Know ledge,attitude and recommenda tions for p ractice regarding dengue among the resident population of Queensland,Australia
2016-09-07NarayanGyawaliRichardStewartBradburyAndrewilliamTaylorRobinsonSchoolofMedicalandAppliedSciencesCentralQueenslandUniversityRockhamptonAustralia
Narayan Gyawali,Richard Stewart Bradbury,Andrew W illiam Taylor-RobinsonSchool of Medical and Applied Sciences,Central Queensland University,Rockhampton,Australia
Know ledge,attitude and recommenda tions for p ractice regarding dengue among the resident population of Queensland,Australia
Narayan Gyawali,Richard Stewart Bradbury,Andrew W illiam Taylor-Robinson*
School of Medical and Applied Sciences,Central Queensland University,Rockhampton,Australia
Epidemiological investigation http://dx.doi.org/10.1016/j.apjtb.2016.01.002
ARTICLE INFO
Article history:
Received in revised form 4 Nov, 2nd revised form 11 Nov 2015 Accepted 22 Nov 2015
Availableonline8 Jan 2016
Dengue
Awareness Survey
Transm ission Prevention
Queensland
ABSTRACT
Ob jective:To investigate levels of awareness of dengue among the inhabitants of Queensland(QLD),a dengue-prevalent state in the north east of Australia.
M ethods:A computer-assisted telephone interview ing survey was conducted in m id 2014.A totalof1223 random ly selected respondents(≥18 years)acrossQLD completed a structured questionnaire covering all aspects of dengue.
Results:97.55%had heard of dengueand participated further.Among them,54.70%had travelled overseas(48.11%to dengue-risk countries)in the last fi ve years.A total of 94.47%said transm ission is by mosquito bite.In addition,84.83%knew of current transm ission of dengue in QLD,while 80.97%knew the focus is Far North and North QLD.Furthermore,2.35%and 8.97%had experienced an infection in their life or thatof their immediate fam ily/partner,respectively.85.03%identi fi ed correctly at leastonemeans of prevention.A total of 69.72%advised to use insect repellent,wear covered clothing and avoid visiting mosquito-prone areaswhile 20.93%advised fum igation and clearing water containers around residences.Therewas a signi fi cantdifference(P<0.05)between residents of South East QLD and the rest of QLD regarding know ledge of prevention. However,such awarenesswas not affected signi fi cantly by overseas travel(P>0.05). Conclusions:A lthoughmany people throughoutQLD have heard of dengue,about15% appear unaware of local transmission,its symptoms and of methods to reduce risk of infection.A lack of know ledge regarding prevention ofmosquito breeding is evident in South East QLD,where dengue is not currently reported.The study suggests that future dengue awareness campaigns should target communities in both endem ic and potentially endem ic areas throughout Queensland.
1.Introduction
Dengue,a mosquito-borne viral disease of humans,has in recent years drawn increased worldw ide public health concern. Over 3.6 billion inhabitants of the tropics and subtropics are currently at risk of infection[1],w ith an estimated 390 m illion dengue infections reported per year in around 130 countries worldw ide[2,3].The causative agent of the disease is the enveloped,icosahedral,single stranded positive-sense RNA virus dengue,a member of the fam ily Flaviviridae and genus Flavivirus.Based on differences in antigen neutralization tests fi ve serotypes(DENV-1 to DENV-5)are now recognized[4]. The mosquito species that are principally responsible for dengue transm ission,Aedes aegypti and Aedes albopictus[5], are distributed mainly in tropical localities,including the Asia–Paci fi c region,in parts of which it is endem ic[6].The nature of disease ranges from m ild self-lim iting illness,dengue w ith warning signs(abdom inal pain,persistent vom iting,fl uid accumulation,mucosal bleeding,lethargy,increasing haematocritw ith decreasing platelets),to severe dengue(dengue w ith severe plasma leakage,severe bleeding,or organ failure)[7].Despite decades of intensive research,the presentunavailability of an effective antiviral drug and/or licensed vaccine makes dengue amajor global public health priority[8,9].
Dengue isan emerging concern in Australia.Therehavebeen occurrences of infection in Queensland(QLD)formany years, w ith local transm ission resulting in multiple outbreaks in Northern QLD[10,11].A major outbreak in March 2009 and continuing sporadic incidences have further alerted state authorities to the public health risk posed by dengue.A large outbreak of DENV-2 in 1992–93 has left a sustained potential threat.In the intervening period,there have beenmore than 40 outbreaks comprising 3086 con fi rmed cases and causing three deaths[12].The number of overseas travel-associated cases of dengue,almost10 times higher than locally acquired,continues to increaseannually:1390 in 2011–12;1133 in 2010–11;593 in 2009–10;350 in 2007–08[13,14].
