综合糖脂代谢指标与冠状动脉病变严重程度的相关性研究
2016-05-28温志超施海明范维琥倪唤春罗心平
于 佳 温志超 洪 晋 李 剑 施海明 范维琥 倪唤春 罗心平
200040 上海,复旦大学附属华山医院心内科
·临床研究·
综合糖脂代谢指标与冠状动脉病变严重程度的相关性研究
于佳温志超洪晋李剑施海明范维琥倪唤春罗心平
200040 上海,复旦大学附属华山医院心内科
【摘要】目的:探讨综合糖脂代谢指标与冠状动脉(冠脉)病变程度的关系及其临床意义。方法:入选2012年3月至2013年12月于我院接受冠脉造影的717例患者,根据造影结果分为冠脉造影阴性的对照组(n=385)和冠心病组(n=332)。检测所有研究对象的血清糖化血红蛋白(HbA1c)、总胆固醇(TC)、低密度脂蛋白胆固醇(LDL-C)、高密度脂蛋白胆固醇(HDL-C)、三酰甘油(TG)等,采用Gensini评分评估冠脉病变严重程度。采用Pearson相关系数分析连续性变量之间的相关性,Spearman相关系数检测分类变量之间的相关性。线性回归分析综合糖脂代谢指标HbA1c×LDL-C/HDL-C与Gensini积分的线性关系,非条件Logistic回归分析HbA1c×LDL-C/HDL-C与冠脉病变支数的相关性,受试者工作特征(ROC)曲线评价HbA1c×LDL-C/HDL-C预测冠脉严重程度、冠脉多支病变的价值。结果:血清HbA1c、LDL-C水平、HbA1c×LDL-C/HDL-C与Gensini积分呈正相关,而HDL-C水平与Gensini积分呈负相关。线性回归显示HbA1c×LDL-C/HDL-C与Gensini积分呈线性相关,其判断冠脉病变严重程度的ROC曲线下面积为0.724(P<0.01)。Logistic回归分析显示HbA1c×LDL-C/HDL-C与冠脉病变支数显著相关,其判断冠脉病变支数的ROC曲线下面积为0.638(P<0.01)。结论:综合糖脂代谢指标对冠脉粥样硬化病变严重程度、病变支数有一定的预测价值。
【关键词】冠状动脉粥样硬化性心脏病;糖化血红蛋白;低密度脂蛋白胆固醇;高密度脂蛋白胆固醇
冠状动脉粥样硬化性心脏病(冠心病)存在多个危险因素,其中低密度脂蛋白胆固醇(LDL-C)是目前公认的危险因素,与冠心病的发病率和死亡率密切相关[1-2]。高密度脂蛋白胆固醇(HDL-C)水平降低可增加冠心病发病风险[3],糖化血红蛋白(HbA1c)是心血管疾病发生和死亡的重要预测因子[4-5]。临床上冠心病患者常合并血糖、血脂紊乱,单一指标难以准确、全面地反映冠心病风险。本研究将血清LDL-C、HDL-C和HbA1c水平合并作为综合糖脂代谢指标,探讨其与冠状动脉(冠脉)粥样硬化严重程度的关系。
