微栓子监测在脑干梗死和椎基底动脉狭窄中的作用
2016-06-28荣艳红赵琨苏红军齐金龙
荣艳红,赵琨 ,苏红军,齐金龙
微栓子监测在脑干梗死和椎基底动脉狭窄中的作用
荣艳红,赵琨 ,苏红军,齐金龙
摘要:目的探讨脑干梗死患者微栓子信号(MES)阳性与椎基底动脉狭窄的关系。方法156例急性脑干梗死患者进行头颅核磁共振成像和CT血管造影检查,确定脑梗死病灶及椎基底动脉狭窄情况,并于发病7 d内应用经颅多普勒经枕窗进行基底动脉MES监测,分为MES阴性组136例及阳性组20例。考察2组一般资料及不同狭窄程度;椎基底动脉狭窄患者中2组不同部位情况;Logistic回归分析MES阳性表达的影响因素。结果2组年龄、性别、高血压病史及糖尿病史等差异均无统计学意义;不同狭窄程度的构成差异有统计学意义,阴性组以无或轻度狭窄为主,阳性组以重度狭窄最高(P<0.05)。无椎基底动脉狭窄70例,轻、中及重度狭窄86例均为椎基底动脉狭窄,其中MES阳性者14例,阴性者72例。椎基底动脉狭窄患者的2组在不同狭窄部位差异有统计学意义,阴性组各狭窄部位比例差异不大,而阳性组颅内椎基底动脉狭窄率高于85%(P<0.05),阳性组多部位梗死比例高于阴性组(P<0.05)。颅内椎基底动脉狭窄、椎基底动脉狭窄75%以上为MES阳性的独立危险因素。结论重度狭窄的椎基底动脉更易出现后循环系统的MES,导致脑梗死;微栓子可能是椎基底动脉狭窄出现多部位脑梗死的发病原因。
关键词:脑干梗死;椎基底动脉狭窄;微栓子;经颅多普勒超声
作者单位:天津市宝坻区人民医院神经内科(邮编301800)
1 资料与方法
1.1一般资料选取2012年1月—2013年10月于本院神经内科确诊为脑干梗死的患者156例,符合1995年全国第4届脑血管病学术会议制定的脑梗死诊断标准,采用第9届国际脑血流动力学会议制定的MES识别标准:(1)时间短暂,<300 s。(2)信号强度高于背景血流信号>3 dB。(3)单方向出现于血流频谱中。(4)伴有尖锐哨声或鸟鸣声,均经头颅磁共振成像(MRI)和头颅CT血管造影(CTA)检查确诊。除外不能配合MES监测及MRI等检查者,156例中无溶栓者;男109例,女47例,年龄35~78岁;合并高血压111例、糖尿53例、脑卒中病史35例、心房纤颤2例、吸烟史66例。
1.2方法(1)MES监测。所有患者发病7 d内,采用德国DWL公司的Doooler BOX TCD检测仪,经枕窗进行基底动脉MES监测,监测时间持续30 min,设置MES相对强度阈值>3 dB;患者坐位或侧卧位,监测头架旋转90°,经枕窗监测基底动脉,双深度探头取样深度80~95 mm,容积8 mm。由经过培训的专人负责MES监测,每个MES均经回放确认,并经2名神经科医生同时确认。