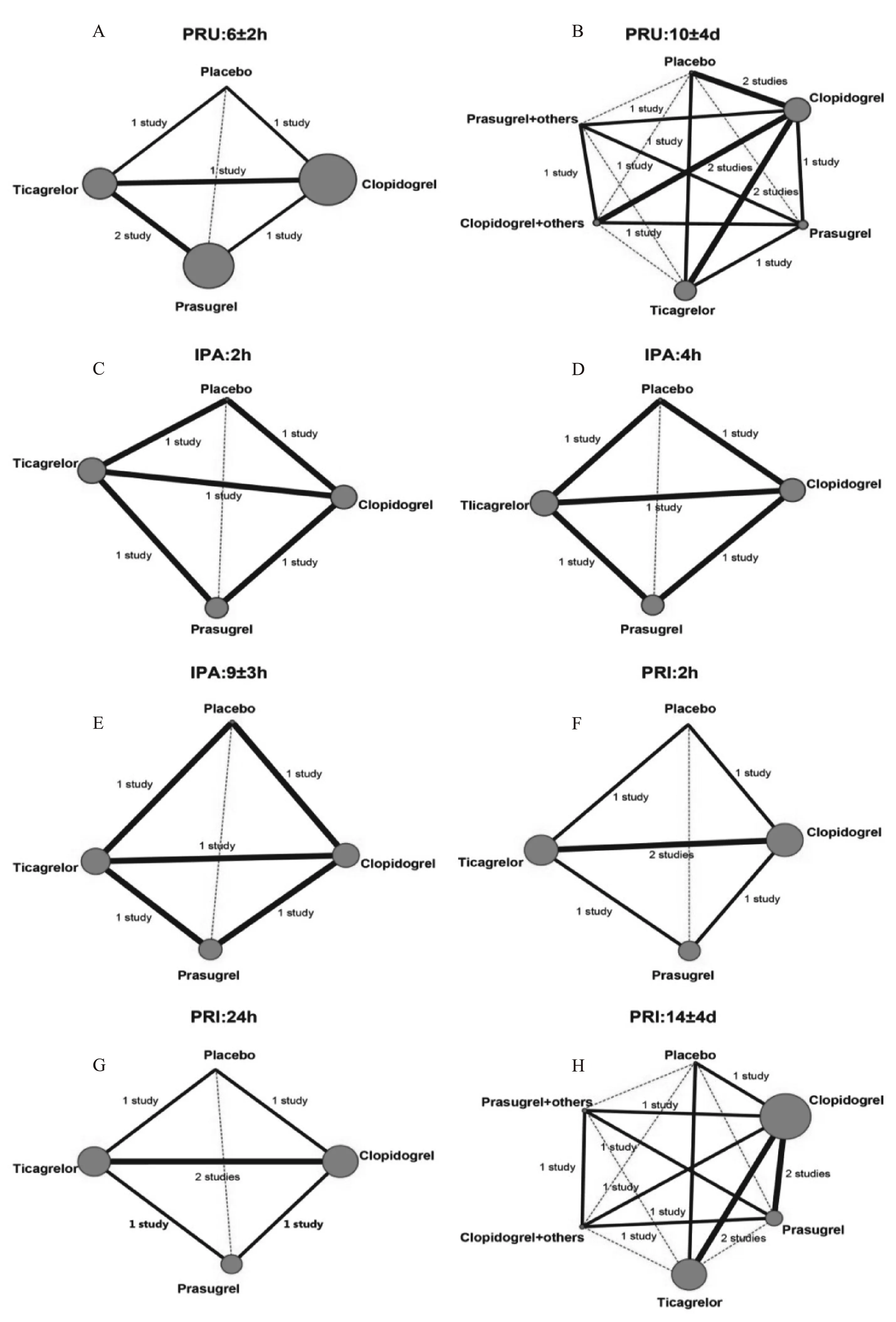
图2 PRU、IPA、PRI的网状关系图
给药2、4、(9±3)h后,Prasugrel、Ticagrelor的IPA高于Placebo(WMD=91.33,95%CI=1.71~179.89;WMD=79.27,95%CI=3.21~152.72;WMD=93.27,95%CI=10.30~177.99;WMD=80.19,95%CI=8.91~152.20;WMD=89.05,95%CI=4.58~174.48:WMD=80.16,95%CI=4.93~152.91)。
给药2 h后,Prasugrel、Ticagrelor的PRI低于Placebo(WMD=-65.40,95%CI=-92.21 ~-38.95;WMD=-67.28,95%CI=-89.45~-45.28)、Clopidogrel (WMD=-48.75,95%CI=-67.36~-29.79;WMD=-50.74,95%CI=-65.42~-35.19);给药24 h后,Ticagrelor较Placebo和Clopidogrel降低(WMD=-53.49,95%CI=-102.11~-2.09;WMD=-35.25,95%CI=-69.22~-0.73),其余药物在PRU、IPA和PRI指标上的两两比较无显著性差异,具体结果见表4。通过网状Meta分析发现,Clopidogrel、Prasugrel、Ticagrelor均有抑制血小板功能的作用,但Prasugrel和Ticagrelor的抑制功能优于Clopidogrel。
2.6 累积排序概率 PRU指标的累积排序概率曲线图(图4A、图4B)显示,给药(6±2)h后,Prasugrel和Ticagrelor的累积排序概率较高,分别为87.75%、85.50%;给药(10±4)d后,Ticagrelor和Prasugrel+others的累积排序概率最高,分别为80.00%、76.00%;IPA指标给药后2、4、(9±3)h累积排序概率均以Prasugrel最高,分别为91.50%、92.75%、91.00%,见图4C、图4E;PRI指标的累积排序概率显示,给药2、24 h后,以Ticagrelor的累积概率最高,分别为91.75%、88.75%,而给药(14±4)d后,累积排序概率以Prasugrel最高,为76.67%,见图4F、图4H。
