Influence of obesity and bariatric surgery on gastric cancer
2016-08-10AnnaCarolinaBatistaDantasMarcoAurelioSantoRobertodeClevaRubensAntnioAissarSallumIvanCecconello
Anna Carolina Batista Dantas, Marco Aurelio Santo, Roberto de Cleva, Rubens Antônio Aissar Sallum, Ivan Cecconello
Influence of obesity and bariatric surgery on gastric cancer
Anna Carolina Batista Dantas, Marco Aurelio Santo, Roberto de Cleva, Rubens Antônio Aissar Sallum, Ivan Cecconello
Department of Digestive Surgery, University of São Paulo School of Medicine, São Paulo-SP 05403-000, Brazil
ABSTRACTEsophageal and gastric cancer (GC) are related to obesity and bariatric surgery. Risk factors, such as gastroesophageal reflux and Helicobacter pylori, must be investigated and treated in obese population. After surgery, GC reports are anecdotal and treatment is not standardized. This review aims to discuss GC related to obesity before and after bariatric surgery.
KEYWORDSObesity; bariatric surgery; stomach neoplasms; esophageal neoplasms
Introduction
Obesity remains an epidemic disease worldwide despite advanced clinical and surgical treatment over the past decades. Morbid obesity increases the risk of several diseases1, including cancer, and can lead to increased morbidity related to cancer treatment2,3.
The relationship between cancer and obesity is known, but whether high body mass index (BMI) significantly affects overall cancer risk or whether intense weight loss postoperatively influences cancer incidence remains unclear. A recent meta-analysis demonstrated reduced cancer risk after bariatric surgery, but conclusion could not be drawn because of the high heterogeneity between studies4. New research programs have focused on investigating proteins related to carcinogenesis that are hyper-expressed in obese patients and disappear after surgical weight loss.
Evidence of obesity as a risk factor for colon, breast,endometrial, and renal cell cancer is increasing5, but different results are obtained related to gastric cancer (GC). A recent meta-analysis by Turati et al.6reviewed 22 studies and found a relative risk (RR) of 2.34 for BMI ≥30 kg/m2for cardia and esophageal adenocarcinoma. The European Prospective Investigation into Cancer and Nutrition conducted a multicenter study that included 23 centers and almost 400,000 patients with 11-year follow-up; this study showed the correlation of the abdominal waist circumference and visceral fat with greater risk to esophagus-gastric junction (EGJ) cancer7.
In this context, we aim to review and discuss obesity and bariatric surgery and its risk factors related to GC.
Obesity as a risk factor for GC
Incidence of GC has decreased over the last decades. However, GC remains the fourth most common cancer worldwide and is usually in an advanced disease when it is diagnosed. This disease is classified into cardia and noncardia cancer, with distinct epidemiological and clinical characteristics and diverse treatment options8.
Even though the relationship between obesity and GC remains controversial, with a recent meta-analysis showing no statistically significant association between obesity and non-cardia GC, data on cardia cancer are suggestive9. A recent prospective study, including more than half a million people within the Me-Can Project10, showed that high BMI is associated with an increased risk for esophageal adenocarcinoma, independently from other metabolic risk factors, such as blood pressure, glucose, cholesterol, and triglycerides.
Risk factors
Helicobacter pylori (H. pylori)
H. pylori is classified a type I carcinogen in humans and a well-established risk factor for GC11. Following the continuity of gastritis, intestinal metaplasia, and dysplasia, H. pylori infection can lead to GC. Few studies have investigated the relationship between obesity and H. pylori infection12,13,and the evidence of obesity as a risk for gastric dysplasia is still poor14. Kim et al.15studied more than 1,000 Korean patients to prove the association between obesity and GC regardless of H. pylori status. Their result showed an increased risk of early gastric cancer in men and gastric dysplasia in women, regardless of H. pylori infection.
Gastroesophageal reflux disease (GERD)
GERD and obesity are frequently related, and the prevalence of symptoms is correlated with high BMI16. Super-obese patients with BMI ≥50 kg/m2exhibit higher prevalence of esophagitis compared with obese patients with BMI <40 kg/m217.
Barrett's esophagus, a premalignant precursor, is also highly associated with obesity; however, given the low incidence of disease progression, obesity markers and predictors have been investigated18,19. Higher level of ghrelin is associated with an increased risk of Barrett's esophagus20. Duggan et al.21proved that increased levels of leptin and insulin resistance in overweight patients are associated with high risk of progression from Barrett's esophagus to EGJ cancer.
The Barrett's and Esophageal Adenocarcinoma Consortium22study showed a positive association between heartburn/regurgitation symptoms and EGJ cancer. With regard to other risk factors, such as age, sex, and cigarette smoking, only BMI showed a different effect on stratified analysis with an increased risk for the obese group.
Inflammatory Factors
Obesity is associated with a low-grade chronic inflammation of white adipose tissue (WAT) that is related to insulin resistance and cardiovascular morbidity23,24. In obese patients, WAT activates the innate immune system and induces secretion of TNF-α and interleukin-625. In vivo and in vitro studies have shown that these cytokines are related to GC, inducing proliferation and inhibiting apoptosis of human GC cell lines26.