根据有无监测到MES分为MES阳性组和阴性组。156例中MES阳性组20例(12.8%),阴性组136例(87.2%)。(2)狭窄程度判断。所有患者进行包含磁共振扩散加权成像(DWI)的MRI和CTA检查,DWI检查采用带有标准化头线圈的1.5 T核磁扫描仪(Gyroscan ASC NT, Philips Medical Systems)。用0、313和1 252 s/mm2不同值获得3个基本磁场方向的9个层面。至少在2个DWI中出现高强度信号才能被认为是急性脑梗死。CTA应用美国GE LightSpeed VCT型CT检查,根据管腔狭窄和信号丢失的程度,将椎基底动脉狭窄分成无狭窄、轻度狭窄(<50%)、中度狭窄(50%~75%)及重度狭窄(>75%)。
1.3统计学方法采用SPSS 13.0统计软件包进行数据处理。符合正态分布的计量资料用x ±s表示,2组间均数比较应用t检验。计数资料以例(%)表示,组间比较用χ2检验。多因素分析采用Logistic回归分析。检验水准α=0.05。
2 结果
2.1 2组一般资料及不同狭窄程度结果比较2组性别、年龄、高血压病史及糖尿病史等差异均无统计学意义,见表1。2组不同狭窄程度的构成差异有统计学意义,阴性组以无或轻度狭窄为主,阳性组重度狭窄者比例最高(P<0.05),见表2。
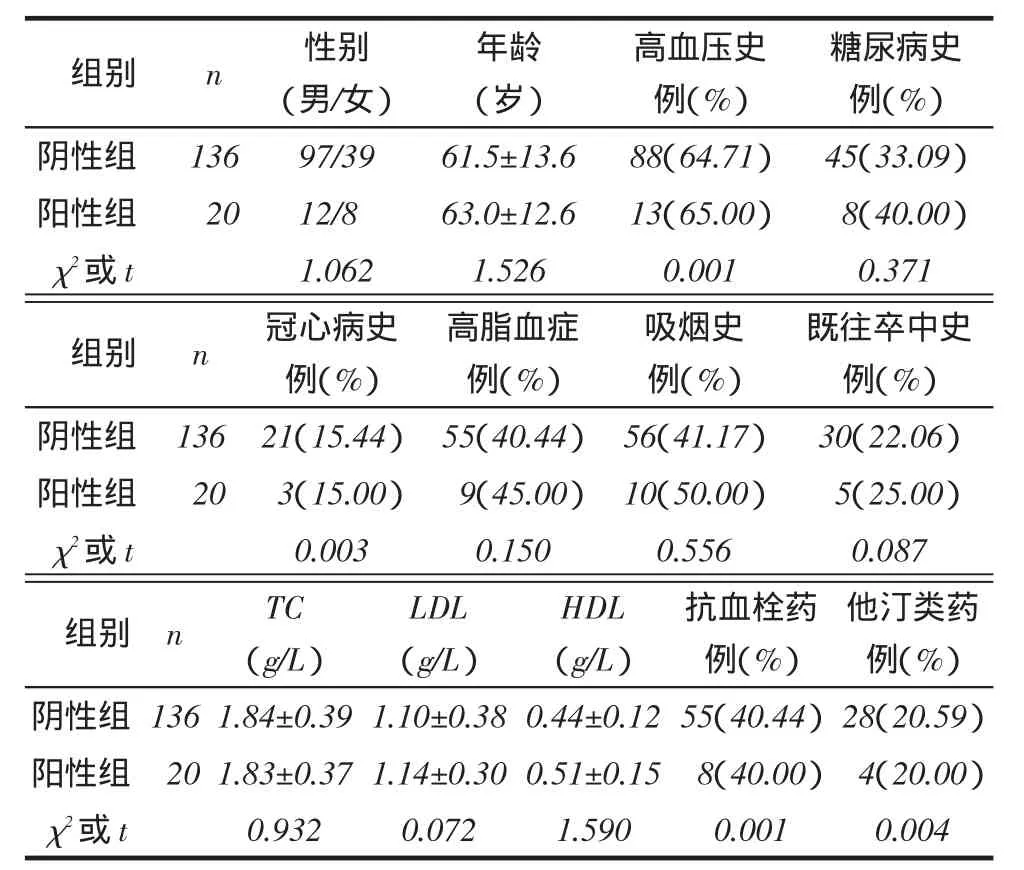
Tab. 1 Comparison of the clinical characteristics between two groups表1 2组一般资料比较
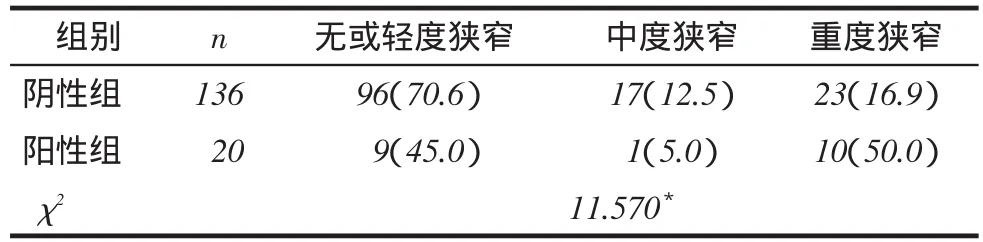
Tab. 2 Comparison of different degrees of VBA stenosis between two groups表2 2组不同狭窄程度的情况比较 例(%)
2.2椎基底动脉狭窄患者不同部位情况156例中无椎基底动脉狭窄70例、轻度35例、中度18例、重度33例;轻、中及重度狭窄86例均为椎基底动脉狭窄,其中MES阳性14例,阴性72例。MES阳性组和阴性组在不同狭窄部位差异有统计学意义,阴性组各狭窄部位比例差异不大,而阳性组中颅内椎基底动脉狭窄率高于85%(P<0.05),见表3。
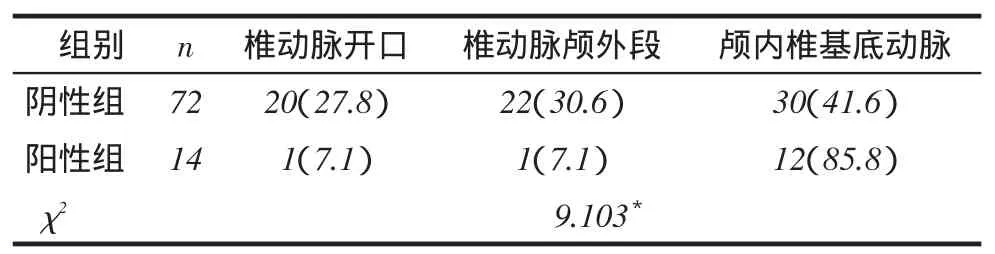
Tab. 3 Comparison of different VBA stenosis locations between two groups of patients表3椎基底动脉狭窄患者不同狭窄部位的比较例(%)