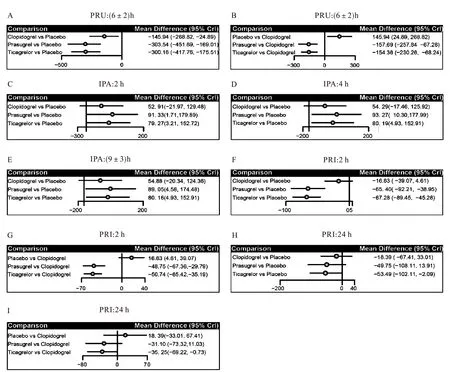
图3 PRU、IPA、PRI的相对关系森林图
3 讨论
本研究采用贝叶斯网状模型比较ADP受体拮抗药治疗冠心病患者时对血小板功能的作用差异,根据相对关系直接证据和间接证据比较结果显示,Clopidogrel、Prasugrel、Ticagrelor均有抑制血小板功能的作用,但Prasugrel和Ticagrelor抑制功能优于Clopidogrel,而两者中又以Prasugrel的抑制作用略好。
Clopidogrel是通过ADP受体P2Y12抑制ADP介导的糖蛋白Ⅱb/Ⅲa复合物的活化,从而达到减弱低剂量ADP所诱导的血小板微聚集和减少剪切力所诱导的血小板微聚集的效果[8]。Parodi等[30]研究发现,Clopidogrel具有抑制血小板聚集的作用,但是存在个体抵抗现象,即使通过改变氯吡格雷抵抗患者的治疗方案,仍有38%的患者存在氯吡格雷抵抗现象。Ticagrelor是一种可逆地直接阻断血小板P2Y12受体的新型口服抗血小板药物,具有抑制血小板聚集、降低急性冠脉综合征患者的心源性病死率,心肌梗死发生率的作用[31]。Gurbel等[32]研究显示,对Clopidogrel有抵抗现象的患者,改用Ticagrelor后,血小板聚集率显著下降;同时,Ticagrelor在Clopidogrel非抵抗组、抵抗组中抗血小板的作用几乎相同,表明Ticagrelor具有更强的抑制血小板凝聚的作用。而Prasugrel具有很高的生物利用度,可迅速抑制血小板活性,且较Clopidogrel具有激活更快速、有效,不受CYP2C19抑制剂和基因多态性影响的优点[11]。陈燕春等[33]研究发现,在治疗急性冠脉综合征时,Prasugrel比Clopidogrel具有更强的抗血小板作用,且不增加出血风险。Biondi等[34]观察急性冠状动脉综合征患者使用Ticagrelor、Prasugrel的有效性与安全性,结果显示,Ticagrelor与Prasugrel具有相似的疗效,但Prasugrel的血栓发生率低于Ticagrelor。上述研究与本文结果相似。
