Screening of developmental dysplasia of the hip in infants and young children in hospital
2016-08-05LIUQiuliangWANGYishengLIUYufengZHANGMengzhenGAOJianboCHANGJianminTIANPeichaoZHANGYonggaoHEXiaoCHENXinrangWANGJiaxiangQINPanFANYingzhongGAOJingyaoWANGQiSHILongyanZHANGJiao
LIU Qiu-liang, WANG Yi-sheng, LIU Yu-feng, ZHANG Meng-zhen, GAO Jian-bo, CHANG Jian-min, TIAN Peichao, ZHANG Yong-gao, HE Xiao, CHEN Xin-rang, WANG Jia-xiang, QIN Pan, FAN Ying-zhong, GAO Jing-yao,WANG Qi, SHI Long-yan, ZHANG Jiao
. 髋关节发育不良 Dysplasia of hip joint .
Screening of developmental dysplasia of the hip in infants and young children in hospital
LIU Qiu-liang, WANG Yi-sheng, LIU Yu-feng, ZHANG Meng-zhen, GAO Jian-bo, CHANG Jian-min, TIAN Peichao, ZHANG Yong-gao, HE Xiao, CHEN Xin-rang, WANG Jia-xiang, QIN Pan, FAN Ying-zhong, GAO Jing-yao,WANG Qi, SHI Long-yan, ZHANG Jiao
Funding Disclosure: Provincial Joint Project by the National Health and Family Planning Commission with Henan Province Health and Family Planning Commission (201401007); the Scientific and Technological Key Project by Zhengzhou Science and Technology Bureau (131PPTGG409-23)
Authoraddress: 450052, Henanprovince, the First Affliated Hospital of Zhengzhou University, Pediatric Surgery (LIU Qiu-liang,CHEN Xin-rang, WANG Jia-xiang, QIN Pan, FAN Ying-zhong, GAO Jing-yao, WANG Qi, SHI Long-yan, ZHANG Jiao), Department of Orthopaedics (WANG Yi-sheng), Paediatrics (LIU Yu-feng, TIAN Pei-chao), Obstetrics Department (ZHANG Meng-zhen), Radiology Department (GAO Jian-bo, ZHANG Yong-gao), Hypersound Department (CHANG Jian-min, HE Xiao)
Objective To summarizethe status of screening of developmental dysplasia of the hip (DDH)in infants and young children 0 - 36 months of age and to generate a standardized process for DDH screening in infants and young children. Methods Preliminary DDH screening was carried out by obstetricians for newborns, and by pediatricians for infants and young children 0 - 36 months inpatients in ward, and by pediatric surgeon for infants and young children 0 - 36 months of age outpatient. Secondary screening was performed by pediatric orthopedic surgeons. In addition, ultrasound or radiograph examination of bilateral hip joints was performed. Suspected cases were followed up regularly until patients were diagnosed with DDH or excluded. Results From January 2012 to December 2014,22 396 infants and young children were screened at the First Affliated Hospital of Zhengzhou University, Zhengzhou,China. Ultrasound examination was performed for 2669 patients, 591 of whom (775 hips) with suspected and abnormal fndings were transferred to the Department of Pediatric Orthopedics. Among the referrals, a positive Ortolani or Barlow test was observed in 61 patients (89 hips). Anteroposterior hip radiography showed acetabular dysplasia in 94 cases (131 hips). Finally, 76 patients (121 hips) were diagnosed with DDH. Among them, 21 (29 hips)were males and 55 (92 hips) were females. The left side was involved in 91 hips, and the right side was involved in 30 hips. Thirteen cases (including 3 newborns) were 1 - 6 months old (1.95‰, 13 / 6676), 49 cases were 7 - 18 months old (7.09‰, 49 / 6909), and 14 cases were 19 - 36 months old (1.59‰, 14 / 8811). Among the 76 cases of DDH,49 (64.47%) were 7 - 18 months old. The incidence of hip dysplasia was 3.39‰ (76 / 22 396). Conclusions During the present study, we screened infants and young children 0 - 36 months old for early detection and diagnosis of DDH and generated a standardized screening process based on the actual status of patients in our district.