In response to the real and perceived threat to the resident population of QLD,the State Government has launched successive denguemanagement plans,themost current iteration of which concludes soon[15].However,risk of outbreak is always ampli fi ed when communities are not aware of the disease.In spite of the long history of dengue in this state,it was our anecdotal belief that local people lack suf fi cient awareness of the virus,its route of transmission,and the disease it causes. Thus,the aim of the present survey was to investigate know ledge of and attitude towards dengue among the people of QLD.Awareness level is an extremely important factor in determ ining a strategy for future public health policies. W ithout this information,scarce resources for rural and regional health may easily be directed towards information campaigns that do little to alter the community's current understanding of preventivemeasures.Hence,this study holds pragmatic value to policy makers of QLD for implementing a public health information drive to assist in the reduction,and ultimately prevention,of dengue in QLD.A lso,it provides a useful point of reference for health educators in countries of the Western Paci fi c,North America and Europe,where, sim ilar to Australia,dengue poses an increasing threat.
2.M aterials and m ethods
The survey was conducted by a highly experienced team of trained telephone operators from the 2014 Queensland Social Survey(QSS 2014).Thiswas the tenth annualstate-w ide survey adm inistered by the Population Research Laboratory(PRL) based at the Rockhampton campus of Central Queensland University.The QSS is an omnibus-style survey of households in QLD that is acknow ledged to provide a structured research framework that serves as a reliable,credible,and relatively lowcost data collection vehicle.
2.1.Survey instrument
The survey consisted of three components:1)a standardized introduction;2)socio-demographic questions;and 3)questions that speci fi cally addressed the interests of the researchers participating in the study,including awareness of denguewhich constituted our research study.For the second component,information was requested on household composition,gender, age,marital status,highest level of education,household income,religion,ethnicity,employment status,occupation, home ownership and sample area.For the third component,a structured questionnaire of nine standard questions,carefully designed to cover all aspect of awareness of dengue among residents of QLD,was used.Our research hypothesis was that awareness of dengue is in fl uenced by the geographical location of residence and overseas travel history of an individual.
The setof survey questions focused on dengue epidem iology in the state,mode of transmission and vector controlmethods along w ith participants'place of origin and travel history. Trained interviewers trialled the entire questionnaire on 68 households in QLD selected at random.M inor amendments to improve text of questions were made after review of pre-test frequency distributions and feedback from interviewers(e.g. comments on effect of question order on responses,inappropriate response categories,ambiguouswording).
Approval forQSS 2014 was received from the Human Ethics Research Review Comm ittee at Central Queensland University prior to its conductw ith the QLD general public.Theauthorized application was Project H13/06-120 Queensland Social Survey 2014.
2.2.Sampling design
For sampling purpose the state of QLD was delineated into two areas for telephone interview ing:South East QLD(SEQ); the remainder of QLD(non-SEQ).QLD is the second largest and third most populous state in Australia.Among an estimated 4.75m illion population,more than two thirds(3.20m illion)live in SEQ,which includes the state capital Brisbane,and the metropolitan regions of Gold Coast,Sunshine Coast and West M oreton.The remainder of QLD is sparsely populated and regional or rural[16].In order to perm it the analysis of each area asa separateentity,am inimum sample sizeof 400 foreach subregion was deemed necessary.
A two-stage selection process was used to register participants:selection of households and selection of respondent genderw ithin each household.The target population designated for telephone interview ing was all persons 18 years of age or olderwho,at the timeof the survey,were living in as theirusual placeof residencean abode in QLD thatcould be contacted viaa direct-dialled,landline telecommunications connection.A random selection approach assured thateach respondenthad the same likelihood of being contacted.The PRL used a telephone database of random ly generated landline telephone numbers which had been selected using postcode parameters and washed to remove known non-residential and non-working numbers. Each household was random ly pre-selected as either amale or female household.W ithin the household,one eligible person was selected as the respondent for the interview.If there was more than onemale/female in the household then themale/female thathad themost recentbirthday wasselected.If therewas no one of the pre-selected gender residing in the house then the house was designated not quali fi ed.
2.3.Data collection
QSS 2014 was performed utilising a twenty-station computer-assisted telephone interview ing(CATI)system linked to a local area network at the PRL.This facility enabled informationexchangebetween interview ing PC stationsand a supervisorhub connected by a shared fi le server.Supervisorsmonitored each call deposition,after which data were edited,validated and compiled for analysis.
Follow ing the pilot test,the sample database was uploaded to the CATI system which assigns telephone numbers to interview ing stations.Instructions and questions were show n on the PC screen to the interviewer who spoke to the respondent by telephone.As interviewers entered the responses provided into the PC while each interview took place, itwas possible tomonitor continually closed-ended responses. A ll PRL staff involved in the study were required to sign a con fi dentiality statement before the commencement of data collection.