Pathological findings
Several surgeons from different countries with high rates of GC, such as Japan, Korea, and Chile, suggested Roux-en-Y gastric bypass (RYGB) with resection of the distal stomach because accessing excluded stomach postoperatively is difficult27,28. Braghetto et al.29performed laparoscopic resectional gastric bypass in 112 obese patients, with 10.7% complication rate and only 2 duodenal stump leakages. Histological study found no GC and gastric dysplasia in only five patients.
Over the last 10 years, sleeve gastrectomy (SG) has gained popularity and provided an opportunity to examine the resected specimen, but no incidental finding of GC was reported. Several studies found high rates of gastritis and H. pylori infection on the pathological study of the resected stomach30,31; however, only case reports have described incidental findings of gastrointestinal stromal tumors (GIST)32,33. Given the scarce incidence of pathological findings, selective microscopic examination is endorsed as a safe and economic option, guided with clinical history and macroscopic examination34.
Pre-operative screening
Current guidelines recommend routine upper gastrointestinal endoscopy (UGE) before bariatric surgery35. As shown in Table 136-48, several studies identified a wide range of findings, such as gastritis, esophagitis, hiatal hernia,and gastric or duodenal ulcers, but no study found incidental GC36-38. Routine UGE has been questioned because most of the findings are clinically irrelevant.
Incidental findings without clinical suspicion can lead to unnecessary and morbid treatments, such as prophylactic gastrectomy for gastric polyposis that revealed as benign lesion42. Fernandes et al.48were the first to address endoscopic findings and surgical complications. In regression analysis, endoscopic ulceration was the only predictor of postoperative complications.