2.3椎基底动脉狭窄患者MES表达阳性组和阴性组的单一梗死和多部位梗死情况比较阳性组多部位梗死比例高于阴性组(P<0.05),见表4。
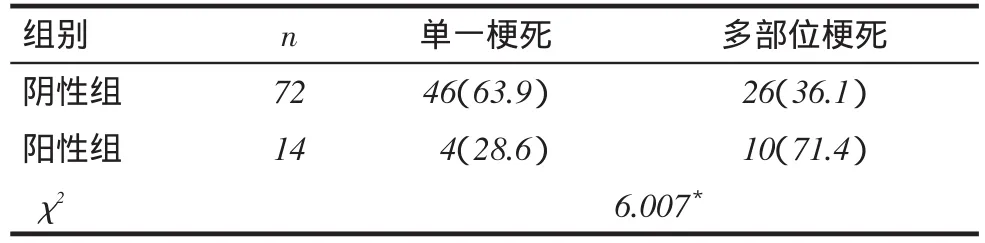
Tab. 4 Comparison of different infarct lesions between two groups of patients表4椎基底动脉狭窄患者脑梗死部位比较 例(%)
2.3 MES影响因素分析结果以MES为因变量(有=1,无=0),以年龄( 65岁=0,<65岁=1)、性别(女=0,男=1)、监测时间( 24 h=0,>24 h=1)、动脉狭窄(部位和程度)、吸烟、糖尿病、高血压、冠心病、高脂血症为自变量(均为无=0,有=1),Logistic多因素回归分析结果显示,颅内椎基底动脉狭窄、椎基底动脉狭窄75%以上为MES的危险因素(均P<0.05),见表5。
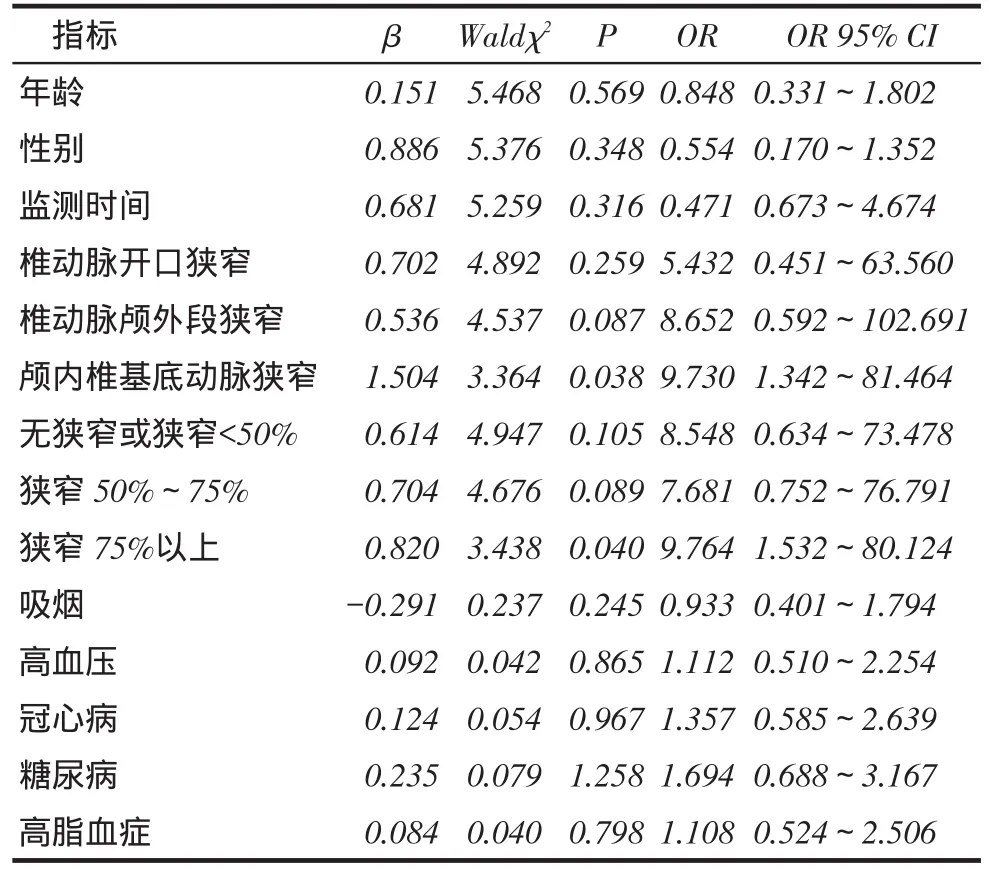
Tab. 5 The multivariate Logistic regression analysis of factors influencing microembolic signals表5微栓子影响因素的多元Logistic回归分析
3 讨论
目前,MES监测主要应用于前循环脑梗死。Kinsella等[3]研究表明,重度狭窄患者较轻、中度狭窄患者微栓子阳性率高,其中12.2%患者再次出现缺血性脑血管病。Markus等[4]对70%狭窄以上的无症状颈动脉狭窄患者进行MES监测示,MES阳性患者2年内发生缺血性脑血管病风险是阴性患者的2.54倍。后循环椎基底动脉狭窄的MES监测的报道少见,主要原因为后循环血管不易固定头架监测。Hwang等[5]对140例急性后循环缺血性脑血管病患者进行MES监测显示,18例(12.9%)患者出现微栓子,认为椎基底动脉狭窄是微栓子阳性的独立相关因素,重度椎基底动脉狭窄者微栓子出现频率较轻、中度狭窄者更高,头MRI出现多病灶的患者微栓子阳性率较单一病灶患者更多。本研究Logistic回归分析示,颅内椎基底动脉狭窄、尤其椎基底动脉重度狭窄为MES阳性的独立危险因素,而颅外段椎动脉狭窄不是MES影响因素。Telman等[6]研究亦显示,椎基底动脉狭窄是脑血管发生缺血事件和复发的重要原因,而椎动脉颅外段很少有症状。有研究推测原因可能为椎动脉颅外段斑块所受生物学剪应力小,斑块较稳定,不易破裂产生微栓子[7-8]。