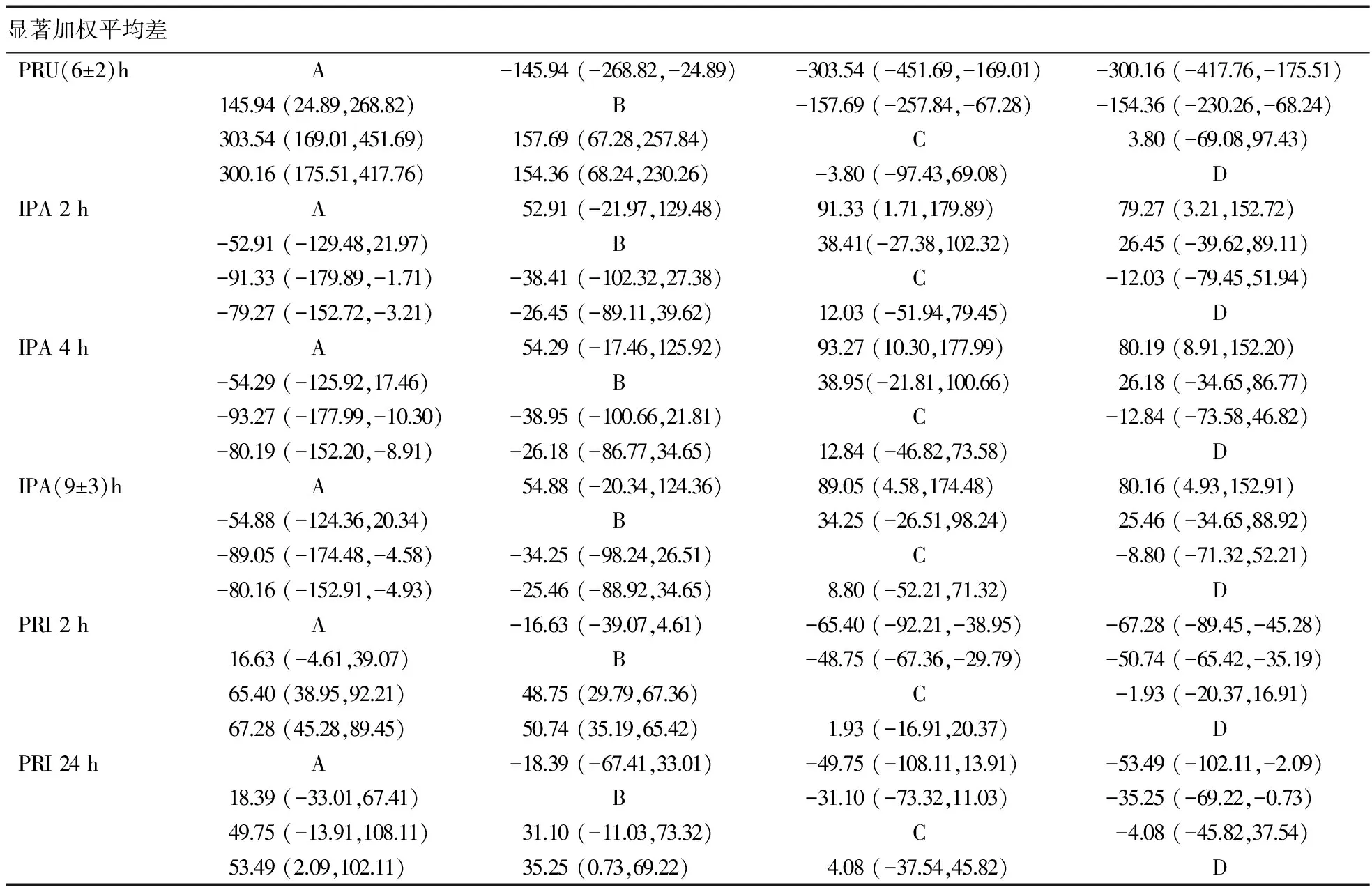
表3 不同治疗手段在PRU、IPA、PRI指标中的网状Meta分析比较
注:A=Placebo,B=Clopidogrel,C=Prasugrel,D=Ticagrelor
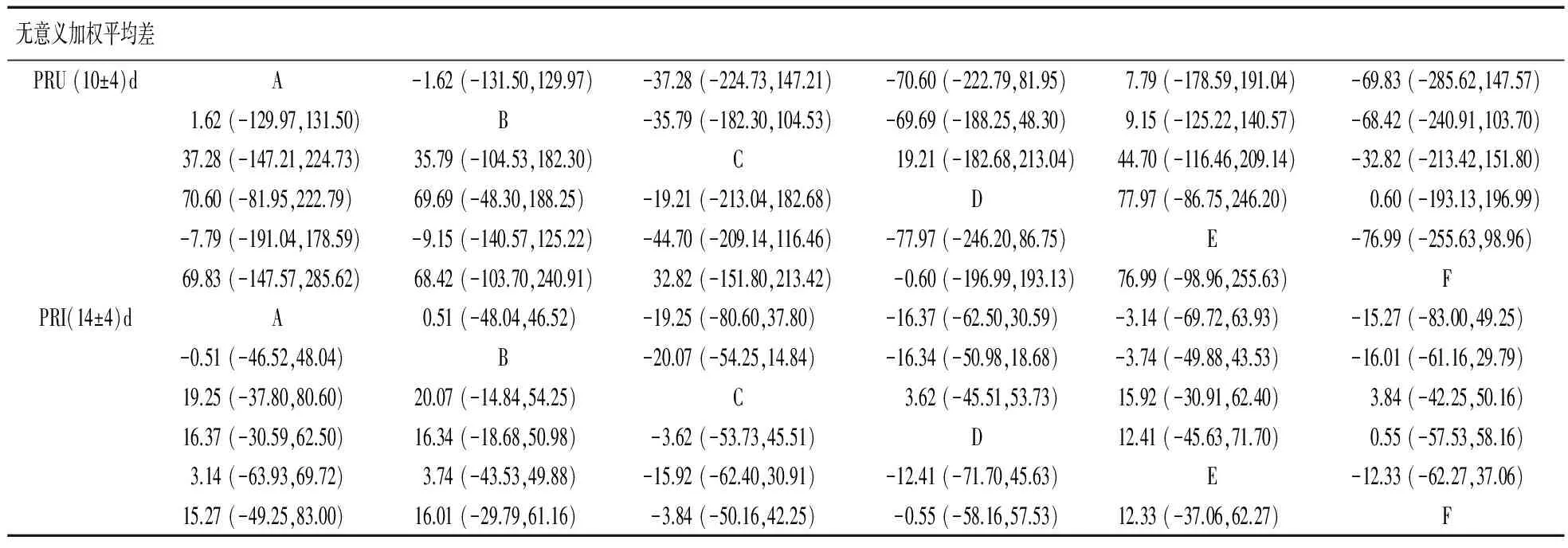
表4 网状Meta分析比较不同治疗方式PRU、IPA、PRI指标结果
注:A=Placebo,B=B,C=Prasugrel,D=Ticagrelor,E=Clopidogrel+others,F=Prasugrel+others
本研究显示,除(10±4)d PRU指标的Ticagrelor与Placebo节点存在显著不一致性,其余结果均具有一致性,表明该研究的结果具有可靠性。TRIGGER-PCI试验[35]通过研究患者PCI术后仍有血小板高反应性(PRU>208)的稳定性冠心病患者,结果表明,治疗3、6个月时,Prasugrel组高PRU患者比例均低于Clopidogrel组,说明使用Prasugrel较Clopidogrel具有更好的治疗效果。杨晓伟等[36]研究表明,Ticagrelor组术后24 h PRU水平低于Clopidogrel,说明Ticagrelor对抗血小板的聚集作用较Clopidogrel增强。关于IPA指标的研究显示,在30 min内,Prasugrel对20 μmol/L ADP诱导的IPA超过20%,而Clopidogrel需1.5 h才能达到此水平[6]。ONSET/OFFSET研究表明,服用负荷剂量Ticagrelor 0.5、1、2、4、8、24 h以及维持用药6周后的IPA均高于Clopidogrel组;服用负荷剂量2 h后,Ticagrelor组IPA>50%的患者占98%,而Clopidogrel组仅31%的患者达到此抑制效应[37]。上述研究与本文结果一致,表明Prasugrel和Ticagrelor对血小板的抑制效果优于Clopidogrel。