GC after bariatric surgery
Reported cases of GC after bariatric surgery are anecdotal,with low level of evidence, arising between 1 and 10 years postoperatively. A recent meta-analysis showed 18 cases of GC after different bariatric procedures, with a mean diagnosis at 8.6 years and adenocarcinoma representing 83% of the cases (Table 2)49-65.
Pathophysiological mechanism
Using the evidence of gastric stump cancer after Billroth II gastrectomy for peptic ulcer, anatomic changes after bariatric surgery may increase carcinogenic risk66. However, according to tumor location, a different pathophysiological mechanism can be established.
RYGB is still the most common bariatric procedure and has the risk of cancer in the gastric pouch and the excluded stomach. Despite increasing evidence showing that RYGB hasa positive role on GERD, with clinical and endoscopic improvement67-69, recent studies have proven the presence of bile reflux in the pouch; its presence can be related to cancer risk as alkaline reflux is widely accepted as a cause of esophagitis, Barrett's esophagus, and adenocarcinoma70-72.
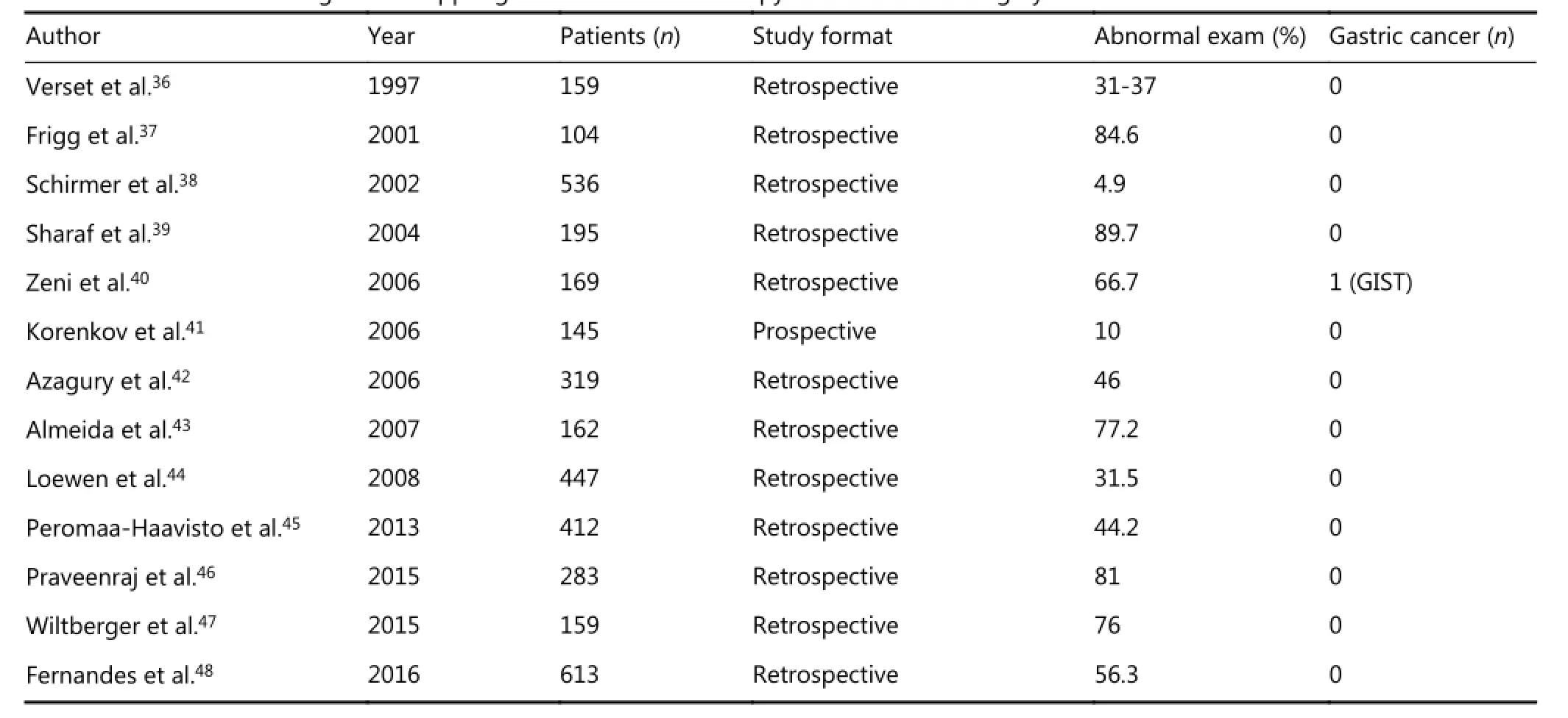
Table 1 Studies addressing routine upper gastrointestinal endoscopy before bariatric surgery
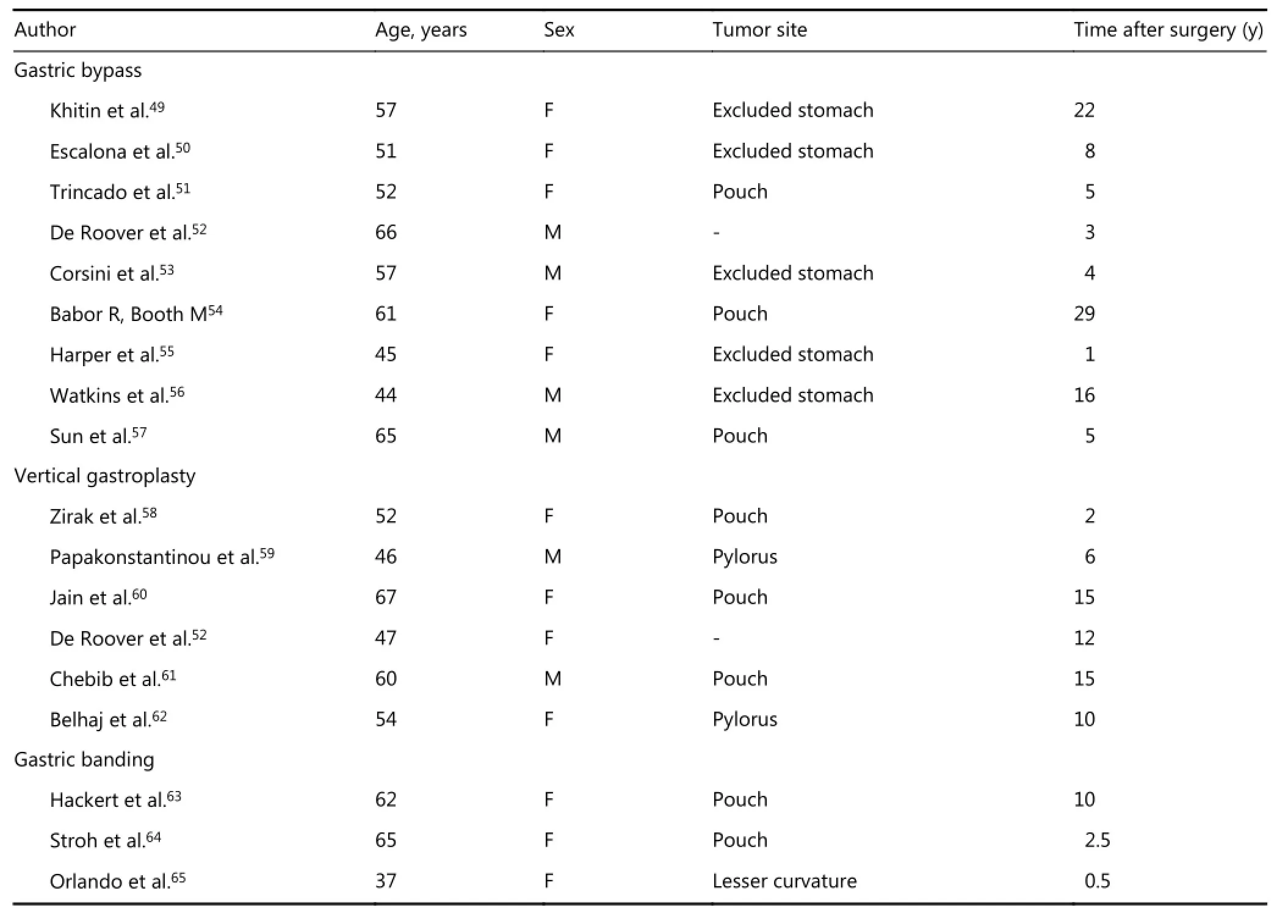
Table 2 Data reported on gastric cancer after bariatric surgery
The excluded stomach has no contact with food and its exogenous carcinogens; thus, pancreaticobiliary reflux may be responsible for cancer risk. Bile reflux in the excluded stomach is well known, and its attributed mucosal changes with atrophy, intestinal metaplasia, and chronic inflammation have been tested in experimental models73. Endoscopic evaluation and cholescintigraphic study found bile in the excluded stomach in 68.6% and 36% of patients,respectively74, 75.