Interview ing took place between 29 July and 31 August 2014.Interviews were conducted between the hours of 10:30–14:30 Monday,Wednesday and Friday,16:30–18:30 Monday to Friday,and 12:00–16:00 on Saturday and Sunday.If interviewers were unsuccessful in establishing contact on their fi rstcall,aminimum of fi ve call-back attemptswasmade.Upon making contact,interviewers identi fi ed themselves and then asked the screening questions for selecting the respondent.The average complete interview length was 29 m in.
2.4.Data analysis
The estimated sampling error for the totalsample,at the 95% con fi dence level,was±2.8%,19 times out of 20.Respondents 65 years and older were overrepresented(33.6%)while there was under sampling of the under 35 age categories(7.8%). Gaining adequate participation of younger respondents when conducting CATI surveys using random ly generated landline telephone samples has become more dif fi cult as this demographic has been particularly affected by the shifting pattern towards preference for exclusive use of mobile phones.However,recent studies have shown that the exclusion of mobile phone only households may currently have only low or nonsigni fi cant impacts upon estimates obtained using these data [17,18].
The collected data were tabulated and analysed using SPSS version 19.A Chi-square test(x2)was performed using 95% con fi dence intervals(CI)in order to determ ine the association between overseas travellers and non-travellers,and between SEQ and non-SEQ residentsw ith respect to their know ledge of dengue and its prevention.
3.Resu lts
3.1.Socio-demographic characteristics of respondents
Of 3438 individuals contacted for the QSS 2014,1223 completed the survey,a response rate of 35.57%.This is in line w ith the response rate for general household telephone surveys in recent years[19].A total of 814(66.56%)householderswere sampled from SEQ and 409(33.44%)from non-SEQ.These sample sizes are closely proportional to the state populations they represent,as indicated by themost recentAustralian Bureau of Statistics census data[20].An equal proportion ofmales and females w ith amean age of(57.2±15.5)years participated in the study.About 77.76%(951/1223)of respondents were born in Australia;regardless of the country of birth,themean time spent living in Australia was 55.35 years.Table 1 shows the major socio-demographic characteristics of respondents in the sample areas.
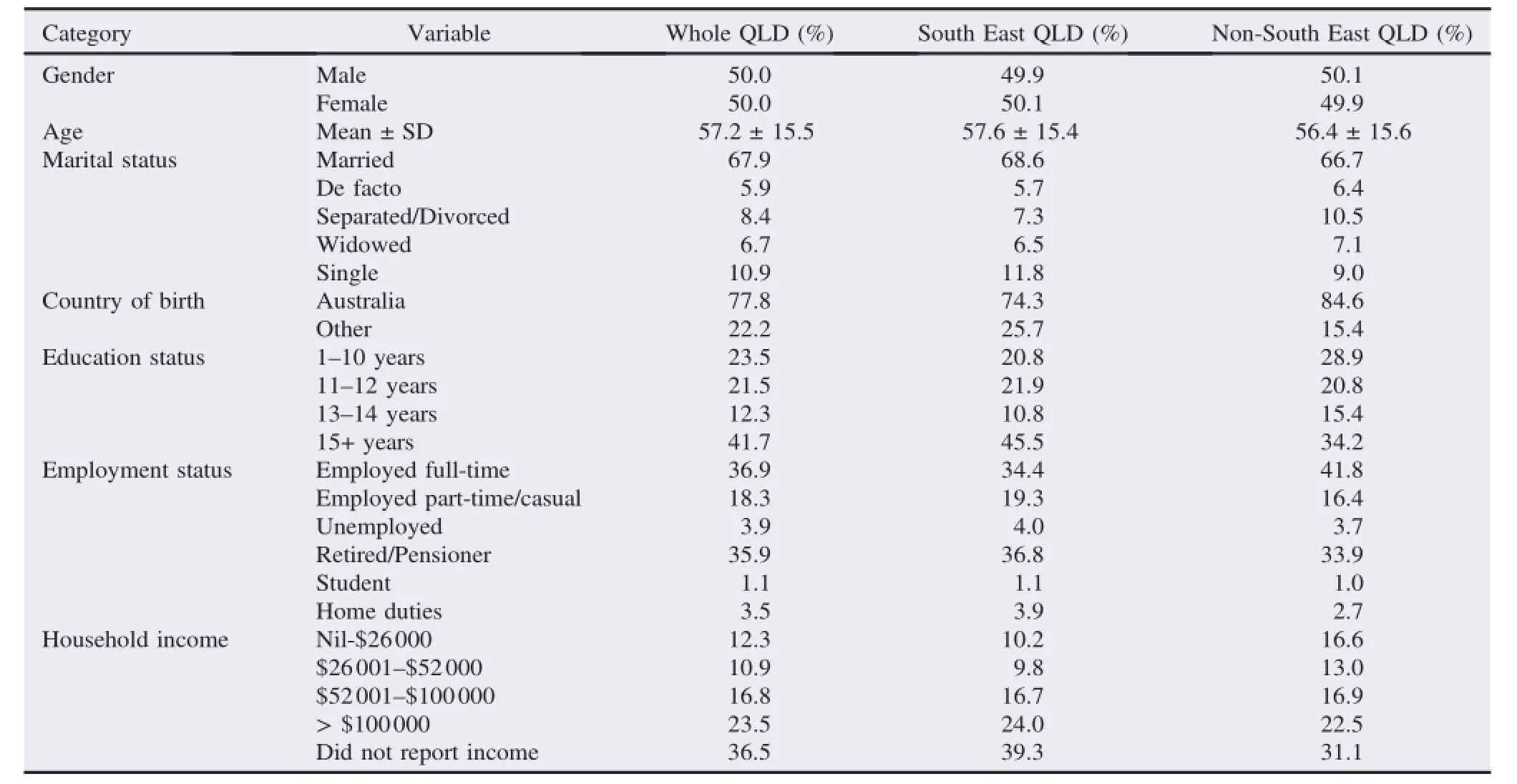
Table1 Major socio-demographic characteristics of survey respondents.