Hip join; Hip dislocation, developmental; Neonatal screening; Infant; Child pre (2 - 5);Mass screening; Hip dysplasia
Developmental dysplasia of the hip (DDH) is common in children. Early diagnosis is the key toeffective treatment of DDH, and, to these ends, early screening is necessary for early diagnosis. Recently, we have developed a DDH screening team in the First Affiliated Hospital of Zhengzhou University to identify DDH in infants and young children and gradually have established a standardized process for DDH screening. Here we report about the development of this DDH screening program and its components so our program can be duplicated and refned at additional hospitals in China and elsewhere. In addition, we offer suggestions about coordination of care and healthcare delivery systems that incorporate DDH screening as part of the standard of care.
Data and Methods
Patients
All neonates born in the Obstetrical Department and all infants and young children (0 - 36 months of age) who visited the Outpatient Department or were admitted to the Department of Pediatrics of the First Affiliated Hospital of Zhengzhou University between January 2012 and December 2014 were screened for DDH. Age was determined in “months”as follows: Newborns were taken as 0 month, and infants and young children more than 1 month old were recorded according to the actual number of months of lifebased on the date of birth; if the date of birth occurred before the 15th of the birth month, the child's age was considered to be less than one month, and if the date of birth was after the 15th day, the infant's age was considered to be more than one month. During the 2 initial years of the program, 22 396 infants and young children were screened. The average age was (11.7 ± 4.7) months;6676 patients were6 months old, 6909 were 7 -18 months old, and 8811 were1836 months old. This group included 12 017 males and 10 379 females. Screening Process
Figure 1 illustratesthe screening process to identify DDH in infants and young children.
Training Screeners
All staff participating in the screening process received theoretical study and hands-ontraining to ensure the use of standard procedures and manipulations involved in DDH screening. All staff were allowed to participate in the research only after on-site manipulation, training, and passing the examination.
Screening Device
A Hitachi HIVISIONPreirus Ultrasound systemwith an 8.0-MHz linear array transducer was used in the present study.
DDH Screening Protocol[1-5]
General examination Each patient's developmental history, including presentation, sex, family history relevant to DDH, was recorded.
Physical signs Patients' physical signs were examined and recorded, including symmetries of bilateral medial dermatoglyphs in the thigh and bilateral gluteal folds; symmetry of the hip; general consistency of length and thickness of bilateral lower extremities;and characteristics of hip joint motion, including bilateral hip flexion, extension, abduction, adduction, external rotation, and internal rotation angles.
Special signs The Allis sign of the bilateral lower extremities (also known as the Galeazzi Test), the hip abduction test, the Ortolani or Barlow Test, the TrendelenburgTest, and walking gait were tested and recorded according to our standardized protocol.
Detection of related complications Physicians or staff checked patients for the presence of muscular torticollis, spinal deformities, congenital heart diseases (based on ultrasound findings after birth), urinary tract abnormalities, foot deformities, calcaneal valgus,and metatarsus adductus. All this malformation was diagnosed by correlative pediatric surgeon.
Ultrasound Examination of Bilateral Hip Joints[1-4]
Graf ultrasound examination
For infants less than 6 months old, we performed a Graf ultrasound examination. The infant was placed in the lateral decubitus position, and the lower extremity to be examined was fexed naturally and pronated slightly. The probe was placed over the greater trochanter of the lower limb to be examined. The probe was placed parallel to the long axis of the body. Measurement data included the following: (1) baseline: the tangent line of the ilium at the junction between the periosteum and perichondrium; (2) bone roof line: the tangent line of the acetabular roof at the inferior margin of the ilium inside the acetabulum;the angle between the baseline and the bone roof line was defned as α; (3) cartilage roof line: the line connecting the turning point of the acetabular roof margin and the center of the cartilage labrum. The angle between the cartilage roof line and the baseline was defned as β. Based on the Graf standard,we classified each hip into normal (I), suspicious (II a), or abnormal (II b, II c, D, III, and IV) types.