For restrictive procedures, such as gastric banding and SG,the main mechanisms are GERD and its consequent mucosal transformations, food stasis causing chronic inflammation,and local irritation by the band. Previous studies showed that foreign body can lead to local pathological changes76, but evidence also exists that the pressure applied by the gastric band can cause ischemia and metaplastic changes in the mucosa that can progress to malignancy77.
Diagnostic assessment
Given the lack of surveillance program after bariatric surgery,a delay in diagnosis caused by unspecific symptoms is common. The most frequent complaints are dysphagia,nausea, vomiting, abdominal pain, and anemia, which are often attributed by physicians and patients to the effects of the bariatric surgery itself instead of a new disease78.
UGE is the first and most important test if a patient is suspected of GC. This test must be carried out by experienced hands and with great criteria, as well as with photographic documentation and biopsy of any suspected area. If any strictures are observed, obtaining complete dilation is significant to perform complete evaluation of the stomach.
Computed tomography (CT) scan can help to locally access tumor extension and distant metastasis. In the case of RYGB, CT can be used as an initial diagnostic tool because excluded stomach is difficult to evaluate. It has an important role in evaluating gastric distention and greater tumors, but early lesions can be misdiagnosed and biopsy cannot be performed56.
Several authors have reported different and innovative techniques to access the excluded stomach. Virtual gastroscopy was described in 200279and has been performed through percutaneous and noninvasive techniques80. Despite the better image quality of virtual gastroscopy, it has the same limitations to small lesions and histologic evaluation as the CT scan.
Endoscopic evaluation of the excluded stomach is described both via retrograde approach and double-balloon technique. Retrograde endoscopy has long been reported, but failures are frequent due to the angulations of the anastomosis81. Double-balloon endoscopy was first described by Yamamoto et al.82in 2001. This technique can access the excluded stomach even with long limbs and shows high success rate (87.5%), as reported by Safatle-Ribeiro et al.83.
Surgical treatment
Given the unspecific symptoms and difficult diagnostic evaluation, several patients may present with locally advanced (Figure 1) or metastatic disease55. For these patients, multidisciplinary palliative treatment must be provided by surgeons, oncologists, radiotherapists, and nutritionists.
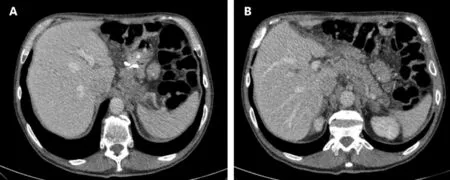
Figure 1 Computed tomography (CT) showing locally advanced gastric pouch cancer. (A) Pouch with silastic ring (B) Remanent stomach.
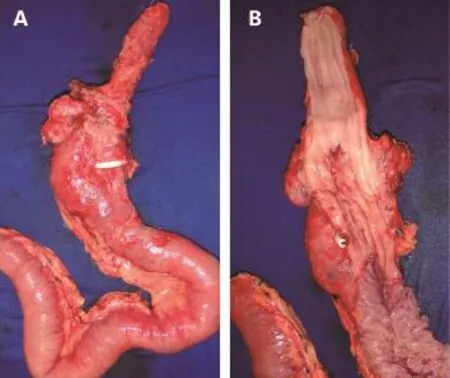
Figure 2 Surgical resection of gastric pouch cancer with subtotal esophagectomy. (A) Oesophagus, gastric pouch and alimentary limb (B) Detail of tumor in gastric pouch.
In cases amenable to surgical treatment, extent of resection is determined by tumor location84. Tumors of the pouch can be treated similarly to EGJ tumors by removing the gastric pouch, esophagus, and regional lymph nodes (Figure 2). In the case of a previous RYGB, the excluded stomach can be used for reconstruction and reach the neck for cervical anastomosis. Care must be taken to preserve the vascular supply of the greater curvature, particularly the right gastric and gastroepiploic arteries. If the bariatric procedure was a SG and the tumor is close to the cardia, a complete resection must be conducted and colon or jejunum can be used for reconstruction.
Neoplasms located in the excluded stomach are treated with total gastrectomy and D2 lymphadenectomy, following the same criteria for margins and extent of resection as GC treatment in general population. Nevertheless, resection of the Roux limb is unnecessary to preserve intestinal length and prevent nutritional complications.
Conclusions
Obesity is a risk factor for several types of cancer, including GC and EGJ. Reports of GC in gastric pouch or excluded stomach are rare, frequently asymptomatic and with incidental diagnosis. During bariatric surgery follow-up, late changes of symptoms, notably dysphagia, should be a warning sign for cancer diagnosis. Cancer treatment is ruled by current concepts, including surgical resection with D2 lymphadenectomy according to location with either gastrectomy of the excluded stomach or esophagectomy and pouch resection.
Conflict of interest statement
No potential conflicts of interest are disclosed.