3.2.Travel history of respondents
54.70%(669/1223)of all participants had travelled overseas in the last fi ve years.Among SEQ inhabitants,60.81%(495/ 814)provided an overseas travel history,while only 43.52% (178/409)of non-SEQ respondents did sim ilarly(P<0.05). Respondents collectively reported visiting 106 countries in the last fi ve years.Nearly half(48.11%;51/106)of the nations visited by participants are listed as dengue-risk countries by the World Health Organization.The principal destinations for travel are depicted in Figure 1.

Figure 1.Dengue-risk countries to which QLD residents travelled in the last fi ve years.FJ:Fiji;HK:Hong Kong;IN:India;ID:Indonesia;MY:Malaysia;NG: Papua New Guinea;PH:Philippines;SG:Singapore;ZA:South Africa; TH:Thailand;VN:Vietnam;PI:Paci fi c Islands;SA:South America. Numbers signify total of individual responses per nation,region or continent.
3.3.Respondents'knowledge of dengue:symptoms and transmission of infection
A total of 97.55%(1193/1223)of participants claimed know ledge of dengue and so were asked further questions. About 2.35%(28/1193)of these respondents had experienced dengue infection;1.28%(10/793)and 4.5%(18/400)from SEQ and non-SEQ,respectively(Table 2).About 8.97%(107/1193) indicated that their partner or an immediate fam ily member had been infected.In addition,46.02%(549/1193)of participants identi fi ed correctly the typical symptoms of dengue,such as fever,rash,headache,muscle and joint pain.Furthermore, 84.83%(1012/1193)knew of the current transm ission of dengue in QLD,and 80.97%(966/1193)identi fi ed correctly the major areas in the state where past epidem ics of dengue have occurred.The response rate was in follow ing order:Far North QLD>North QLD>Central QLD.There was no signi fi cant difference in the views of respondents from geographically distinct locations(P>0.05).
Among these,94.47%(1127/1193)responded correctly that dengue is transm itted bymosquito bite,3.27%(39/1193)did not know themode of transm ission,while the remaining 2.26%(27/ 1193)offered the view that it is caused by bad food,water, coughing or unwashed hands.Regarding know ledge of transm ission,no signi fi cantdifferencewas found between inhabitants of SEQ and non-SEQ,and between overseas travellers and nontravellers(P>0.05)(Table 3).

Table2 Survey respondents'experience of dengue infection.

Table3 Survey respondents'know ledge of dengue transm ission.
3.4.Respondents'know ledge of dengue:control and prevention of infection
3.10%participants(37/1193)did not give a response regarding vector control,so the sample population for this question was reduced to 1156.In addition,7.01%(81/1156)of respondents expressed no know ledge of vector control,but 85.03%(983/1156)had at least an idea of suitable methods, identifying correctly at least one appropriatemeans of prevention.About 69.72%(806/1156)responded to avoid mosquito bites by applying insect repellent,wearing covered clothing, avoiding visiting mosquito-prone areas,while 20.93%(242/ 1156)showed an appreciation of vector control by disturbance of mosquito breeding(clearing water containers around,and fum igation of residential sites).Inhabitants of SEQ weresigni fi cantly less know ledgeable of dengue prevention w ith regard to elim inating vector breeding sites than residents of other regions of QLD(P<0.05).There was no such difference observed between the know ledge of overseas travellers and nontravellers(P=0.23)(Table 4).Of note,2.34%(27/1156)of participants stated a dengue vaccine as ameans of prevention. of dengue into the community by a viraem ic traveller,visiting or returning from overseas or even elsewhere in QLD,who is infectious to mosquitoes[26].Potential secondary vectors are found only in Far North QLD;to date Aedes albopictus has been identi fi ed only in the Torres Strait Islands[27]and Aedes scutellaris in both the Torres Strait Islands and Cape York[28].