Kinsella等[9]研究认为,颈动脉狭窄程度越重,MES出现频率越高。与颈动脉狭窄类似,本研究结果显示,椎基底动脉狭窄(狭窄 50%)较无狭窄或狭窄<50%MES阳性率高,并且椎基底动脉重度狭窄较中度狭窄MES阳性率高,提示椎基底动脉狭窄程度严重,MES出现频率升高。Logistic多因素回归分析表明椎基底动脉狭窄是急性脑梗死MES阳性的主要影响因素,与Hwang等[5]研究结果一致。有研究认为,高度狭窄的血管之所以易于产生MES,可能与血流动力学改变有关,管腔狭窄越明显,血流速度越快,冲刷狭窄的血管壁和斑块所受生物学剪应力就越大,可引起斑块脱落,同时当血液流经狭窄处进入较宽的血管腔时,易于在旋涡处聚集成凝块,从而产生微栓子,另外也可能与狭窄处的病变组织性质和类型不同有关[10]。
本研究86例有椎基底动脉狭窄,MES阳性组较阴性组脑梗死病灶增多,表明椎基底动脉狭窄患者的微栓子可能是多部位脑梗死的病因,可能机制为血管源性微栓子脱落,阻塞了不同小动脉,出现缺血,从而表现为急性脑梗死的各种临床症状。虽然一些研究提到后循环狭窄患者有DWI的严重病变,但该文未探讨椎基底动脉狭窄的脑梗死发生机制[11]。一般情况下,DWI显示的多部位梗死是脑梗死栓塞发生机制的标志,而应用MES监测和DWI病变分析有助于发现脑梗死患者的发病机制。
综上所述,对于椎基底动脉狭窄的患者可以通过枕窗进行基底动脉MES监测,重度狭窄的椎基底动脉更易出现后循环系统的MES,导致脑梗死;微栓子可能是椎基底动脉狭窄出现多部位脑梗死的发病原因。
参考文献
[1] Molloy J, Markus HS. Asymptomatic embolization predicts stroke and TIA risk in patients with carotid artery stenosis[J]. Stroke, 1999, 30(7):1440-1443. doi: 10.1161/01.STR.30.7.1440.
[2] Saedon M, Dilshad A, Tiivas C, et al. Prospective validation study of transorbital doppler ultrasound imaging for the detection of tran⁃sient cerebral microemboli[J]. Br J Surg, 2014 ,101 (12): 1551-1555.doi:10.1002/bjs.9634.
[3] Kinsella JA, Tobin WO, Kavanagh GF, et al. Increased thrombin generation potential in symptomatic versus asymptomatic moderate or severe carotid stenosis and relationship with cerebral microemboli[J]. J Neurol Neurosurg Psychiatry, 2015, 86(4):460-467. doi:10.1136/ jnnp-2015-312067.