Radiographic Examination of the Pelvis
For infants and young children more than 6 months old, an anteroposterior pelvic radiograph was taken. The infants and young children were placed in the supine position (10% 0.5 ml / kg chloral hydrate wasgiven orally for those who could not lie down quietly). The bilateral lower limbs were kept straight with upright bilateral patellas. When performing radiographic examination, staff members shielded the patient's perineum. The hip joint was flexed to about 30° (for stability and to ensure the correct angle, the operator placed a thin wood block beneath the thigh). The presence of acetabular dysplasia, if any, was observed. The anteroposterior radiograph of bilateral hip joints was taken at 40° of internal rotation and 35° of abduction so staff could observe the status of the acetabulum covering the femoral head.
Standard of Defnite Diagnosis[1-5]
Infants and young children were examined for inclusion or exclusion in the DDH cohort by pediatric orthopedic surgeons who examined the data mentioned above. According to Terjesen's standard, an acetabular index of32° in infants 1 - 11 months old was considered to beacetabular dysplasia. Infants and young children with limited abduction of the hip (positive),a positive Barlow or OrtolaniTest, or type II b - IV hips determined by ultrasound examination were diagnosed with DDH. Some were diagnosed after radiographic examination of the hip.
Results
Ultrasound screening of the hip joint was performed for 2699 cases, and 591 cases (755 hips)with suspicious or abnormal fndings were transferred to the Department of Pediatric Orthopedics. The Ortolani or Barlow Test was positive in 61 cases (89 hips) among the suspected cases, and the anteroposterior radiograph showed acetabular dysplasia in 94 cases (131 hips). Finally, 76 cases (121 hips) were diagnosed with DDH. The mean age was (12.8 ± 4.3) months, and patients included 21 males (29 hips) and 55 females (92 hips). The left side was involved in 91 hips, and the right side was involved in 30 hips. Thirteen cases (including 3 newborns) were 1 - 6 months old (1.95‰, 13 / 6676),49 cases were 7 - 18 months old (7.09‰, 49 / 6909),and 14 cases were 19 - 36 months old (1.59‰, 14 / 8811). The incidence of DDH was 3.39‰ (76 / 22 396). Among the 76 cases diagnosed with DDH, 49 cases(64.47%) were 7 - 18 months old. Among DDH patients,17 cases had associated foot deformities, 12 had congenital heart diseases, 5 had calcaneal eversion (8 feet), 7 had spinal deformities, 8 had muscular torticollis, 4 had urinary tract abnormalities, and 2 had metatarsus adductus.
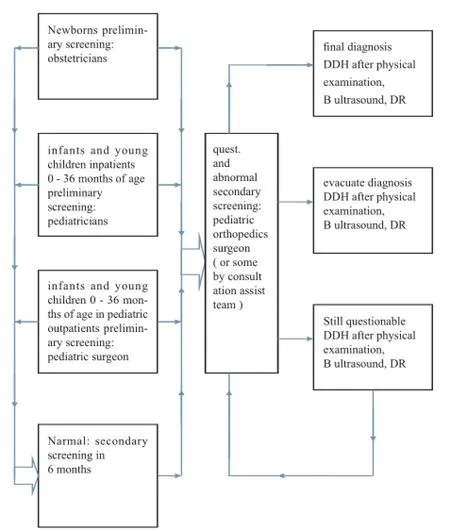
Fig.1 DDH screening fuidogram in infant and young children
Discussion
Early screening, early detection, and early intervention to treat DDH in infants and young children have become the consensus strategies of most physicians[1,6-9]. All young children are included for screening in some areas, butonly high-risk populations are screened in some other areas. In China, most areas carry out universal screening for DDH for all infants and young children. In some cities such as Beijing, Tianjin,and others, the detection of DDH is included in the government-run health care system for children. Other areas also carry out early screening of DDH using their own methods[1,10].
Various national and regional districts have established different agesat which early screening should begin. For example, countries such as Germany and Austria start screening within 72 hours after birthand 6 - 8 weeks after birth, respectively. In China, early screening is often performed 6 weeks after birth (at the time of health checkup and vaccination) to avoid overdiagnosis, over-treatment, and iatrogenic complications such as femoral head necrosis[1,2,8,11]. Some physician scholars also recommend screening 6 - 8 weeks after birth[12]. In the present study, we carried out screening of newborns immediately after birth. Based on the principle of DDH diagnosis and treatment, early diagnosis and intervention can reduce the rate of surgery and achieve satisfactory long-term outcomes. However,national systems and requirements in China favor early screening 6 weeks after birth.