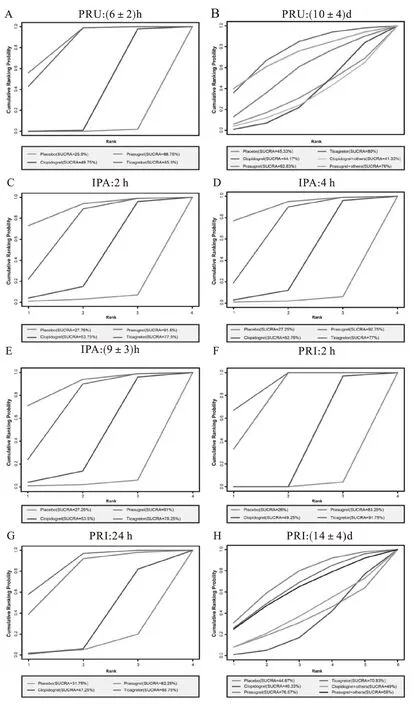
图4 PRU、IPA、PRI的累积排序概率图
网状Meta分析需同时比较多个干预措施的效果,与传统的Meta分析比较,其纳入了更多的原始研究,加上证据网络图的复杂性,使得网状Meta分析证据网络中的不同比较组的统计效能和精确性通常存在差异,但这并不影响网状分析结果的准确性[38-40]。同时,本研究通过干预药物的累积排序概率,来判断疗效最佳的药物。累积排序概率图与累积排序概率图下面积可帮助研究者在比较多种干预措施后,获知最优干预[41]。但因本研究纳入的相关文献量、研究药物及血小板评价指标较少,且本文仅考虑到药物对血小板功能的作用,并未考虑到血小板降低的同时导致不良事件的影响,因而虽然在临床上有一定的指导意义,仍需进一步分析以得出比较全面可靠的结论。如本研究中,传统Meta分析显示,Clopidogrel的PRU、PRI高于Prasugrel+others,Clopidogrel+others的PRU、PRI比Prasugrel明显增加,Clopidogrel+others的PRU、PRI高于Prasugrel+others;但是在网状Meta分析中并未出现该结果,这主要是因为在本研究中纳入文献量、直接配对文献数量和研究药物的样本量较少。
本研究相关贝叶斯网状模型分析结果提示,Prasugrel和Ticagrelor对血小板的抑制效果优于Clopidogrel,而两者中又以Prasugrel的抑制作用较好,对冠心病患者接受治疗具有一定的指导治疗意义。
[1]马琴,牛凡.血浆纤维蛋白原与冠状动脉粥样硬化性心脏病[J].中国实用医药,2010,5(4):255-256.
[2]生部心血管病防治研究中心.中国心血管病报告2012[M].北京:中国大百科全书出版社,2013:13-16.
[3]陈灏珠.实用内科学[M].第14版.北京:人民卫生出版社,2013:1467-1478.
