红细胞分布宽度与阵发性非瓣膜性心房颤动射频消融后复发的关系
2016-05-18李宏亮刘彤许纲刘恩照焦占全李广平
李宏亮,刘彤,许纲,刘恩照,焦占全,李广平
(天津医科大学第二医院心脏科,天津市心血管病离子与分子机能重点实验室,天津心脏病学研究所,天津300211)
论著
红细胞分布宽度与阵发性非瓣膜性心房颤动射频消融后复发的关系
李宏亮,刘彤,许纲,刘恩照,焦占全,李广平
(天津医科大学第二医院心脏科,天津市心血管病离子与分子机能重点实验室,天津心脏病学研究所,天津300211)
目的:探讨红细胞分布宽度(RDW)与阵发性非瓣膜性心房颤动(房颤)导管射频消融后复发的关系。方法:入选阵发性非瓣膜性房颤患者73例,均首次行环肺静脉消融术。收集所有患者的RDW、房颤病程、血清非结合胆红素水平、总胆红素水平、左房直径的临床数据。设定术后3个月为空白期。平均随访(17±15)个月。复发定义为术后3个月发生的持续时间>30 s的快速房性心律失常,包括房速、房扑、房颤。采用多元Logistic回归分析RDW与复发的关系。结果:房颤复发24例、未复发49例,复发组患者术前RDW、左房直径、房颤病程、间接胆红素、总胆红素均高于未复发组(P<0.05),经多元Logistics回归显示,左房直径、房颤病程、RDW是房颤消融术后复发的独立危险因素。结论:RDW增高、左房直径增大、房颤病程延长与阵发性非瓣膜性房颤患者导管射频消融后复发有关。
心房颤动;红细胞分布宽度;射频消融;复发
红细胞分布宽度 (red cell distribution width, RDW)是反映外周血红细胞体积异质性的参数,通常以红细胞体积大小的变异系数来表示,临床上多用于缺铁性贫血的诊断和鉴别诊断。近年来研究发现,RDW增高与心功能衰竭[1]、冠心病、脑卒中[2]及肺动脉高压患者的死亡密切相关,可能是一种新的心血管疾病危险标记物[3]。然而,关于RDW与阵发性心房颤动(房颤)射频消融术后复发的关系研究甚少。本研究对RDW与阵发性房颤患者射频消融术后复发的关系进行探讨。
1 资料与方法
1.1 临床资料 2011年1月-2014年12月在本院心内科因阵发性非瓣膜性房颤接受射频消融治疗的住院患者共104例,均为第1次行射频消融治疗的症状性房颤患者,且资料完整。排除标准:急性感染或慢性感染急性加重期、严重肝肾功能障碍、甲状腺功能亢进等甲状腺疾病、随访期间发生死亡、血红蛋白<100 g/L。符合以上标准的73例患者完成随访,男44例、女29例,年龄(62±9)岁,病程(6.5± 6.0)年,合并心房扑动(房扑)及房性心动过速(房速)9例、预激综合征1例、病态窦房结综合征1例、高血压42例、冠心病25例、2型糖尿病18例,既往有脑卒中病史5例。
1.2 射频消融 患者常规开放静脉通道,芬太尼0.5 mg加安定10 mg经生理盐水稀释至50 mL后静脉恒速泵入(5~8 mL/h),必要时给予负荷量2~5 mL。在三维电解剖标测系统(CART0或EnsiteNavx)指导下,行肺静脉环形消融电隔离术,预设温度43℃。放电时生理盐水输入速度17mL/h。每点消融30~40s至局部心房电位振幅下降80%或呈现双电位,逐点连接成线,达到肺静脉电位完全消失且至少30 min无复发,左心房-肺静脉传导双向阻滞。完成消融线路,对术中经消融不能终止房颤的患者进行同步直流电复律。术中30~60 min监测激活的凝血酶原时间,调整肝素用量,维持凝血酶原时间250~350 s。
1.3 观察指标 患者均于入院次日晨空腹采集肘静脉血2 mL,采用全自动血细胞分析仪测定RDW,用全自动生化分析仪测定非结合胆红素、总胆红素水平。术前采用心脏彩超测定左房直径。术后随访,设定术后3个月为空白期,3个月后开始至研究结束随访患者的复发情况,患者出现持续时间>30 s的房颤、房扑、房速为复发。
1.4 统计学方法 采用SPSS22.0统计软件。计量资料用s表示,组间比较采用t检验;采用多变量Logistic回归分析消融术后复发的危险因素。P<0.05为差异有统计学意义。
2 结果
73例患者术后平均随访(17±15)个月。术后3个月房颤复发24例(复发组),未复发49例(未复发组)。房颤复发组RDW、左房直径、房颤病程、非结合胆红素、总胆红素明显高于未复发组(P<0.05),见表1。经多变量Logistic回归分析显示,RDW、左房直径、病程是房颤消融术后复发的独立危险因素(P<0.05),见表2。
表1 两组RDW、左房直径、病程、非结合胆红素、总胆红素比较(s)Tab 1 Comparison of baseline charactersistics between two groups of patients(s)

表1 两组RDW、左房直径、病程、非结合胆红素、总胆红素比较(s)Tab 1 Comparison of baseline charactersistics between two groups of patients(s)
与未复发组比较,*P<0.05
总胆红素/(μmol/L)复发组 24 13.0±1.0*44.0±5.2*8.7±4.0*11.9±5.5* 14.8±5.6*未复发组49 12.4±0.6 39.4±5.2 5.4±6.6 9.1±3.2 12.1±3.9组别 nRDW/% 左房直径/ mm 病程/年非结合胆红素/(μmol/L)
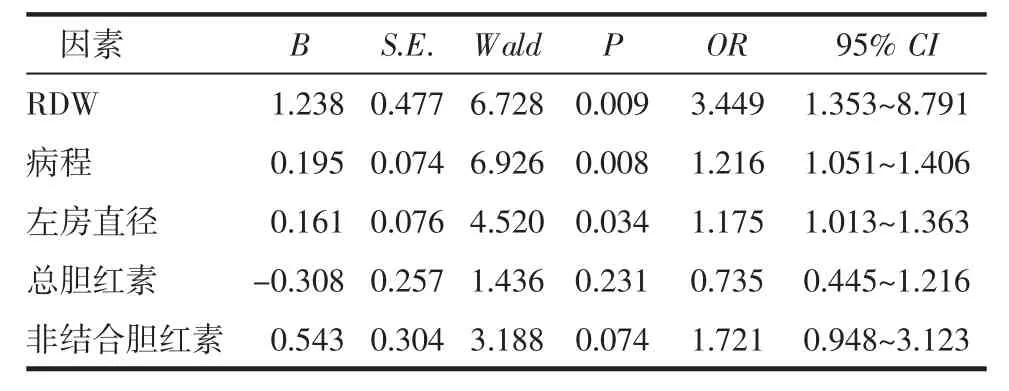
表2 房颤患者消融术后复发的危险因素分析Tab 2 Results of Logistic regression analysis of influencing factors of atrial fibrillation
3 讨论