Table4 Survey respondents'know ledge of dengue prevention.
4.Discussion
Outbreaks of dengue in Australia date back as far as the late 19th century and have been reported across the country in Northern Territory,Queensland,New SouthWales and Western Australia[21].However,currently local transm ission occurs w ithin QLD only[15].Despite this long history of dengue in Australia,to the best of our know ledge,this is the fi rst study to be conducted to assess know ledge and attitude regarding dengue among the resident population of Australia.
The presentsurvey found that97.55%ofparticipants resident in QLD had heard of dengue.Of these individuals,94.47% knew aboutmosquito transm ission of infection.This level of awareness is higher than that reported for inhabitants of other nations:Northern Thailand,67%[22],Nepal,77%[23],and India, 90%[24].Each of these countries is dengue-endem ic[1,2],but is recognized as having a low human development index(HDI) [25].Comparing our result w ith these fi ndings assumes that peoples'know ledge may be associated w ith the development index of the country in which they live,as HDI in fl uences directly the education system,technology and media of the nation.A more valid comparison would be w ith high HDI countries for which dengue is endem ic.As Australia is unusual,but not unique,in being a highly developed nation in which local transm ission of dengue occurs,this information is not currently available.Sim ilar studies to the one reported herewould be required elsewhere.
Over four fi fths(84.83%)of participants in the survey were cognisant of the ongoing prevalence of dengue in QLD and almost all these respondents(80.97%)also knew that its occurrence and local transm ission is particularly high in the north of the state.The coverage by local,state and national Australianmedia(newspaper,television,radio and socialmedia) of previous dengue outbreaks in QLD w ill likely have raised awareness of such residents to the geographical distribution of dengue in the state.The principal vector for dengue transm ission,Aedes aegypti,is present in Far North and North QLD but ismuch less common further south.Thus,at present outbreaksare restricted largely to these regions butw illpresumably occurw ith increasing frequency elsewhere in future if the range of the vectorextendsasa consequence of globalwarm ing.Local transm ission is possible and occurs after the initial introduction
A total of 2.35%of participants had personally experienced denguewhile 8.97%knew of an infection to their partner or immediate fam ily member.This report links indirectly to the noti fi ed incidence rate of dengue in QLD,forwhich the current population is 4.75 m illion[16].The total number of recorded dengue cases in QLD in the last10 years is approximately 2000 [15].Thus,itmay be implied from our survey result thatmany participantswere infected w ith dengue over a decade ago,most probablyduring dengueoutbreaksof1992–93and 1997–99[10,12].
46.02%of participants identi fi ed correctly the commonly recognized symptoms of dengue,such as fever,rash,headache, muscle and joint pain.This total compares poorly w ith the understanding of participants of sim ilar surveys conducted in Nepal(>80%)[23],India(>70%)[24],Malaysia(>80%)[29] and Brazil(>66%)[30].These countries are dengue-endem ic and most people live in a traditional fam ily unit in a closely clustered neighbourhood as compared to themore isolated residences in QLD,especially in regional and rural areas.Hence, the greater understanding of the signs and symptoms of disease by people in these tropical locationsmay be based on their close observation of dengue infection contracted by their fam ily members and/or neighbours.
More than half(54.70%)of participants had travelled overseas in the last fi ve years.In total,51 of 106 nations visited are considered of fi cially as dengue-risk countries according to current guidelines for dengue control issued by the World Health Organization[7].These include Paci fi c Islands,Singapore, Thailand and Indonesia,the last two of which are considered hyper-endem ic for dengue w ith regular reporting of outbreaks since 2000[31].In Singapore,the number of clinical cases is rising rapidly and is anticipated to exceed 1000 per week during high season[32].At present,dengue is not a disease endem ic to Australia w ith local outbreaks con fi ned to North QLD.Since 1990 there has been almost continual annual transm ission in QLD arising from infections introduced by incom ing travellers[33].W hen a viraem ic person enters a vector-prevalent area like North QLD,they become a potential source for transmission,which may lead to a local outbreak. Currently,most imported cases originate from Indonesia, Thailand,Philippines and Papua New Guinea[13,33].An improved general know ledge of dengue would make travellers more likely to recognize its disease symptoms,and thereforeto seek medical advice if returning w ith a febrile illness from overseas,particularly a dengue-endemic region.