1对象和方法
1.1研究对象
入选2012年3月至2013年12月在复旦大学附属华山医院心内科住院并接受冠脉造影的拟诊冠心病患者717例。根据造影结果分为2组:冠脉造影阴性的对照组(n=332)和冠心病组(n=332)。冠心病诊断标准:冠脉造影示左主干、左前降支、回旋支、右冠脉或其主要分支的血管直径狭窄≥50%。高血压病诊断标准:收缩压≥140 mmHg和(或)舒张压≥90 mmHg,或正在服用降压药物治疗。糖尿病诊断采用美国糖尿病协会标准:空腹血糖≥7.0 mmol/L,或葡萄糖耐量试验2 h血糖≥11.1 mmol/L,或正在服用降糖药物治疗。排除标准:临床资料或冠脉造影资料不全;严重肝、肾功能不全;恶性肿瘤。本研究经过华山医院医学伦理委员会同意,所有入选者签署知情同意书。
1.2研究方法
所有患者入院8 h内采集病史,进行全身体格检查,24 h内采集空腹肘静脉血,进行血脂、血糖、HbA1c、肝功能、肾功能等生化检查。
所有入选对象在完善常规生化检查、排除造影禁忌后,进行冠脉造影。采用Judkins法体位投照,血管入路首选经皮穿刺桡动脉,经桡动脉入路困难时采用经皮穿刺股动脉。
冠脉病变支数的判断以管径狭窄≥50%为病变阳性。冠脉多支病变指2支及以上的冠脉在造影中存在≥50%的狭窄和(或)左主干病变。
Gensini评分由两位有经验的心内科医生在盲法下独立进行。Gensini积分计算方法如下:(1)冠脉狭窄程度≤25%为1分,25%~49%为2分,50%~74%为4分,75%~89%为8分,90%~98%为16分,99%~100%为32分;(2)病变部位系数:左主干×5,左前降支:近段×2.5、中段×1.5、远段×1、第一对角支×1、第二对角支×0.5,回旋支:近段×2.5、中段×1、钝缘支×1、后降支×1、后侧支×0.5,右冠脉:近段×1、远段×1、后降支×1;(3)相应积分数与系数相乘后求和为Gensini积分[6]。
1.3统计学分析
采用SPSS19统计软件进行数据处理。计量资料用均数±标准差表示,计数资料用例数和百分数表示。计量资料组间比较使用t检验;计数资料组间比较采用方差分析。Pearson相关系数检测连续性变量之间的相关性,Spearman相关系数检验分类变量之间的相关性。线性回归分析HbA1c×LDL-C/HDL-C与Gensini积分的线性关系,非条件Logistic回归分析HbA1c×LDL-C/HDL-C与冠脉病变支数的相关性,ROC曲线评价HbA1c×LDL-C/HDL-C预测冠脉病变严重程度、多支病变的价值。以P<0.05为有统计学差异。