2007年Felker等[5]首次发现心力衰竭患者的RDW明显升高,且是预后的独立危险指标[6]。更高基线的RDW水平可以预测冠状动脉搭桥术后患者房颤的发生[7],是阵发性房颤的独立预测分子[8]。一项为27 124例患者大型研究[9]结果表明,RDW处在后25%的人群比处在前25%的人群房颤的发生率高33%。越来越多的证据表明,炎症和氧化应激在房颤的发生发展过程中具有重要作用[10~12]。外周血中高RDW水平反映激活的应激(炎症)状态[13-14]。在体快速心房起搏狗的模型研究表明,在房颤的背景下,RDW与炎症、氧化应激水平有潜在的联系[15]。房颤消融术后复发组RDW增高反映了慢性炎症可能是其共同的病理过程。炎性细胞因子可使骨髓红系干细胞对促红细胞生成素刺激不敏感,阻止其抗细胞凋亡和促进细胞成熟的作用。炎症因子抑制红细胞的成熟,导致未成熟红细胞进入循环,使红细胞大小异质性增加而RDW水平升高[16];增高的RDW还可能与慢性炎症导致的红细胞无效生成有关。其次,RDW增加,红细胞的可变形性降低,使得微循环血流通过受损,进而导致缺氧,诱发或加重了房颤患者机体的炎症状态。因此,RDW升高可作为预测房颤消融术后复发的独立危险因素。本研究发现,复发组术前RDW水平比未复发组明显增大,经Logistic回归分析显示,RDW是房颤消融术后复发的独立危险因素。
目前很多文献提到左房增大、房颤病程是房颤消融术后复发的独立危险因素。本研究通过多因素分析亦发现左房增大、房颤病程是房颤消融术后复发的独立危险因素。研究表明,胆红素在人体内具有很强的抗氧化作用,本研究中,复发组的非结合胆红素水平明显高于对照组,但在Logistic回归分析中非结合胆红素水平增高无明显意义。推测原因可能为氧化应激促进房颤的发生,而胆红素作为一种抗氧化应激因子,为了平衡体内的氧化和抗氧化而代偿性升高。
综上所述,RDW是房颤射频消融术后复发的独立危险因素。本研究样本小,没有评估其他炎性标记物对房颤消融术后复发的影响,需进一步研究探讨。
[1] Fasching P A,Jud S M,Hauschild M,et al.FemZone trial:a randomized phase II trial comparing neoadjuvant letrozole and zoledronic acid with letrozole in primary breast cancer patients[J]. Bmc Cancer,2014,14(6):804
[2] Rhodes C J,John W,Howard L S,et al.Red cell distribution width outperforms other potential circulating biomarkers in predicting survival in idiopathic pulmonary arterial hypertension[J].Heart, 2011,97(13):1054
[3] Ani C,Ovbiagele B.Elevated red blood cell distribution width predicts mortality in persons with known stroke[J].J Neurol Sci, 2009,277(1):103
[4] Gmallen F.Red cell distribution width as a novel prognostic marker in heart failure:data from the CHARM Program and the Duke Databank[J].J Am Coll Cardiol,2007,50(1):40
[5]柳森,王莉,周建华,等.红细胞分布宽度与心血管疾病的研究进展[J].中华心血管病杂志,2015,43(5):461
[6] Ertas G,Aydin C,Snmez O,et al.Red cell distribution width predicts new-onset atrial fibrillation after coronary artery bypass grafting[J].Scand Cardiovasc J,2013,47(3):132
[7] Liu T,Shao Q,Miao S,et al.Red cell distribution width as a novel, inexpensive marker for paroxysmal atrial fibrillation[J].Int J Cardiol, 2014,171(2):e52
[8] AdamssonES,BornéY,MelanderO,etal.Redblood cell distribution width is associated with incidence of atrial fibrillation[J].J Intern Med,2014,275(1):84
[9] Guo Y,Lip G Y,Apostolakis S.Inflammation in atrial fibrillation[J]. J Am Coll Cardiol,2012,60(22):2263
[10]Tousoulis D.Oxidative stress and inflammatory process in patients with atrial fibrillation:The role of left atrium distension[J].Int J Cardiol,2009,136(3):258
[11]Korantzopoulos P,Kolettis T M,Galaris D,et al.The role of oxidative stress in the pathogenesis and perpetuation of atrial fibrillation[J].Int J Cardiol,2007,115(2):135
[12]Emans M E,Gaillard C A,Pfister R,et al.Red cell distribution width is associated with physical inactivity and heart failure, independent of established risk factors,inflammation or iron metabolism;the EPIC-Norfolk study[J].Int J Cardiol,2013,168(4): 3550