85.03%of survey respondents had some awareness of appropriatemeasures to take for dengue control.Among these, around two thirds advised prevention ofmosquito bites,butonly one in fi ve conveyed the concept of vector control by lim iting their breeding.Residents outside SEQ were signi fi cantly more likely to have an awareness of dengue prevention and control than those individuals living in SEQ,where there is no prevalence of dengue.This indicates that the geographical location of an individual's permanent place of residence in fl uences their awareness of the risk to their local community of dengue infection.2.34%of participantsmentioned dengue vaccination, even though a commercially available preparation is not currently available.While thismay be due to expectation of the existence of a vaccine,it may be that in part this shows awareness through the news media of drug and vaccine trial research,especially that taking place w ithin QLD[34,35].
Of particular interest,there was no notable difference in the general know ledge of dengue between those participants of the survey who had travelled overseas,even to dengue-endem ic regions,and those who had not.This fi nding did not support our hypothesis at the outset of the study,that a person's awareness of dengue is in fl uenced by their overseas travel history.This is of concern since prompt presentation formedical care and noti fi cation of public health authorities by returned travellersw ith dengue would effectively reduce the number of dengue outbreaks each year in QLD.
A lthoughmany people surveyed had heard of dengue,most of them wereunawareof the symptoms of diseaseand possessed inadequate know ledge of preventivemethods or vector control. No signi fi cant difference was found in responses to dengue awareness questions(mode of transm ission and dengue control) between overseas travellers and non-travellers.However,there was a direct correlation between the dengue prevalence of the geographical location in QLD of a person'spermanent residence w ith their know ledge of dengue control methods.Annually, travel-associated and some locally acquired dengue cases have been reported from northern parts of QLD.Public awareness of, and preparedness for,incidencesoroutbreaksof any disease can be heavily in fl uenced by communication between neighbourhood residents.Sharing of information formally among people in a community or in thework place,ormore informally among fam ily and friends are effectivemeans of know ledge transfer, especially in ruraland remote locations.In addition,localmedia outletsmake the public aware of issues of regional relevance. However,the results of this survey suggest that the ef fi cacy of dissem ination of relevant and correct information by newspapers,television and radio should be reconsidered in order to increase public understanding of dengue in QLD.
The results of this survey indicate thataround 15%of QLD residentsdo nothaveany awarenessof the prevalence of dengue w ithin the state.Sim ilarly,approximately 15%of the population would appear not to have any know ledge of its symptoms of illness,ormeans of its prevention.This know ledge gapmay not be entirely surprising given that dengue is not an emergency public health issue in QLD and the focus of outbreaks lies in sparsely populated northern tropical regions,a considerable distance from thehigherpopulation density of SEQ.It is thought that past and present public health awareness campaigns have targeted only areas of the state where the potential for establishment of the disease has or currently exists[5,15].Today, dengue vector mosquitoes are found as far south as Rockhampton which lies on the Tropic of Capricorn[13,15].
Nevertheless,particularly given the occurrence of travelassociated cases the outcomes of this study indicate the need for effective dengue awareness campaigns throughout QLD. International travellers,the vast majority of whom depart Australia from airports in Brisbane or othermajormetropolitan areas,should bemade aware of the risk of contracting dengue overseas,since travel-associated cases are themajor source of infection in QLD.
This survey provides an evidence-based indication of the level of know ledge of the resident adult population of QLD in relation to dengue.In considering plans to implement preventativemeasures againstdengue,public health policymakersmay regard this study as a reference to design revised or new strategies to control dengue in areas of transmission.
Con fl ict of interest statement
We declare thatwe have no con fl ict of interest.
Acknow ledgm ents
This study was funded by a competitive grant awarded through the QSS 2014 Population Research Grant Scheme, number H13/06-120/QSS2014-14.Itwas conducted in cooperation w ith the Population Research Laboratory,School of Human,Health&Social Sciences,Central Queensland University. The advice and assistance of laboratory manager Christine Hanley is gratefully acknow ledged.We also thank each telephone operator and all the study participants.
References
[1]Gubler DJ.Dengue viruses:theirevolution,history and emergence as a global public health problem.In:Gubler DJ,Ooi EE, Vasudevan S,Farrar J,editors.Dengue and dengue hemorrhagic fever.2nd ed.London:CABI;2014,p.1-29.
[2]Bhatt S,Gething PW,Brady OJ,Messina JP,Farlow AW, M oyes CL,et al.The global distribution and burden of dengue. Nature 2013;496(7446):504-7.
[3]Brady OJ,Gething PW,Bhatt S,Messina JP,Brownstein JS, Hoen AG,etal.Re fi ning the global spatial lim its of dengue virus transm ission by evidence-based consensus.PLoS Negl Trop Dis 2012;6(8):e1760.