2结果
2.1基线资料比较
两组间年龄、性别构成、体质量指数(BMI)、收缩压、舒张压、三酰甘油(TG)水平无显著差异(P均>0.05)。与对照组相比,冠心病组中吸烟率、高血压和糖尿病患病率、血清HbA1c、总胆固醇(TC)和LDL-C水平明显较高(P<0.05),而HDL-C和左室射血分数(LVEF)明显低于对照组(P<0.05)。
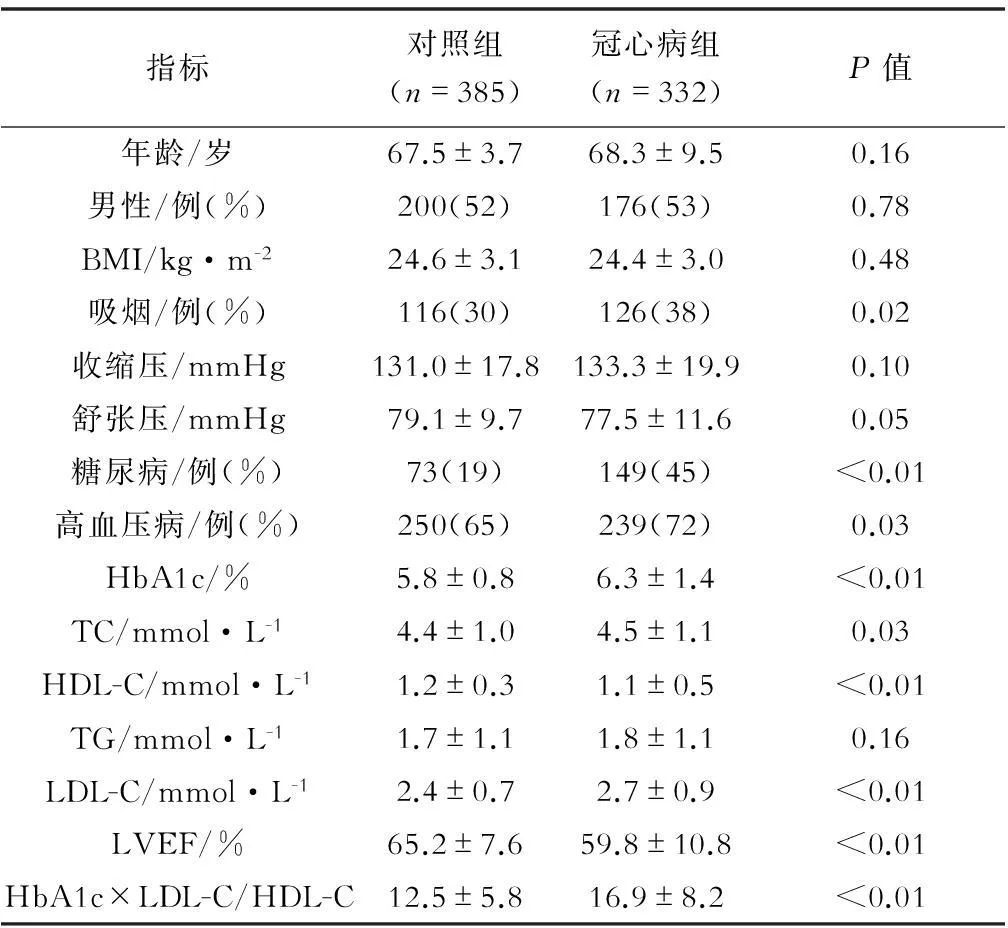
表1 两组患者的临床基线资料
2.2糖脂代谢指标与Gensini积分
冠心病风险因素与Gensini积分的相关性分析显示,HbA1c、LDL-C水平与Gensini积分呈正相关,HDL-C水平与Gensini积分呈负相关,HbA1c×LDL-C/HDL-C与Gensini积分的正相关性更显著,见表2。
线性回归分析显示,HbA1c×LDL-C/HDL-C与Gensini积分具有显著线性关系,方程为y=1.07x+38.69,y=Gensini积分,x=HbA1c×LDL-C/HDL-C,r2=0.038,P<0.01。

表2 冠心病组风险因素与Gensini积分的相关性分析
根据Gensini积分结果将患者分为低Gensini积分组(<40分)和高Gensini积分组(≥40分)[7]。将HbA1c×LDL-C/HDL-C划分为若干临界点,以每个临界点对应的灵敏度为纵坐标,1-特异度为横坐标,作图得到ROC曲线(见图1),曲线下面积为0.724(0.679~0.768),P<0.01。约登指数最大值为0.385,此时对应的HbA1c×LDL-C/HDL-C值为15.46。
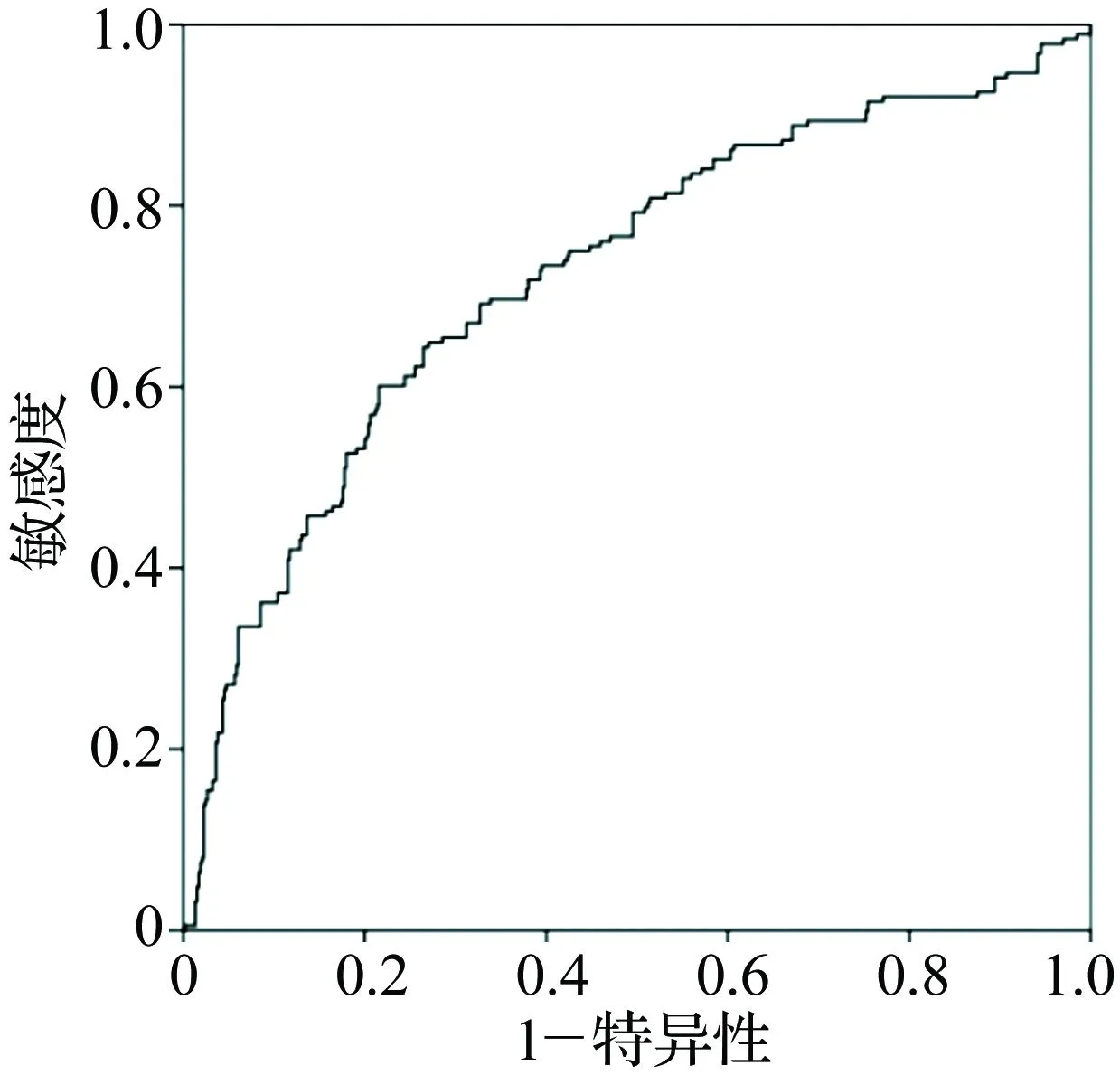
图1 综合糖脂代谢指标判断冠脉病变的ROC曲线
2.3糖脂代谢指标与冠脉病变支数
以冠脉多支病变为因变量,Logistic回归分析HbA1c×LDL-C/HDL-C与冠脉多支病变的关系,结果显示高HbA1c×LDL-C/HDL-C是发生冠状动脉多支病变的危险因素(OR=1.053,95%CI:1.021~1.086,P=0.001)。
根据冠脉造影结果将冠心病患者分为单支病变组和多支病变组,将HbA1c×LDL-C/HDL-C划分为若干临界点,作ROC曲线(见图2)得到曲线下面积为0.638(0.576~0.699),P<0.01。约登指数最大值为0. 251,此时对应的HbA1c×LDL-C/HDL-C值为15.11。
