改良型FRⅢ型矫治器矫治安氏Ⅲ类错 后舌骨位置的对比研究
2016-08-19朱远平段银钟
朱远平 段银钟
1.宜昌市第二人民医院,三峡大学第二人民医院口腔科,宜昌 443000;2.第四军医大学口腔医学院,西安 710032
改良型FRⅢ型矫治器矫治安氏Ⅲ类错 后舌骨位置的对比研究
朱远平1段银钟2
1.宜昌市第二人民医院,三峡大学第二人民医院口腔科,宜昌 443000;2.第四军医大学口腔医学院,西安 710032
目的比较改良型FRⅢ型矫治器矫治儿童安氏Ⅲ类错前后舌骨位置的变化。方法选取儿童功能性安氏Ⅲ类错患者40例,实验组和对照组各20例,实验组病例采用改良型FRⅢ型矫治器矫治,对照组病例采用传统FRⅢ型矫治器矫治,对两组病例矫治前后的X线头影测量片上的舌骨位置进行对比分析。结果改良型FRⅢ型矫治器矫治儿童功能性安氏Ⅲ类错后舌骨的位置,与其治疗前比较,H-FH、H-S、H-Ptm、Ar-H-Me增大(P<0.01),H-MP、H-RGn减小(P<0.01);与传统FRⅢ型矫治器矫治后的儿童功能性安氏Ⅲ类错患者的舌骨位置比较,HFH、H-S、H-Ptm增大(P<0.05),Ar-H-Me角度增大(P<0.01),H-MP、H-RGn减小(P<0.05)。结论经改良型FRⅢ型矫治器矫治后的儿童安氏Ⅲ类错患者的舌骨位置,与其治疗前相比,位置更靠后、下,下颌骨与舌骨位置发生了顺时针旋转;比传统FRⅢ型矫治器矫治后下颌骨与舌骨位置发生顺时针旋转的角度更大,下颌在发生后下位移的同时,更有效地促进了舌骨位置的后上移位,对儿童功能性安氏Ⅲ类错患者的舌骨位置有显著影响。
改良型FRⅢ型矫治器;安氏Ⅲ类错;舌骨位置
1 材料和方法
1.1对象
1.2方法
1.2.1改良FRⅢ型矫治器[4]与传统FRⅢ型矫治器比较,作了以下4点改良:1)上颌两侧唇挡与颊屏之间的连接改为“U”型曲(图1a);2)在下颌与前腭弓相对应的位置设计一根与前腭弓形状相同的前舌弓(图1b);3)颊屏内凹状改为外凸状(图1c);4)上颌软硬腭交界中份加一个能前后旋转的小球(图1d)。
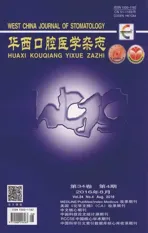
1.2.2确定标志点和测量项目由同一名技师对40例安氏Ⅲ类错患者拍摄治疗前后的X线头影测量片,并由同一名正畸医师将颅颌侧面结构及舌骨影像描于硫酸纸上,参照Adamidis等[5]方法,确定标志点及测量项目(图2)。标志点如下。P点:机械耳点;O点:眶下缘之最低点;Ptm点:翼上颌裂轮廓之最下点;FH平面:眼耳平面;MP平面:下颌平面;RGn点:颏后点;Ar点:颅底下缘与下颌颏突颈后缘之交点;Me点:颏部之最下点;S点:蝶鞍中心点;H点:舌骨体最前上点。垂直测量项目如下。1)H-FH:舌骨最前上点到眶耳平面的垂直距离;2)H-MP:舌骨最前上点到下颌平面的垂直距离;3)H-S(Ver):舌骨至蝶鞍的垂直距离。水平测量项目如下。1)H-Ptm:舌骨最前上点到Ptm点所作FH平面垂线的水平距离;2)H-RGn:舌骨最前上点到颏后点的距离。角度测量项目为Ar-H-Me,代表舌骨相对于下颌骨的位置。

图1 改良型FRⅢ型矫治器Fig 1 Improved appliance FRⅢ
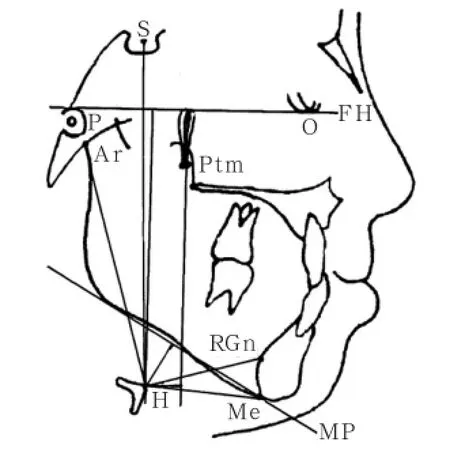
图2 测量标志点及测量项目Fig 2 Landmarks and measurements of hyoid bone position
1.2.3资料收集和分析所有项目都测量3次,取其平均值,3次结果均无显著性差异。两组病例在矫治前同一项目各测量值间差异无统计学意义(P>0.05),具有可比性。然后将结果输入SPSS 13.0软件行统计学分析,组内比较行配对计量资料t检验,组间比较行两样本均数差别t检验,检验水准α=0.05。
2 结果
2.1矫治前后舌骨位置的比较
表1 功能性Ⅲ类错患者治疗前后舌骨位置的比较Tab 1 Comparison of the hyoid bone position between functional class Ⅲ malocclusion before and after treatment n=20