[4]韩雅玲.中国冠心病抗栓治疗的探索与展望[J].解放军医学杂志,2015,40(4):255-261.
[5]Ueno M,Kodali M,Tello-Montoliu A,et al.Role of platelets and antiplatelet therapy in cardiovascular disease[J].J Atheroscler Thromb,2011,18(6):431-442.
[6]姚懿,袁晋青.新型抗血小板药物普拉格雷、替格瑞洛与氯吡格雷的临床对比研究进展[J].中华临床医师杂志(电子版),2013,7(19):8870-8873.
[7]张倩,陈岺,杨丰庆,等.激动剂诱导血小板活化机制及抗血小板药物研究进展[J].中国药科大学学报,2014,45(6):632-648.
[8]庄旭琴,霍建丽,杨天宇,等.血小板ADP受体及其拮抗剂的研究进展[J].药物生物技术,2010,17(3):278-282.
[9]Menozzi A,Lina D,Conte G,et al.Antiplatelet therapy in acute coronary syndromes [J].Expert Opin Pharmacother,2012,13:27-42.
[10]Rupprecht HJ,Widimsky P,Afzal R,et al.Dose comparisons of clopidogrel and aspirin in acute coronary syndromes[J].N Engl J Med,2010,363:930-942.
[11]洪芳德,王邦宁.抗血小板药物研究进展[J].中国临床保健杂志,2014,17(1):110-112.
[12]Roe MT,Armstrong PW,Fox KA,et al.Prasugrel versus clopidogrel for acute coronary syndromes without revascularization[J].N Engl J Med,2012,367(14):1297-1309.