[4] Markus HS, King A, Shipley M, et al. Asymptormtic embolisation for prodiction of stroke in the Asymptomatic Carotid Emboli Study (ACES):a prospective observational study[J]. Lancet Neurol, 2010,9 (7): 663-671.doi: 10.1016/S1474-4422(10)70120-4.
[5] Hwang J, Kim SJ, Hong JM, et al. Microembolic signals in acute pos⁃terior circulation cerebral ischemia sources and consequences[J]. Stroke, 2012, 43(3):747-752. doi:10.1161/STROKEAHA.111.633438.
[6] Telman G, Sprecher E, Kouperberg E. Microembolic signals in patients with acute nonembolic stroke[J]. JStroke Cerebrovasc Dis, 2013, 22 (7): 31-33. doi: 10.1016/j.jstrokecerebrovasdis.2012.03.017.
[7] Wu XJ, Xing YQ, Wang J, et al. Clinical utilization of microem⁃ bolus detection by transcranial Doppler sonography in intracranial stenosis occlusive disease[J]. Chin Med J, 2013, 126(7):1355-1359.
[8] Wang X, Lin WH, Zhao YD, et al. The effectiveness of dual isch⁃emic stroke patients with intracranial arterial stenosis subgroup analysis of CL- AIR study[J]. Int J Stroke, 2013, 8(8):663- 668. doi: 10.1111/j.1747-4949.2012.00828.x.