表1 功能性Ⅲ类错患者治疗前后舌骨位置的比较Tab 1 Comparison of the hyoid bone position between functional class Ⅲ malocclusion before and after treatment n=20
注:a为P<0.05,b为P<0.01。
对照组[2]测量项目实验组 t值矫治前 矫治后 矫治前 矫治后 实验组 矫治后矫治前/后 对照组/实验组H-FH/mm 82.66±7.10 87.85±4.89 83.79±3.38 91.67±4.19 9.286 5b 2.648 4aH-MP/mm 11.87±5.58 12.01±4.46 11.87±1.48 9.58±1.57 12.461 2b 2.298 4aH-S(Ver)/mm 101.40±7.20 105.56±6.34 101.56±3.22 109.38±4.46 12.267 9b 2.203 9aH-Ptm/mm 9.21±6.78 11.99±4.01 10.01±1.04 14.50±1.33 21.882 5b 2.067 6aH-RGn/mm 36.55±3.88 36.41±3.41 35.65±3.07 31.34±3.56 10.989 7b 2.275 1aAr-H-Me/° 122.39±9.69 120.43±8.85 123.29±9.56 127.39±8.83 4.545 6b 3.635 8b
2.2典型病例

图3 术前检查Fig 3 Preoperative examination

图4 术中检查Fig 4 Intraoperative examination
图5 术后检查Fig 5 Postoperative examination
3 讨论
3.1FRⅢ型矫治器的改良
与传统FRⅢ型矫治器比较,FRⅢ型矫治器作了以下4点改良:1)上颌两侧唇挡与颊屏之间的连接改为“U”型曲,对上颌发育不足较明显的病例,在治疗过程中,随着上齿槽向前的发育,唇档与齿槽逐渐贴近时需要将上唇档适当前移以增加对上颌生长的刺激[9]。此时,只需要在椅旁调节曲即可达到前伸,操作简便,省时。2)舌肌是平衡牙弓内外力量的重要肌群,Ⅲ类错患者的舌位置较低[10-11],在下颌与前腭弓相对应的位置设计一根与前腭弓形状相同的前舌弓,舌弓要求离开下颌前牙5 mm以上,不与其接触,设计下前舌弓的目的是诱导舌在静止状态下的姿势位,使舌在休息位时后退,改变其靠前的状态。3)颊屏内凹状改为外凸状,颊屏的上颌部分与上齿槽间有3 mm的间隙,可以消除颊肌对上颌侧方的压力而使其扩展。颊屏与下齿槽相贴合,颊肌压力可以传达到下颌而抑制其生长。改颊屏内凹状为外凸状,使其能更好地对抗颊肌,增加颊肌张力,加大颊屏牵拉前庭沟处骨膜的力量,更好地刺激该部牙槽骨的生长。4)研究发现,Ⅲ类错患者的舌尖较为靠前[12],舌的长度明显偏短[13]。在上颌软硬腭交界中份加一个能前后旋转的小球,嘱患者不断地舔使之旋转,此时的舌处于后退位,旨在诱导舌在运动状态下的姿势位,弱化舌对下前牙的作用力,舌的后退有利于建立正常牙齿接触的吞咽,反复的训练使其恢复正常位置。
3.2.1在垂直向的变化在垂直向,线距测量结果显示, H-FH、H-S比矫治前增大(P<0.01),说明矫治器改变了Ⅲ类错患者相对升高、靠前的舌骨位置,限制了过度发育的下颌及舌骨上肌群对舌骨的牵拉而下降,这与以前的研究结果相同。所不同的是,矫治后,H-MP较矫治前的位置明显变小(P<0.01),说明矫治后低平的舌骨位置发生了明显地上移。与传统FRⅢ型矫治器矫治后的儿童功能性安氏Ⅲ类错患者的舌骨位置比较,H-FH、H-S增大(P<0.05),H-MP减小(P<0.05),说明舌肌功能训练装置对舌骨位置的影响优于传统矫治器。
3.3改良型FRⅢ型功能矫治器对舌骨位置的影响
在前期的研究中,H-MP、H-RGn是没有改变的(P>0.05),Ar-H-Me角度是变小的(P<0.05),认为矫治后Ⅲ类错患者的舌骨位置的后下移位,是伴随着下颌骨的后下旋转而位移。本研究H-MP减小(P<0.01)、H-RGn减小(P<0.05),Ar-H-Me增大(P<0.01),说明矫治器的改良,使下颌发生后下位移的同时,更有效地促进了舌骨位置的后上移位,这种改变证明舌骨位置与Ⅲ类错有关,其舌骨向前、上的位移是造成其错的原因之一,下颌骨矢状位置的不同导致了舌骨位置的差异,而改变发育中的安氏Ⅲ类错位置低平靠前的舌的位置,可以矫正错矢状位面型。这为进一步探讨安氏Ⅲ类错与舌骨位置及方向的关系,设计独立于FRⅢ型矫治器以外的舌功能训练矫治器,来预防和治疗儿童功能性安氏Ⅲ类错畸形提供了有效证据。改良型FRⅢ型矫治器对于功能性安氏Ⅲ类错的影响及治疗效果的长期稳定性,有待于进一步的临床随机对照研究。