References
1.Samanic C, Chow WH, Gridley G, Jarvholm B, Fraumeni JF. Relation of body mass index to cancer risk in 362,552 Swedish men. Cancer Causes Control. 2006; 17: 901-9.
2.Parekh N, Chandran U, Bandera EV. Obesity in cancer survival. Annu Rev Nutr. 2012; 32: 311-42.
3.Kaidar-Person O, Bar-Sela G, Person B. The two major epidemics of the twenty-first century: obesity and cancer. Obes Surg. 2011; 21: 1792-7.
4.Casagrande DS, Rosa DD, Umpierre D, Sarmento RA, Rodrigues CG, Schaan BD. Incidence of cancer following bariatric surgery: systematic review and meta-analysis. Obes Surg. 2014; 24: 1499-509.
5.Boeing H. Obesity and cancer-the update 2013. Best Pract Res Clin Endocrinol Metab. 2013; 27: 219-27.
6.Turati F, Tramacere I, La Vecchia C, Negri E. A meta-analysis of body mass index and esophageal and gastric cardia adenocarcinoma. Ann Oncol. 2013; 24: 609-17.
7.Steffen A, Huerta JM, Weiderpass E, Bueno-De-Mesquita HB, May AM, Siersema PD, et al. General and abdominal obesity and risk of esophageal and gastric adenocarcinoma in the European Prospective Investigation into Cancer and Nutrition. Int J Cancer. 2015; 137: 646-57.
8.Rüdiger Siewert J, Feith M, Werner M, Stein HJ. Adenocarcinoma of the esophagogastric junction: results of surgical therapy based on anatomical/topographic classification in 1,002 consecutive patients. Ann Surg. 2000; 232: 353-61.
9.Yang P, Zhou Y, Chen B, Wan HW, Jia GQ, Bai HL, et al. Overweight, obesity and gastric cancer risk: results from a metaanalysis of cohort studies. Eur J Cancer. 2009; 45: 2867-73.
10.Lindkvist B, Johansen D, Stocks T, Concin H, Bjørge T, Almquist M, et al. Metabolic risk factors for esophageal squamous cell carcinoma and adenocarcinoma: a prospective study of 580,000 subjects within the Me-Can project. BMC Cancer.2014; 14: 103.
11.IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Some Industrial Chemicals. IARC Monogr Eval Carcinog Risks Hum.1994; 60: 51-2.
12.Kamada T, Hata J, Kusunoki H, Ito M, Tanaka S, Kawamura Y, et al. Eradication of helicobacter pylori increases the incidence of hyperlipidaemia and obesity in peptic ulcer patients. Dig Liver Dis. 2005; 37: 39-43.
13.Torisu T. Atrophic gastritis, but not antibody to Helicobacter pylori, is associated with body mass index in a Japanese population. J Gastroenterol. 2008; 43: 762-6.
14.Kim HY. Metabolic syndrome is associated with gastric dysplasia. Eur J Gastroenterol Hepatol. 2011; 23: 871-5.
15.Kim HJ, Kim N, Kim HY, Lee HS, Yoon H, Shin CM, et al. Relationship between body mass index and the risk of early gastric cancer and dysplasia regardless of Helicobacter pylori infection. Gastric Cancer. 2014; 18: 762-73.
16.Lagergren J, Bergström R, Lindgren A, Nyrén O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999; 340: 825-31.
17.Santo MA, Quintanilha SR, Mietti CA, Kawamoto FM, Marson AG,de Cleva R. Endoscopic changes related to gastroesophageal reflux disease: comparative study among bariatric surgery patients. Arq Bras Cir Dig. 2015; 28 Suppl 1: 36-8.
18.18.Chang P, Friedenberg F. Obesity and GERD. Gastroenterol Clin North Am 2014;43:161-73.
19.Kamat P, Wen S, Morris J, Anandasabapathy S. Exploring the association between elevated body mass index and Barrett's esophagus: a systematic review and meta-analysis. Ann Thorac Surg. 2009; 87: 655-62.
20.Thomas SJ, Almers L, Schneider J, Graham JE, Havel PJ, Corley DA. Ghrelin and leptin have a complex relationship with risk of barrett's esophagus. Dig Dis Sci. 2016; 61: 70-9.
21.Duggan C, Onstad L, Hardikar S, Blount PL, Reid BJ, Vaughan TL. Association between markers of obesity and progression from Barrett's esophagus to esophageal adenocarcinoma. Clin Gastroenterol Hepatol. 2013; 11: 934-43.
22.Cook MB, Corley DA, Murray LJ, Liao LM, Kamangar F, Ye W, et al. Gastroesophageal reflux in relation to adenocarcinomas of the esophagus: a pooled analysis from the Barrett's and Esophageal Adenocarcinoma Consortium (BEACON) PLoS One. 2014; 9: e103508.
23.Hotamisligil GS, Shargill NS, Spiegelman BM. Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulin resistance. Science. 1993; 259: 87-91.
24.Cottam DR, Mattar SG, Barinas-Mitchell E, Eid G, Kuller L, Kelley DE, et al. The chronic inflammatory hypothesis for the morbidity associated with morbid obesity: implications and effects of weight loss. Obes Surg 2004; 14: 589-600.