[13]Ozcan F,Turak O,Durak A,et al.Red cell distribution width and inflammationinpatientswithnon-dipperhypertension[J].BloodPress, 2013,22(2):80
[14]Zhao Z,Liu T,Li J,et al.Elevated red cell distribution width level is associated with oxidative stress and inflammation in a canine model of rapid atrial pacing[J].Int J Cardiol,2014,174(1):174
[15]FÖrhécz Z,Gombos T,Borgulya G,et al.Red cell distribution width in heart failure:prediction of clinical events and relationship with markers of ineffective erythropoiesis,inflammation,renal function, and nutritional state[J].Am Heart J,2009,158(4):659
(2015-12-12收稿)
Association between RDW and atrial fibrillation recurrence after radiorequency catheter ablation in patients with paroxysmal non-valvular atrial fibrillation
LI Hong-liang,LIU Tong,XU Gang,LIU En-zhao,JIAO Zhan-quan,LI Guang-ping
(Department of Cardiology,The Second Hospital,Tianjin Medical University,Tianjin Key Laboratory of Ionic-Molecular Function of Cardiovascular Disease,Tianjin Institute of Cardiology,Tianjin 300211,China)
Objective:To investigate the association between red cell distribution width (RDW)and atrial fibrillation recurrence after radiofrequency catheter ablation in patients with paroxysmal non-valvular atrial fibrillation.Methods:73 patients with paroxysmal nonvalvular atrial fibrillation that undergoing ring plumonary vein radiofrequency catheter ablation were included.RDW,course of atrial fibrillation,left atrium diameter,unconjugated bilirubin,total bilirubin of all patients were carefully collected.Three months after the operation for the blank period was set up.The average follow-up period was(17±15)months.Recurrence was defined as recurrence of atrial fibrillation,atrial flutter,atrial tachycardia which lasted>30 s.Statistic data were analyzed by multiple Logistic regression.Results:Twenty-four patients had atrial fibrillation recurrence relapse.Recurrence group had higher preoperative RDW,bigger left atrial diameter, longer course of atrial fibrillation,higher unconjugated bilirubin,total bilirubin than non-recurrence group(P<0.05).Multivariate Logistic regression analysis showed that left atrial diameter,course of disease,RDW were independent risk factors for atrial fibrillation recurrence after radiofrequency catheter ablation.Conclusion:Left atrial diameter,course of atrial fibrillation,and RDW could be associated with recurrence of atrial fibrillation after radiofrequency catheter ablation in patients with paroxysmal non-valvular atrial fibrillation.
atrial fibrillation;red cell distribution width;radiofrequency ablation;recurrence
R541.7+5
A
1006-8147(2016)02-0104-03
李宏亮(1989-),男,硕士在读,研究方向:心血管疾病的基础与临床;通信作者:李广平,E-mail:tjcardiol@126.com。