[4]M ustafa MS,Rasotgi V,Jain S,Gupta V.Discovery of fi fth serotype of dengue virus(DENV-5):a new public health dilemma in dengue control.Med JArmed Forces India 2015;71(1):67-70.
[5]M ackenzie JS,la Brooy JT,Hueston L,Cunningham AL.Dengue in Australia.JMed Microbiol 1996;45(3):159-61.
[6]Higa Y.Dengue vectors and their spatial distribution.Trop Med Health 2011;39(Suppl 4):17-27.
[7]W orld Health O rganization.Dengue:guidelines for diagnosis, treatment,prevention and control.Geneva:World Health Organization;2009,p.1-160.[Online]Available from:http://www. who.int/tdr/publications/documents/dengue-diagnosis.pdf [Accessed on 29th October,2015]
[8]Wan SW,Lin CF,Wang S,Chen YH,Yeh TM,Liu HS,et al. Currentprogress in dengue vaccines.JBiomed Sci2013;20(1):37.
[9]Gyawali N,Taylor-Robinson AW.Vaccine development against dengue,a viral disease of increasing signi fi cance to global public health.Immun Dis 2014;2(a10):1-4.
[10]Hanna JN,Ritchie SA,Phillips DA,Sera fi n IL,Hills SL,van den Hurk AF,etal.An epidemic of dengue 3 in Far North Queensland, 1997–1999.Med JAust2001;174(4):178-82.
[11]Hanna JN,Ritchie SA,Richards AR,Taylor CT,Pyke AT, Montgomery BL,etal.Multiple outbreaksof dengue serotype 2 in North Queensland,2003/04.AustN Z JPublic Health 2006;30(3): 220-5.
[12]M cBride W J,Mullner H,LaBrooy JT,W ronski I.The 1993 dengue 2 epidemic in Charters Towers,North Queensland:clinical features and public health impact.Epidemiol Infect 1998;121(1): 151-6.
[13]Knope K,Doggett S,Kurucz N,Johansen CA,Nicholson J, Feldman R,et al.A rboviral diseases and malaria in Australia, 2011–12:annual report of the National Arbovirus and M alaria Advisory Comm ittee.Commun Dis Intell Q Rep 2014;38(2): E122-42.
[14]Knope K,Whelan P,Smith D,Johansen C,Moran R,Doggett S, etal.A rboviral diseasesandmalaria in Australia,2010–11:annual reportof the National A rbovirusand M alaria Advisory Comm ittee. Commun Dis Intell Q Rep 2013;37(1):E1-20.
[15]Queensland Government.Queensland dengue management plan (DMP)2010–2015.Brisbane:Communicable Diseases Branch, Queensland Health;2011,p.1-47.[Online]Available from:https:// www.health.qld.gov.au/publications/clinical-practice/guidelinesprocedures/diseases-infection/governance/dengue-mgt-plan.pdf [Accessed on 29th October,2015]
[16]Queensland Government.Population grow th,Queensland, December quarter 2014.Brisbane:Queensland Government's Statistician Of fi ce;2015.[Online]Available from:http://www. qgso.qld.gov.au/products/reports/pop-grow th-qld/pop-grow th-qld-201412.pdf[Accessed on 29th October,2015]
[17]Pennay DW,Bishop N.Pro fi ling the‘mobilephoneonly’population: astudyofAustralianswithamobilephoneand no landline telephone. M elbourne:Social Research Centre Pty Ltd;2009,p.1-18.
[18]Dal Grande E,Taylor AW.Sampling and coverage issues of telephone surveys used for collecting health information in Australia:results from a face-to-face survey from 1999 to 2008. BMC Med Res Methodol 2010;10:77.
[19]Curtin R,Presser S,Singer E.Changes in telephone survey nonresponse over the past quarter century.Public Opin Q 2005; 69(1):87-98.
[20]Australian Bureau of Statistics.3218.0-Regional population growth,Australia,2013–14.Estimated resident population,statistical local areas,Queensland.Canberra:Australian Bureau of Statistics;2015.[Online]Available from:http://www.abs.gov.au/ ausstats/abs@.nsf/m f/3218.0/[Accessed on 29th October,2015]
[21]Lum ley GF,Taylor FH.Dengue:service publication number 3. Sydney:School of Public Health and Tropical Medicine,University of Sydney&Commonwealth Department of Health;1943, p.1-171.
[22]Van Benthem BH,KhantikulN,PanartK,Kessels PJ,Somboon P, Oskam L.Know ledge and use of prevention measures related to dengue in Northern Thailand.Trop Med Int Health 2002;7(11): 993-1000.