[9] Kinsella JA, Tobin WO, Tierney S, et al. Increased platelet activa⁃tion in early symptomatic vs. asymptomatic carotid stenosis and rela⁃tionship with microembolic status: results from the Platelets and Ca⁃rotid Stenosis Study[J]. J Thromb Haemost, 2013, 11(7): 1407-1416. doi: 10.1111/jth.12277.
[10] Ritter MA, Theismann K, Schmiedel M, et al. Vascularization of ca⁃rotid plaque in recently symptomatic patients is associated with the occurrence of transcranial microembolicsignals[J]. Eur J Neurol, 2013, 20 (8): 1218-1221. doi: 10.1111/ene.12030.
[11] Ay H, Oliveira-Filho J, Buonanno FS, et al. Diffusion weighted imaging identifies asubset of lacunar infarction associated with embolic source [J]. Stroke, 1999, 30(12):2644-2650. doi:10.1161/01.STR.30.12.2644.
(2015-07-27收稿2015-10-23修回)
(本文编辑陆荣展)
应用研究
The role of microembolic signal monitoring in brainstem infarction and vertebrobasilar artery stenosis
RONG Yanhong, ZHAO Kun , SU Hongjun, QI Jinlong
Neurology Department, Baodi People′s Hospital, Tianjin 301800, China Corresponding Author E-mail:rongrong790125@163.com
Abstract:Objective To investigate the relation between microembolic signals (MES) and vertebral basilar artery ste⁃nosis in patients with brainstem infarction. Methods A total of 156 patients with acute brainstem infarction, who were de⁃termined the cerebral infarction lesion and vertebral basilar artery stenosis by cranial magnetic resonance imagingand CT an⁃giography, and were monitored by transcranial Doppler via occipital window of basilar arterial MES monitoring in 7 days of the onset, were divided into microembolus signal negative group (n=136) and positive group (n=20). The clinical data were compared between two groups. The differences of different degrees of stenosis were analyzed in two groups. The differences of different locations of stenosis in patients with vertebral basilar artery stenosis were analyzed in two groups. Logistic regres⁃sion analysis was used to analyse the factors affecting MES. Results There were no significant differences in age, gender, history of hypertension and diabetes mellitus between the two groups (P<0.05). There were significant differences in the dif⁃ferent degrees of stenosis between two groups, no or mild stenosis was found in MES-negative group and severe stenosis in MES-positive group (P<0.05). There were 70 cases with no vertebral basilar artery stenosis, 86 cases with mild, moderate and severe stenosis, in which 14 cases were MES-positive and 72 cases were negative. There were significant differences in different locations of stenosis between the two groups. The proportion of multiple infarctions was significantly higher in MES-positive group than that of MES-negative group (P<0.05). The intracranial vertebral basilar artery stenosis and 75% of ver⁃tebral basilar artery stenosis were the independent risk factors of MES-positive. Conclusion Severe stenosis of the verte⁃bral basilar artery is more vulnerable to occur MES of posterior circulation, leading to cerebral infarction. Microemboli may be the cause of multiple infarctions in patients with vertebral basilar artery stenosis.
Key words:brain stem infarction; vertebral basilar artery stenosis; microembolic signal; transcranial doppler ultraso⁃nography目前,微栓子信号(microembolic signals,MES)监测已经广泛应用于缺血性脑卒中。MES在预测颈内动脉和大脑中动脉缺血性卒中方面起着重要的作用,MES监测是判断颅内动脉栓子来源的重要依据[1-2]。但是,目前有关椎基底动脉系统的后循环和脑干梗死的MES监测研究尚少见相关报道。本研究拟通过经颅多普勒超声(TCD)对脑干梗死患者经枕窗行基底动脉MES监测,探讨脑干梗死患者微栓子与椎基底动脉狭窄的关系。
中图分类号:R743.33
文献标志码:A
DOI:10.11958/20150054
作者简介:荣艳红(1979),女,硕士,主要从事脑血管病的研究
通讯作者E-mail:rongrong790125@163.com