25.Bastard JP, Maachi M, Lagathu C, Kim MJ, Caron M, Vidal H, et al. Recent advances in the relationship between obesity, inflammation,and insulin resistance. Eur Cytokine Netw. 2006; 17: 4-12.
26.Alemán JO, Eusebi LH, Ricciardiello L, Patidar K, Sanyal AJ, Holt PR. Mechanisms of obesity-induced gastrointestinal neoplasia. Gastroenterology. 2014; 146: 357-73.
27.Csendes A, Burdiles P, Papapietro K, Diaz JC, Maluenda F, Burgos A, et al. Results of gastric bypass plus resection of the distal excluded gastric segment in patients with morbid obesity. J Gastrointest Surg. 2005; 9: 121-31.
28.Kasama K, Tagaya N, Kanehira E, Oshiro T, Seki Y, Kinouchi M, et al. Laparoscopic sleeve gastrectomy with duodenojejunal bypass: technique and preliminary results. Obes Surg. 2009; 19: 1341-5.
29.Braghetto I, Csendes A, Korn O, Gutierrez L, Brunet L, Lanzarini E,et al. Laparoscopic resectional gastric bypass in patients with morbid obesity: experience on 112 consecutive patients. J Gastrointest Surg. 2011; 15: 71-80.
30.Almazeedi S, Al-Sabah S, Al-Mulla A, Al-Murad A, Al-Mossawi A,Al-Enezi K, et al. Gastric histopathologies in patients undergoing laparoscopic sleeve gastrectomies. Obes Surg. 2013; 23: 314-9.
31.Albawardi A, Almarzooqi S, Torab FC. Helicobacter pylori in sleeve gastrectomies: prevalence and rate of complications. Int J Clin Exp Med. 2013; 6: 140-3.
32.Beltran MA, Pujado B, Méndez PE, Gonzáles FJ, Margulis DI,Contreras MA, et al. Gastric gastrointestinal stromal tumor (GIST)incidentally found and resected during laparoscopic sleeve gastrectomy. Obes Surg. 2010; 20: 393-6.
33.Yuval JB, Khalaileh A, Abu-Gazala M, Shachar Y, Keidar A, Mintz Y, et al. The true incidence of gastric GIST-a study based on morbidly obese patients undergoing sleeve gastrectomy. Obes Surg. 2014; 24: 2134-7.
34.Abdullgaffar B, Raman L, Khamas A, Albadri F. Should we abandon routine microscopic examination in bariatric sleeve gastrectomy specimens? Obes Surg. 2016; 26: 105-10.
35.American Societyfor Gastrointestinal Endoscopy Standards of Practice Committee, Evans JA, Muthusamy VR, Acosta RD,Bruining DH, Chandrasekhara V, et al. The role of endoscopy in the bariatric surgery patient. Gastrointest Endosc. 2015; 81: 1063-72.
36.Verset D, Houben JJ, Gay F, Elcheroth J, Bourgeois V, Van Gossum A. The place of upper gastrointestinal tract endoscopy before and after vertical banded gastroplasty for morbid obesity. Dig Dis Sci. 1997; 42: 2333-7.
37.Frigg A, Peterli R, Zynamon A, Lang C, Tondelli P. Radiologic and endoscopic evaluation for laparoscopic adjustable gastric banding: preoperative and follow-up. Obes Surg. 2001; 11: 594-9.
38.Schirmer B, Erenoglu C, Miller A. Flexible endoscopy in the management of patients undergoing Roux-en-Y gastric bypass. Obes Surg. 2002; 12: 634-8.
39.Sharaf RN, Weinshel EH, Bini EJ, Rosenberg J, Sherman A, Ren CJ. Endoscopy plays an important preoperative role in bariatric surgery. Obes Surg. 2004; 14: 1367-72.
40.Zeni TM, Frantzides CT, Mahr C, Denham EW, Meiselman M,Goldberg MJ, et al. Value of preoperative upper endoscopy in patients undergoing laparoscopic gastric bypass. Obes Surg. 2006;16: 142-6.
41.Korenkov M, Sauerland S, Shah S, Junginger T. Is routine preoperative upper endoscopy in gastric banding patients really necessary? Obes Surg. 2006; 16: 45-7.
42.Azagury D, Dumonceau JM, Morel P, Chassot G, Huber O. Preoperative work-up in asymptomatic patients undergoing Rouxen-Y gastric bypass: is endoscopy mandatory? Obes Surg. 2006; 16: 1304-11.
43.De Moura Almeida A, Cotrim HP, Santos AS, Bitencourt AG,Barbosa DB, Lobo AP, et al. Preoperative upper gastrointestinal endoscopy in obese patients undergoing bariatric surgery: is it necessary? Surg Obes Relat Dis. 2008; 4: 144-9; discussion 150-1.
44.Loewen M, Giovanni J, Barba C. Screening endoscopy beforebariatric surgery: a series of 448 patients. Surg Obes Relat Dis. 2008;4: 709-12.
45.Peromaa-Haavisto P, Victorzon M. Is routine preoperative upper GI endoscopy needed prior to gastric bypass? Obes Surg. 2013; 23: 736-9.