[1] Miethke RR, Lindenau S, Dietrich K. The effect of Fränkel's function regulator type Ⅲ on the apical base[J]. Eur J Orthod,2003, 25(3):311-318.
[2]朱远平, 彭友俭, 张渝宁, 等. FRⅢ型矫治器矫治安氏Ⅲ类错后舌骨位置的对比研究[J]. 实用口腔医学杂志,2011, 27(2):239-242. Zhu YP, Peng YJ, Zhang YN, et al. The position of hyoid bone after treatment of class Ⅲ malocclusion with FRⅢappliance in children[J]. J Pract Stomatol, 2011, 27(2):239-242.
[3] Hägg U, Pancherz H. Dentofacial orthopaedics in relation to chronological age, growth period and skeletal development. An analysis of 72 male patients with Class Ⅱ division 1 malocclusion treated with the Herbst appliance[J]. Eur J Orthod, 1988, 10(3):169-176.
[4] 朱远平. 口腔功能调节器: 中国, ZL201420344457.X[P]. 2014-12-10. Zhu YP. Oral function regulator: China, ZL201420344457. X[P]. 2014-12-10.
[5] Adamidis IP, Spyropoulos MN. Hyoid bone position and orientation in ClassⅠ and Class Ⅲ malocclusions[J]. Am J Orthod Dentofacial Orthop, 1992, 101(4):308-312.
[6] 王宏伟, 齐素青, 王建国, 等. 下颌后退术后舌骨、舌体位置和咽腔间隙变化的锥形束CT分析[J]. 华西口腔医学杂志, 2012, 30(6):650-654. Wang HW, Qi SQ, Wang JG, et al. Detection to changes in hyoid and tongue positions, and pharyngeal airway following mandibular setback surgery by cone beam CT[J]. West Chin J Stomatol, 2012, 30(6):650-654.
[7] Akin M, Ucar FI, Chousein C, et al. Effects of chincup or facemask therapies on the orofacial airway and hyoid position in Class Ⅲ subjects[J]. J Orofac Orthop, 2015, 76(6): 520-530.
[8] Graber LW. Hyoid changes following orthopedic treatment of mandibular prognathism[J]. Angle Orthod, 1978, 48(1): 33-38.
[9] Lee JW, Park KH, Kim SH, et al. Correlation between skeletal changes by maxillary protraction and upper airway dimensions[J]. Angle Orthod, 2011, 81(3):426-432.