Graf[13]initially applied ultrasound examination in the diagnosis of DDH in neonates and proposed and improved the standards for ultrasound classification during DDH screening. Thereafter, ultrasound screening of DDH for neonates and infants has beenwildly used in the world and has gradually become the gold standard of early imaging diagnosis of DDH and the primary means of early screening. Subsequent clinical practices have proved that this method is simple, safe, economical, and effective[14]. Some clinicians consider that the method of DDH screening should be improved and updated;for example, the distance between the proximal femur and the pubic bone should be measured, the depth of acetabulum on the coronal plane should also be measured, and ultrasound examination should be carried out only for cases with high-risk factors of DDH or following abnormal fndings during a health checkup[15].
The results of our screening showed that the incidence of DDH was 3.39‰, which is slightly higher than that of other areas in China but is similar to that of other Asian countries. The possible reason is that in the present study the number of patients who visited the outpatient department for pediatric orthopedics was relatively high, and we did not perform DDH screening for all infants and young children in our area. The youngest DDH child was 1 month (the actual age was 3 days), the oldest child was 36 months, and the mean age was (12.8 ± 4.3) months, which is an older cohort compared to that in other studies. The possible reason is that the range of subjects included in our screening was wider. In the present study, females were 2.6 times more likely to have DDH compared to males, the left hip was 3.0 times more likely to be affected compared to the right hip, and these resultsare consistent with other reports. Two out of 76 DDH cases had a history of legs being tied after birth. The results of our screening also showed that asymmetry in the medial dermatoglyphs in the thigh and gluteal folds is an important clue during DDH screening, and the symptoms of the lower extremities, female sex, family history of DDH, and breech birth are independent factors associated with a higher risk for DDH[16-17].
During the process of screening, we found that it was very important to carry out physical examination of the lower extremities and hip joints skillfully and normally, and ultrasound examination is a necessary complement. During health checkup, lighting should be optimal and the environment should be quiet, the parents should be informed sufficiently and cooperate actively during the whole process, the fnancial burden should be decreased, the expectations and concerns of parents should be understood, and repeated examination can reduce false negative and false positive rates. The staff should help parents understand that ultrasound examination of the hip joints is a routine component of the health checkup and is not prompted by the suspicion of disease--these social and environmental cues will help parents participate in DDH screening more conscientiously[4,11].
DDH screening is often carried out actively by local public health agencies during vaccination and health checkups for females and infants, but newborns and infants are usually screened in various hospitals. At present, pediatric orthopedic staff are the main caregivers for early DDH screening and treatment in China. However, they are often over burdened even before they are challenged to carry out such a large amount of work, and it is impossible for pediatric orthopedic staff alone to perform early DDH screening for all infants and young children. We believe that early DDH screening should be carried out during government-guided vaccinations and health checkup sconducted by local public health agencies.
Because we operatea general hospital, our early DDH screening depends on the staff in the Obstetrics andPediatrics Departments. Since 2010, we have performed DDH screening for all infants and children younger than 36 months. Among 76 DDH patients, 49 (64.47%)were 7 - 18 months old.
In the beginning of our study, the processes and plans were developed mainly for the Department of Pediatric Orthopedics. However, the workload of staff in this department was almost overwhelming,and we adjusted our approach so that only patients with suspected or abnormal findings during primary screening were selected for the secondary screening by the staff in the Department of Pediatric Orthopedics. Other departments were involved in the screening independently but also closely connected to the Department of Pediatric Orthopedics. In this manner, the range of screening was ensured, and even an absolutely normal child could be screened twice. This reduced the possibilities of misdiagnosis and missed diagnosis and also put the Department of Pediatric Orthopedics in an important position. During our research, we continuously adjusted and standardized the process, trained and examined the staff who participated in the screening, and arranged consultations for patients with unclear diagnosis in order to establish a satisfactory screening process (Fig.1). This process ensured smooth progress during the current study and improved the fnal results.