46.Praveenraj P, Gomes RM, Kumar S, Senthilnathan P,Parathasarathi R, Rajapandian S, et al. Diagnostic yield and clinical implications of preoperative upper gastrointestinal endoscopy in morbidly obese patients undergoing bariatric surgery. J Laparoendosc Adv Surg Tech A. 2015; 25: 465-9.
47.Wiltberger G, Bucher JN, Schmelzle M, Hoffmeister A, Dietrich A. Preoperative endoscopy and its impact on perioperative management in bariatric surgery. Dig Surg. 2015; 32: 238-42.
48.Fernandes SR, Meireles LC, Carrilho-Ribeiro L, Velosa J. The role of rou.ine upper gastrointestinal endoscopy before bariatric surgery. Obes Surg. 2016 Jan 10 [Epub ahead of print].
49.Khitin L, Roses RE, Birkett DH. Cancer in the gastric remnant after gastric bypass: a case report. Curr Surg. 2004; 60: 521-3.
50.Escalona A, Guzmán S, Ibáñez L, Meneses L, Huete A, Solar A. Gastric cancer after Roux-en-Y gastric bypass. Obes Surg. 2005; 15: 423-7.
51.Trincado MT, Del Olmo JC, García Castaño J, Cuesta C, Blanco JI,Awad S, et al. Gastric pouch carcinoma after gastric bypass for morbid obesity. Obes Surg. 2005; 15: 1215-7.
52.De Roover A, Detry O, De Leval L, Coimbra C, Desaive C, Honoré P, et al. Report of two cases of gastric cancer after bariatric surgery: lymphoma of the bypassed stomach after Roux-en-Y gastric bypass and gastrointestinal stromal tumor (GIST) after vertical banded gastroplasty. Obes Surg. 2006; 16: 928-31.
53.Corsini DA, Simoneti CA, Moreira G, Lima SE, Garrido AB. Cancer in the excluded stomach 4 years after gastric bypass. Obes Surg. 2006; 16: 932-4.
54.Babor R, Booth M. Adenocarcinoma of the gastric pouch 26 years after loop gastric bypass. Obes Surg. 2006; 16: 935-8.
55.Harper JL, Beech D, Tichansky DS, Madan AK. Cancer in the bypassed stomach presenting early after gastric bypass. Obes Surg. 2007; 17: 1268-71.
56.Watkins BJ, Blackmun S, Kuehner ME. Gastric adenocarcinoma after Roux-en-Y gastric bypass: access and evaluation of excluded stomach. Surg Obes Relat Dis. 2007; 3: 644-7.
57.Sun C, Jackson CS, Reeves M, Rendon S. Metastatic adenocarcinoma of the gastric pouch 5 years after Roux-en-Y gastric bypass. Obes Surg. 2008; 18: 345-8.
58.Zirak C, Lemaitre J, Lebrun E, Journé S, Carlier P. Adenocarcinoma of the pouch after silastic ring vertical gastroplasty. Obes Surg. 2002; 12: 693-4.
59.Papakonstantinou A, Moustafellos P, Terzis I, Stratopoulos C,Hadjiyannakis EI. Gastric cancer occurring after vertical banded gastroplasty. Obes Surg. 2002; 12: 118-20.
60.Jain PK, Ray B, Royston CM. Carcinoma in the gastric pouch years after vertical banded gastroplasty. Obes Surg. 2003; 13: 136-7.
61.Chebib I, Beck PL, Church NG, Medlicott SA. Gastric pouch adenocarcinoma and tubular adenoma of the pylorus: a field effect of dysplasia following bariatric surgery. Obes Surg. 2007; 17: 843-6.
62.Belhaj A, Memmo L, Memo L, Mehdi A, Mboti F, Closset J. Gastric adenocarcinoma following "silastic vertical ring gastroplasty": case report. Rev Med Brux. 2010; 31: 459-62.
63.Hackert T, Dietz M, Tjaden C, Sieg A, Buchler MW, Schmidt J. Band erosion with gastric cancer. Obes Surg. 2004; 14: 559-61.
64.Stroh C, Hohmann U, Urban H, Manger T. Gastric cancer after laparoscopic adjustable gastric banding. Obes Surg. 2008; 18: 1200-2.
65.Orlando G, Pilone V, Vitiello A, Gervasi R, Lerose MA, Silecchia G,et al. Gastric cancer following bariatric surgery: a review. Surg Laparosc Endosc Percutan Tech. 2014; 24: 400-5.
66.Macdonald WC, Owen DA. Gastric carcinoma after surgical treatment of peptic ulcer: an analysis of morphologic features and a comparison with cancer in the nonoperated stomach. Cancer. 2001;91: 1732-8.
67.Smith SC, Edwards CB, Goodman GN. Symptomatic and clinical improvement in morbidly obese patients with gastroesophageal reflux disease following Roux-en-Y gastric bypass. Obes Surg. 1997;7: 479-84.
68.Nelson LG, Gonzalez R, Haines K, Gallagher SF, Murr MM. Amelioration of gastroesophageal reflux symptoms following Roux-en-Y gastric bypass for clinically significant obesity. Am Surg. 2005; 71: 950-3; discussion 953-4.