[10] Yagci A, Uysal T, Usumez S, et al. Effects of modified and conventional facemask therapies with expansion on dynamic measurement of natural head position in Class Ⅲ patients[J]. Am J Orthod Dentofacial Orthop, 2011, 140(5):e223-e231.
[11] Volk J, Kadivec M, Mušič MM, et al. Three-dimensional ultrasound diagnostics of tongue posture in children with unilateral posterior crossbite[J]. Am J Orthod Dentofacial Orthop, 2010, 138(5):608-612.
[12] Sakata T. A study on the relationship between the position of the hyoid bone in subjects with reversed occlusion and maxillofacial shape in childhood[J]. Nihon Univ Dent J,2001, 75(l):28-37.
[13] Abu Allhaija ES, Al-Khateeb SN. Uvulo-glosso-pharyngeal dimensions in different anteroposterior skeletal patterns[J]. Angle Orthod, 2005, 75(6):1012-1018.
[14] 朱远平, 彭友俭. 安氏Ⅲ类错与舌骨位置关系的研究进展[J]. 临床口腔医学杂志, 2013, 29(6):380-381. Zhu YP, Peng YJ. Research progress of class Ⅲ malocclusion and hyoid position[J]. J Clin Stomatol, 2013, 29(6): 380-381.
[15] Jamilian A, Showkatbakhsh R, Boushehry MB. The effect of tongue appliance on the nasomaxillary complex in growing cleft lip and palate patients[J]. J Indian Soc Pedod Prev Dent,2006, 24(3):136-139.
(本文编辑杜冰)
Comparing study on the hyoid bone position after treatment of class Ⅲ malocclusion using improved appliance FR
ⅢZhu Yuanping1, Duan Yinzhong2.(1. Dept. of Stomatology, The Second People's Hospital of Yichang City, The Second People's Hospital ofThree Gorges University, Yichang 443000, China; 2. School of Stomatology, The Fourth Military Medical Uuiversity, Xi'an 710032, China)
Correspondence: Duan Yinzhong, E-mail: duanyz@fmmu.edu.cn.
ObjectiveThis study aims to compare the changes of hyoid bone position before and after treatment of Angle class Ⅲ malocclusion using improved appliance FR Ⅲ. MethodsForty patients with Angle class Ⅲ malocclusion were chosen and divided into two groups, namely, experimental and control. Each group had 20 patients. The young patients in the experimental group were treated using improved appliance FR Ⅲ, whereas those in the control group were treated using classic appliance FR Ⅲ. The hyoid bone position of the two groups were comparatively analyzed using an X-ray film before and after treatment. ResultsCompared with the condition before treatment, the condition after treatment showed that the hyoid bone position of young patients with Angle class Ⅲ malocclusion treated using improved appliance FR Ⅲ, H-FH, H-S, H-Ptm,and Ar-H-Me exhibited an increased angle (P<0.01), whereas the hyoid bone position of those treated using H-MP and H-Gn showed a decreased angle (P<0.01). The hyoid bone position of young patients with Angle class Ⅲ malocclusion treated using classic appliance FR Ⅲ, H-FH, H-S, and H-Ptm had an increased angle (P<0.05). Moreover, the hyoid bone position of those treated using Ar-H-Me had an increased angle (P<0.01), and the hyoid bone position of those treated using H-MP and H-RGn had a decreased angle (P<0.05). ConclusionCompared with the hyoid bone position before treatment, the hyoid bone position after treatment of the young patients with Angle class Ⅲ malocclusion treated using improved appliance FR Ⅲ may move backward and downward, and the mandibular and hyoid bone position may move through clockwise rotation. The mandibular and hyoid bone position of young patients with Angle class Ⅲ malocclusion treated using classic appliance FR Ⅲ obtained a large angle by moving clockwise. The man-dibular bone moves backward and downward, thereby improving the hyoid bone in backward and upward directions. This condition makes a significant difference in treating the hyoid bone position of young patients with functional Angle class Ⅲmalocclusion.
improved appliance FR Ⅲ;Angle class Ⅲ malocclusion;hyoid bone position
R 783.5
A
10.7518/hxkq.2016.04.010
2015-09-29;
2016-05-15
朱远平,副主任医师,学士,E-mail:zky20041@sina.com
段银钟,主任医师,博士,E-mail:duanyz@fmmu.edu.cn