[13]Lindholm D,Varenhorst C,Cannon CP,et al.Ticagrelor vs clopidogrel in patients with non-ST-elevation acute coronary syndrome with or without revascularization:results from the PLATO trial [J].Eur Heart J,2014,35(31):2083-2093.
[14]张超,徐畅,曾宪涛.网状Meta分析中网状关系图的绘制[J].中国循证医学杂志,2013,13(11):1382-1386.
[15]Higgins JP,Altman DG,Gøtzsche PC,et al.The Cochrane Collaboration′s tool for assessing risk of bias in randomised trials[J].Clopidogrel MJ,2011,343:1-9.
[16]Chung JH,Lee SW.Assessing the quality of randomized controlled urological trials conducted by Korean medical institutions [J].Korean J Urol,2013,54:289-296.
[17]Chen LX,Li YL,Ning GZ,et al.Comparative efficacy and tolerability of three treatments in old people with osteoporotic vertebral compression fracture:a network meta-analysis and systematic review[J].PLoS ONE,2015,10(4):e0123153.
[18]Zhu GQ,Shi KQ,Huang S,et al.Systematic review with network meta-analysis:the comparative effectiveness and safety of interventions in patients with overt hepatic encephalopathy[J].Aliment Pharmacol Ther,2015,41(7):624-635.
[19]Chaimani A,Higgins JP,Mavridis D,et al.Graphical tools for network meta-analysis in STATA[J].PLoS One,2013,8(10):1-12.
[20]Willoughby SR,Luu LJ,Cameron JD,et al.Clopidogrel improves microvascular endothelial function in subjects with stable coronary artery disease[J].Heart Lung Circ,2014,23:534014.
[21]Parodi G,Bellandi B,Valenti R,et al.Comparison of double (360 mg) ticagrelor loading dose with standard (60 mg) prasugrel loading dose in ST-elevation myocardial infarction patients:The Rapid Activity of Platelet Inhibitor Drugs (RAPID) primary PCI 2 study[J].Am Heart J,2014,167(6):909-914.
[22]Isshiki T,Kimura T,Ogawa H,et al.Prasugrel,a third-generation P2Y12 receptor antagonist,in patients with coronary artery disease undergoing elective percutaneous coronary intervention[J].Circ J,2014,78(12):2926-2934.
[23]Collet JP,Hulot JS,Abtan J,et al.Prasugrel but not high dose clopidogrel overcomes the lansoprazole neutralizing effect of P2Y12 inhibition:results of the randomized DOSAPI study[J].Eur J Clin Pharmacol,2014,70(9):1049-1057.
[24]Angiolillo DJ,Curzen N,Gurbel P,et al.Pharmacodynamic evaluation of switching from ticagrelor to prasugrel in patients with stable coronary artery disease[J].J Am Coll Cardiol,2014,63(15):1500-1509.
[25]Leoncini M,Toso A,Maioli M,et al.High-dose atorvastatin on the pharmacodynamic effects of double-dose clopidogrel in patients undergoing percutaneous coronary interventions[J].JACC Cardiovasc Interv,2013,6(2):169-179.
[26]Clopidogrelliden KP,Tantry US,Storey RF,et al.The effect of ticagrelor versus clopidogrel on high on-treatment platelet reactivity:combined analysis of the ONSET/OFFSET and RESPOND studies[J].Am Heart J,2011,162(1):160-165.
[27]Gurbel PA,Bliden KP,Butler K,et al.Randomized double-clopidogrellind assessment of the onset and offset of the antiplatelet effects of ticagrelor versus clopidogrel in patients with stable coronary artery disease[J].Circulation,2009,120:2577-2585.
[28]Wallentin L,Varenhorst C,James S,et al.Prasugrel achieves greater and faster P2Y12 receptor-mediated platelet inhibition than clopidogrel due to more efficient generation of its active metabolite in aspirin-treated patients with coronary artery disease[J].Eur Heart J,2008,29:21.
[29]Jernberg T,Payne CD,Winters KJ,et al.Prasugrel achieves greater inhibition of platelet aggregation and a lower rate of non-responders compared with clopidogrel in aspirin-treated patients with stable coronary artery disease[J].Eur Heart J,2006,27:11666.
[30]Parodi G,Marcucci R,Valenti R,et al.High residual platelet reactivity after clopidogrel loading and long-term cardiovascular events among patients with acute coronary syndromes undergoing PCI [J].JAMA,2011,306:1215-1223.