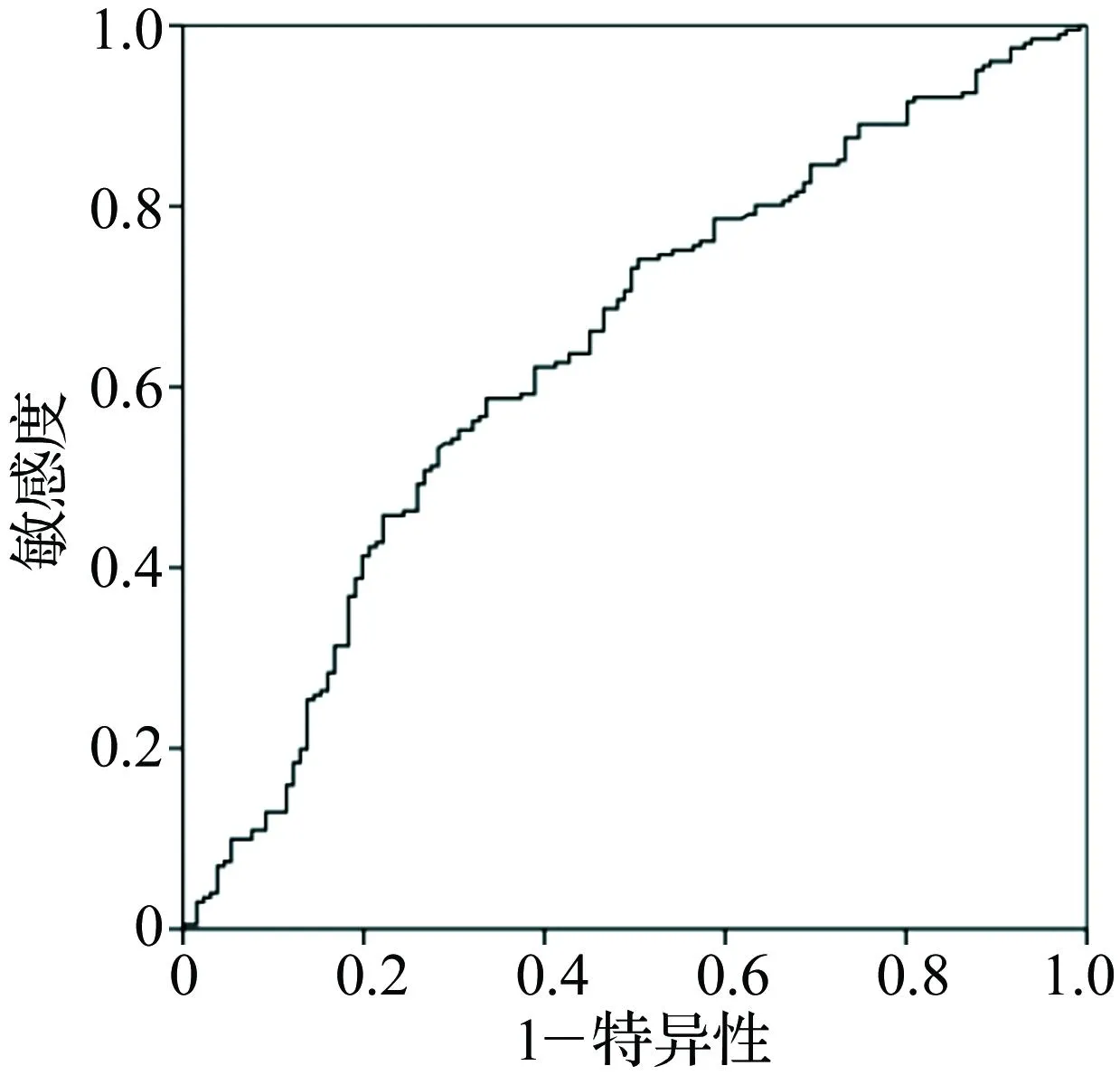
图2 综合糖脂代谢指标判断冠脉多支病变的ROC曲线
3讨论
血脂异常,特别是高水平LDL-C和低水平HDL-C已被确定为冠心病的危险因素[8-9]。荟萃分析显示,LDL-C水平每下降1 mmol/L,冠脉事件可减少23%[10]。当HDL-C<40 mg/dL时,冠心病风险增加明显[11],HDL-C水平每降低1 mg/dL,冠心病风险上升2%~3%[12]。Quebec心血管研究显示,HDL-C水平每下降10%,冠心病风险增加13%[13]。研究发现,LDL-C/HDL-C比单一的LDL-C、HDL-C更能预测冠心病风险,LDL-C/HDL-C与冠脉病变严重程度具有显著相关性[14]。TC/HDL-C、LDL-C/HDL-C、TG/HDL-C与冠脉病变支数密切相关[15]。HbA1c是血红蛋白与葡萄糖发生缓慢非酶促反应形成的复合物,反映近2个月的平均血糖水平。多项研究显示高HbA1c水平增加冠心病发生率[16-17]。HbA1c水平每上升1%,心血管事件和全因死亡率增加20%~30%,并且这种相关性不受糖尿病的影响[18]。
本研究将以上3个冠心病的重要危险因素合并为一个综合指标HbA1c×LDL-C/HDL-C,评价其对冠脉病变严重程度和病变支数的预测作用。结果显示,HbA1c、LDL-C、HbA1c×LDL-C/HDL-C水平均与Gensini积分呈正相关,HDL-C水平与Gensini积分呈负相关,与已有研究结果一致[19-21]。线性回归分析显示,HbA1c×LDL-C/HDL-C与Gensini积分具有显著的线性关系,其判断冠脉病变严重程度的ROC曲线下面积为0.724,诊断临界值为15.46。Logistic回归分析显示HbA1c×LDL-C/HDL-C与冠脉多支病变的风险显著相关,ROC曲线下面积为0.638,临界诊断值为15.11。该综合糖脂代谢指标对冠脉病变严重程度、多支病变具有一定的预测意义。
本研究中HbA1c×LDL-C/HDL-C判断冠脉病变严重程度、多支病变的ROC曲线下面积均不大。此外,本研究样本量偏小,该综合糖脂代谢指标对于冠脉病变严重程度的相关性需增加样本量进一步明确。
参考文献
[1]Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010[J]. Lancet,2012,380(9859):2095-2128.