Our screening was carried out strictly according to the predifined process, and standard screening was performed for infants and young children to establish a screening process suitable to our district. The process displays the advantages of collaboration between various departments in a general hospital. However, it should be further amended and supplemented.
Reference
[1] YANG Jian-ping. Diagnosis, therapy and early screening of developmental dysplasia of the hip. Chin J Pediatric Surg,2016, 37(1):1-2.
[2] DI Yao-zong, YANG Jian-ping, WANG Wen-wen, et al. Early screening of developmental dysplasia of the hip in Tianjin. Chin J Orthop, 2011, 31(5):463-468.
[3] SHEN Pin-quan, CHEN Bo-chang, LU Mei-ling, et al. Ultrasound screening for developmental dysplasia of the hip in 720 infants. Chin J Pediatric Surg, 2007, 28(4):190-192.
[4] JI Shi-jun, MA Rui-xue, LIU Wei-dong. Try torealize the screening and protect. Chin J Pediatric Surg, 2003, 24(3): 199-200.
[5] YANG Jian-ping, DI Yao-zong. Preliminary result and realize of early screeningof developmental dysplasia of the hipinTianjin. Shandong Med J, 2011, 51(24):4-5.
[6] Sink EL, Ricciardi BF, Torre KD, et al. Selective ultrasound screening is inadequate toidentify patients who present with symptomaticadult acetabular dysplasia. J Child Orthop, 2014,8(6):451-455.
[7] Shipman SA, Helfand M, Moyer VA, et al. Screening for developmental dysplasia of the hip: a systematic literaturereview for the US Preventive Services Task Force. Pediatrics,2006, 117(3):e557-576.
[8] de Hundt M, Vlemmix F, Bais JM, et al. Risk factors for developmental dysplasia ofthe hip: a meta-analysis. Eur J Obstet Gynecol Reprod Biol, 2012, 165(1):8-17.
[9] Stevenson DA, Mineau G, Kerber RA, et al. Familial predisposition to developmental dysplasia of the hip. J Pediatr Orthop, 2009, 29(5):463-466.
[10] LIU Qiu-liang, WANG Yi-sheng, LIU Yu-feng, et al. Early screening of developmental dysplasia of the hip among hospitalized children. Natl. Med J China, 2014, 94(20): 1567-1569.
[11] Ortiz-Neira CL, Paolucci EO, Donnon T. A meta-analysis of common risk factors associated with the diagnosis of developmental dysplasia of the hip in newborns. Eur J Radiol,2012, 81(3):e344-351.
[12] Kolb A, Schweiger N, Mailath-Pokorny M, et al. Low incidence of early developmental dysplasia of the hip in universal ultrasonographic screening of newborns: analysis and evaluation of risk factors. Int Orthop, 2016, 40(1):123-127.
[13] Sanghrajka AP, Murnaghan CF, Shekkeris A, et al. Open reduction for developmental dysplasia of the hip: failures of screening or failures of treatment? Ann R Coll Surg Engl,2013, 95(2):113-117.
[14] Tréguier C, Chapuis M, Branger B, et al. Pubo-femoral distance: an easy sonographic screening test to avoid late diagnosis of developmental dysplasia of the hip. Eur Radiol,2013, 23(3):836-844.
[15] Witting M, Boere-Boonekamp MM, Fleuren MA, et al. Determinants of parental satisfaction with ultrasound hip screening in child health care. J Child Health Care, 2012, 16(2): 178-189.
[16] Price KR, Dove R, Hunter JB. The use of X-ray at 5 months in a selective screening programme for developmental dysplasia of the hip. J Child Orthop, 2011, 5(3):195-200.
[17] Graf R. Hip sonography: 20 years experience and results. Hip Int, 2007, 17(Suppl 5):S8-14.
(本文编辑:李贵存)
Acknowledgments: The authors thank Professor SUN Lin from Beijing Children's Hospital Pediatric Orthopedics Department,Professor YANG Jian-ping from Tianjin Hospital Pediatric Orthopedics and Professor YAN Gui-shen from Beijing Jishuitan Hospital Pediatric Orthopedics Department-these individuals provided suggestions and assistance during the screening and implementation processes.
10.3969/j.issn.2095-252X.2016.07.003中图分类号:R681
2016-05-16)