[23]Dhimal M,Aryal KK,Dhimal M L,Gautam I,Singh SP, Bhusal CL,et al.Know ledge,attitude and practice regarding dengue fever among the healthy population of highland and low land communities in central Nepal.PLoS One 2014;9(7): e102028.
[24]Acharya A,Goswam i K,Srinath S,Goswam i A.Awarenessabout dengue syndrome and related preventive practices amongst residents of an urban resettlement colony of South Delhi.J Vector Borne Dis 2005;42(3):122-7.
[25]United Nation Development Programme.Human development reports.International human development index.New York:United Nation Development Programme;2014.[Online]Available from: http://hdr.undp.org/en/content/table-1-human-development-indexand-its-components[Accessed on 29th October,2015]
[26]Mannestål Johansson C,M cBrideWJH,Engstr¨om K,M ills J.Who brings dengue into North Queensland?A descriptive,exploratory study.Aust JRural Health 2012;20(3):150-5.
[27]Ritchie SA,Moore P,Carruthers M,W illiam s C,Montgomery B, Foley P,et al.Discovery of a w idespread infestation of Aedes albopictus in the Torres Strait,Australia.JAm Mosq Control Assoc 2006;22(3):358-65.
[28]Lee DJ,Hicks MM,Grif fi ths M,Debenham ML,Bryan JH, RussellRC,etal.The culicidae of the Australasian region.Vol.4. Nomenclature,synonymy,literature,distribution,biology and relation to disease.Canberra:Australian Government Publishing Service;1987,p.1-324.
[29]Hairi F,Ong CH,Suhaimi A,Tsung TW,bin Anis Ahmad MA, Sundaraj C,et al.A know ledge,attitude and practices(KAP) study on dengue am ong selected rural comm unities in the Kuala Kangsar District.Asia Pac J Public Health 2003;15(1): 37-43.
[30]D´egallier N,Vilarinhos PT,de Carvalho M L,Knox MB, Caetano J Jr.Peop le's know ledge and practice about dengue,its vectors,and controlmeans in Brasilia(DF),Brazil:its relevance w ith entomological factors.JAm Mosq Control Assoc 2000;16(2): 114-23.
[31]Dash AP,Bhatia R,Kalra NL.Dengue in South-East Asia:an appraisal of case management and vector control.Dengue Bull 2012;36:1-13.
[32]Khalik S.Dengue cases expected to surpass 1 000 a week in Singapore.Singapore:The Straits Times;2013.[Online] Available from:http://yourhealth.asiaone.com/content/denguecases-expected-surpass-1000-week[Accessed on 29th October, 2015]
[33]Knope K,National Arbovirus and Malaria Advisory Committee, Giele C.Increasing noti fi cations of dengue in Australia related to overseas travel,1991 to 2012.Commun Dis IntellQ Rep 2013;37: E55-9.
[34]Enserink M.Infectious diseases.Australia to test‘mosquito vaccine’against human disease.Science 2010;330(6010):1460-1.
[35]Cooper D.Dengue breakthrough:protein discovery could‘jumpstart human drug trials’.Brisbane:ABC New s;2015.[Online] Available from:http://www.abc.net.au/news/2015-09-10/denguediscovery-could-jumpstart-drug-trials/6762290[Accessed on 29th October,2015]
27 Oct 2015
*Corresponding author:Prof.Andrew W illiam Taylor-Robinson,School of Medical and Applied Sciences,Central Queensland University,Bruce Highway, Rockhampton,QLD 4702,Australia.
Tel:+617 49232008
E-mail:a.taylor-robinson@cqu.edu.au
The study p rotocol was performed according to the Helsinki declaration and approved by the Human Ethics Research Review Comm ittee of Central Queensland University.A con fi dentially agreementw as signed by each survey interviewer and informed verbal consentw as obtained from each participant.
Foundation Project:Supported by a competitive grantaw arded through the QSS 2014 Population Research Grant Schem e(Grant No.H 13/06-120/QSS2014-14).
Peer review under responsibility of Hainan M edical University.The journal implements double-blind peer review practiced by specially invited international editorial boardmembers.
2221-1691/Copyright©2016 Hainan Medical University.Production and hosting by Elsevier B.V.This is an open accessarticle under the CC BY-NC-ND license(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
杂志排行

Asian Pacific Journal of Tropical Biomedicine的其它文章
- The African Moringa is to change the lives ofm illions in Ethiopia and far beyond
- Salivary leptin concentrations in Bruneian secondary school children
- Characteristics o f obese or overweight dogs visiting private Japanese vete rinary c linics
- Risk factors from HBV infection among blood donors:A system atic review
- Com putational in telligence in tropicalm edicine
- Pediculosis capitis among p rimary and m idd le school children in Asadabad,Iran:An epidem iological study