[2]Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins[J]. Lancet,2005,366(9493):1267-1278.
[3]Boekholdt SM, Arsenault BJ, Hovingh GK, et al. Levels and changes of HDL cholesterol and apolipoprotein A-I in relation to risk of cardiovascular events among statin-treated patients: a meta-analysis[J]. Circulation,2013,128(14):1504-1512.
[4]van't Riet E, Rijkelijkhuizen JM, Alssema M, et al. HbA1c is an independent predictor of non-fatal cardiovascular disease in a Caucasian population without diabetes: a 10-year follow-up of the Hoorn Study[J]. Eur J Prev Cardiol,2012,19(1):23-31.
[5]Selvin E, Steffes MW, Zhu H, et al. Glycated hemoglobin, diabetes, and cardiovascular risk in nondiabetic adults[J]. N Engl J Med,2010,362(9):800-811.
[6]Gensini GG. A more meaningful scoring system for determining the severity of coronary heart disease[J]. Am J Cardiol,1983,51(3):606.
[7]Wang Y, Zheng A, Yan Y, et al. Association between HMW adiponectin, HMW-total adiponectin ratio and early-onset coronary artery disease in Chinese population[J]. Atherosclerosis,2014,235(2):392-397.
[8]National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel Ⅲ) final report[J]. Circulation,2002,106(25):3143-3421.
[9]Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel Ⅲ)[J]. JAMA,2001,285(19):2486-2497.
[10]Cholesterol Treatment Trialists’ (CTT) Collaboration, Baigent C, Blackwell L, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials[J]. Lancet,2010,376(9753):1670-1681.
[11]Castelli WP, Anderson K, Wilson PW, et al. Lipids and risk of coronary heart disease. The Framingham Study[J]. Ann Epidemiol,1992,2(1-2):23-28.
[12]Gotto AM, Jr. High-density lipoprotein cholesterol and triglycerides as therapeutic targets for preventing and treating coronary artery disease[J]. Am Heart J,2002,144(6 Suppl):S33-S42.
[13]Despres JP, Lemieux I, Dagenais GR, et al. HDL-cholesterol as a marker of coronary heart disease risk: the Quebec cardiovascular study[J]. Atherosclerosis,2000,153(2):263-272.
[14]Momiyama Y, Ohmori R, Fayad ZA, et al. The LDL-cholesterol to HDL-cholesterol ratio and the severity of coronary and aortic atherosclerosis[J]. Atherosclerosis,2012,222(2):577-580.