69.Madalosso CA, Gurski RR, Callegari-Jacques SM, Navarini D,Mazzini G, Pereira Mda S. The impact of gastric bypass on gastroesophageal reflux disease in morbidly obese patients. Ann Surg. 2016; 263: 110-6.
70.Hak NG, Mostafa M, Salah T, El-Hemaly M, Haleem M, Abd El-Raouf A, et al. Acid and bile reflux in erosive reflux disease, nonerosive reflux disease and Barrett's esophagus. Hepatogastroenterology. 2008; 55: 442-7.
71.Attwood SE, Demeester TR, Bremner CG, Barlow AP, Hinder RA. Alkaline gastroesophageal reflux: implications in the development of complications in Barrett's columnar-lined lower esophagus. Surgery. 1989; 106: 764-70.
72.Gillen P, Keeling P, Byrne PJ, Healy M, O'moore RR, Hennessy TP. Implication of duodenogastric reflux in the pathogenesis of Barrett's oesophagus. Br J Surg. 1988; 75: 540-3.
73.Cunha Medeiros A, Meneses Rego A, Medeiros Azevedo I, Ferreira Carvalho M, Brasil Medeiros V, Araujo-Filho I. Metabolism and gastric remnant changes after Roux-en-Y gastric bypass in rats. J Invest Surg. 2011; 24: 109-14.
74.Kuga R, Safatle-Ribeiro AV, Faintuch J, Ishida RK, Furuya CK,Garrido AB, et al. Endoscopic findings in the excluded stomach after Roux-en-Y gastric bypass surgery. Arch Surg. 2007; 142: 942-6.
75.Sundbom M, Hedenström H, Gustavsson S. Duodenogastric bile reflux after gastric bypass: a cholescintigraphic study. Dig Dis Sci. 2002; 47: 1891-6.
76.Negri M, Bendet N, Halevy A, Halpern Z, Reif R, Bogokovsky H, et al. Gastric mucosal changes following gastroplasty: a comparative study between vertical banded gastroplasty and silastic ring verticalgastroplasty. Obes Surg. 1995; 5: 383-6.
77.Cariani S, Amenta E. Three-year results of Roux-en-Y gastric bypass-on-vertical banded gastroplasty: an effective and safe procedure which enables endoscopy and X-ray study of the stomach and biliary tract. Obes Surg. 2007; 17: 1312-8.
78.Scozzari G, Trapani R, Toppino M, Morino M. Esophagogastric cancer after bariatric surgery: systematic review of the literature. Surg Obes Relat Dis. 2013; 9: 133-42.
79.Silecchia G, Catalano C, Gentileschi P, Elmore U, Restuccia A,Gagner M, et al. Virtual gastroduodenoscopy: a new look at the bypassed stomach and duodenum after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Obes Surg. 2002; 12: 39-48.
80.Alva S, Eisenberg D, Duffy A, Roberts K, Israel G, Bell R. A new modality to evaluate the gastric remnant after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2008; 4: 46-9; discussion 49.
81.Sinar DR, Flickinger EG, Park HK, Sloss RR. Retrograde endoscopy of the bypassed stomach segment after gastric bypass surgery: unexpected lesions. South Med J. 1985; 78: 255-8.
82.Yamamoto H, Sekine Y, Sato Y, Higashizawa T, Miyata T, Iino S, et al. Total enteroscopy with a nonsurgical steerable double-balloon method. Gastrointest Endosc. 2001; 53: 216-20.
83.Safatle-Ribeiro AV, Kuga R, Iriya K, Ribeiro U, Faintuch J, Ishida RK, et al. What to expect in the excluded stomach mucosa after vertical banded Roux-en-Y gastric bypass for morbid obesity. J Gastrointest Surg. 2007; 11: 133-7.
84.Kuruba R, Jawad M, Karl RC, Murr MM. Technique of resection of esophageal adenocarcinoma after Roux-en-Y gastric bypass and literature review of esophagogastric tumors after bariatric procedures. Surg Obes Relat Dis. 2009; 5: 576-81.
Cite this article as: Dantas ACB, Santo MA, de Cleva R, Sallum RAA,Cecconello I. Influence of obesity and bariatric surgery on gastric cancer. Cancer Biol Med. 2016; 13: 269-276. doi: 10.20892/j.issn.2095-3941.2016.0011
Correspondence to: Marco Aurelio Santo
E-mail: santomarco@uol.com.br
Received January 22, 2016; accepted February 16, 2016. Available at www.cancerbiomed.org
Copyright © 2016 by Cancer Biology & Medicine
杂志排行
Cancer Biology & Medicine的其它文章
- The oncofetal protein IMP3 is an indicator of early recurrence and poor outcome in mucoepidermoid carcinoma of salivary glands
- Modulation of B-cell receptor and microenvironment signaling by a guanine exchange factor in B-cell malignancies
- Characterization of FGFR signaling pathway as therapeutic targets for sarcoma patients
- Bone marrow niche-mediated survival of leukemia stem cells in acute myeloid leukemia: Yin and Yang
- Genetic and molecular changes in ovarian cancer
- New generation of breast cancer clinical trials implementing molecular profiling