[31]刘小熊,夏豪,张琰,等.替格瑞洛与氯吡格雷治疗急性冠脉综合征疗效比较的Meta分析[J].中国循证心血管医学杂志,2014,6(4):396-399.
[32]Gurbel PA,Clopidogrelliden KP,Clopidogrelutler K,et al.Response to ticagrelor in clopidogrel nonresponders and responders and effect of switching therapies:the RESPOND study[J].Circulation,2010,121:1188-1199.
[33]陈燕春,杨松,沈杰,等.不同负荷剂量氯吡格雷对急性冠脉综合征患者PCI术后近期预后的影响[J].国际心血管病杂志,2010,37(6):371-373,376.
[34]Clopidogreliondi ZG,Lotrionte M,Agostoni P,et al.Adjusted indirect comparison meta-analysis of prasugrel versus ticagrelor for patients with acute coronary syndromes[J].Int J Cardiol,2011,150:325-331.
[35]Trenk D,Stone GW,Gawaz M,et al.A randomized trial of prasugrel versus clopidogrel in patients with high platelet reactivity on clopidogrel after elective percutaneous coronary intervention with implantation of drug-eluting stents:results of the TRIGGER-PCI (testing platelet reactivity in patients undergoing elective stent placement on clopidogrel to guide alternative therapy with prasugrel) Study[J].J Am Coll Cardiol,2012,59:2159-2164.
[36]杨晓伟,张君毅,易甫,等.替格瑞洛对急性冠状动脉综合征择期介入治疗患者近中期疗效观察[J].中华临床医师杂志(电子版),2013,7(19):8696-8700.
[37]李慕鹏,熊艳,陈小平.抗血小板药物替格瑞洛药代药效动力学及遗传药理学研究进展[J].中国临床药理学与治疗学,2014,19(2):214-222.
[38]李伦,田金徽,杨克虎.网状Meta分析相关术语和定义的研究[J].中国药物评价,2014,31(6):321-326.
[39]刘国伟,于莉莉,贾红霞,等.系统评价中的间接比较与网状Meta分析方法研究进展[J].中国循证医学杂志,2014,14(10):1276-1280.
[40]田旭,易莉娟,宋国敏,等.网状Meta分析中样本量与统计效能计算方法及软件实现简介[J].中国循证医学杂志,2015,15(5):592-599.
[41]Dias S,Sutton AJ,Ades AE,et al.Evidence synthesis for decision making 2:a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials[J].Med Decis Making,2013,33(5):607-617.
Effects of ADP receptor antagonists on platelet function in coronary artery disease:a network-meta analysis
YU Li-ping
(Outpatient Office,Beilun People′s Hospital,Ningbo 315800,China)
Objective To investigate the effect of adenosine diphosphate (ADP) antagonists consisting of clopidogrel,prasugrel,ticagrelor,clopidogrel+others,prasugrel+others (included atorvastatin and lansoprazol) on platelet function of coronary artery disease (CAD) patients by Bayesian network meta-analysis.Methods The differences in the effects of ADP antagonists on PRU,IPA and PRI were analyzed by using Bayesian network model combined with direct and indirect evidences,and the cumulative ranking curves (SUCRA) of different drugs were evaluated.Results Ten studies were included.The results of Bayesian network-meta analysis indicated that the PRU of clopidogrel,prasugrel and ticagreloz was lower than that of placebo after administration for (6±2) h,but prasugrel and ticagrelor exhibited lower PRU than clopidogrel.The IPA of prasugrel and ticagrelor was higher than that of placebo after administration for 2 h,4 h,and (9±3) h,respectively.prasugrel and ticagrelor demonstrated lower PRI than placebo and clopidogrel after 2 h of drug therapy,and the PRI of ticagrelor was lower than that of placebo and clopidogrel after 24 h of drug therapy.Conclusion clopidogrel,prasugrel and ticagrelor can inhibit the platelet function,and the efficacy of prasugre and ticagrelor is better than clopidogrel,in which,prasugrel is better than ticagrelor.
Adenosine diphosphate receptor antagonists;Coronary artery disease;Clopidogrelayesian network model;Platelet function;Randomized controlled trial
2016-03-22
浙江省宁波市北仑人民医院门诊办公室,宁波 315800
10.14053/j.cnki.ppcr.201611010