[15]吴燕丹. TC/HDL-C、LDL-C/HDL-C、TG/HDL-C与冠心病不同程度相关性[J]. 临床误诊误治,2014,(6):64-67.
[16]Ueda H, Mitsusada N, Harimoto K, et al. Glycosylated hemoglobin is a predictor of major adverse cardiac events after drug-eluting stent implantation in patients with diabetes mellitus[J]. Cardiology,2010,116(1):51-57.
[17]Kataoka Y, Shao M, Wolski K, et al. Multiple risk factor intervention and progression of coronary atherosclerosis in patients with type 2 diabetes mellitus[J]. Eur J Prev Cardiol,2013,20(2):209-217.
[18]Khaw KT, Wareham N, Luben R, et al. Glycated haemoglobin, diabetes, and mortality in men in Norfolk cohort of european prospective investigation of cancer and nutrition (EPIC-Norfolk)[J]. BMJ,2001,322(7277):15-18.
[19]Ashraf H, Boroumand MA, Amirzadegan A, et al. Hemoglobin A1C in non-diabetic patients: an independent predictor of coronary artery disease and its severity[J]. Diabetes Res Clin Pract,2013,102(3):225-232.
[20]Xu RX, Li S, Li XL, et al. High-density lipoprotein subfractions in relation with the severity of coronary artery disease: A Gensini score assessment[J]. J Clin Lipidol,2015,9(1):26-34.
[21]Niccoli G, Baca M, De Spirito M, et al. Impact of electronegative low-density lipoprotein on angiographic coronary atherosclerotic burden[J]. Atherosclerosis,2012,223(1):166-170.
(收稿:2015-08-10修回:2016-02-16)
(本文编辑:梁英超)
Correlation between glycolipid metabolism index and the severity of coronary artery disease
YUJia,WENZhichao,HONGJin,LIJian,SHIHaiming,FANWeihu,NIHuanchun,LUOXinping.
DepartmentofCardiology,HuashanHospital,FudanUniversity,Shanghai200040,China
【Abstract】Objective: To investigate the relation between comprehensive glycolipid metabolism index and the severity of coronary artery disease.Methods: From March 2012 to December 2013, a total of 385 patients were enrolled into the control group, and 332 patients were enrolled into the case group according to the result of coronary angiography. Levels of serum HbA1c, total cholesterol (TC),low-density lipoproteincholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C) and triglyceride (TG) were detected. The severity of coronary artery disease was assessed by Gensini score.Pearson correlation analysis was used to detect the relationship between continuous variables, and Spearman correlation analysis was used to detect the relationship between categorical variables.Linear regression was used to analyze the linear relation between glycolipid metabolism index and the Gensini score. Non-conditional logistic regression was used to identify the correlation between HbA1c×LDL-C/HDL-C and the number of coronary artery lesion vessels. Receiver operating characteristic (ROC) curve was used to evaluate the predictive value of HbA1c×LDL-C/HDL-C for the severity of coronary artery disease and the number of coronary artery lesion vessels.Results: Correlation analysis showed that there were positive correlation between levels of HbA1c, LDL-C, HbA1c×LDL-C/HDL-C and the Gensini score, and there was a negative correlation between level of HDL-C and the Gensini score.Linear regression analysis revealed a strong correlation between HbA1c×LDL-C/HDL-C and the Gensini score, and the area under the ROC curve was 0.724(P<0.01).Logistic regression analysis showed that HbA1c×LDL-C/HDL-C was closely related with the number of lesion branches, and the area under the ROC curve was 0.638 (P<0.01).Conclusion: Glycolipid metabolism index has certain predictive value of the severity of coronary artery disease and number of coronary artery lesion vessels.
【Key words】Coronary artery disease; Hemoglobin A1c;Low-density lipoprotein cholesterol; High-density lipoprotein cholesterol
doi:10.3969/j.issn.1673-6583.2016.02.014
通信作者:倪唤春, Email:docnhc@126.com
基金项目:上海市卫生局科研项目(20134312)