Relationship between urodynamic patterns and lower urinary tract symptoms in Chinese women with a non-neurogenic bladder
2016-04-27LinhuiWangCunzhouWangChuangyuQuLeiYinDanfengXuXingangCuiBingLiu
Linhui Wang,Cunzhou Wang,Chuangyu Qu*,Lei Yin*, Danfeng Xu,Xingang Cui,Bing Liu
Department of Urology,Changzheng Hospital,Second Military Medical University,Shanghai,China
ASIAN FOCUS
Relationship between urodynamic patterns and lower urinary tract symptoms in Chinese women with a non-neurogenic bladder
Linhui Wang1,Cunzhou Wang1,Chuangyu Qu*,Lei Yin*, Danfeng Xu,Xingang Cui,Bing Liu
Department of Urology,Changzheng Hospital,Second Military Medical University,Shanghai,China
Bladder outlet
obstruction;
Detrusor
underactivity;
Idiopathic detrusor
overactivity;
Idiopathic sphincter
overactivity;
Urodynamics
Objective:To investigate the urodynamic study(UDS)patterns,obstruction status, continence status,and their correlations among neurologically intact women with lower urinary tract symptoms(LUTS)through an epidemiological and logistic regression analyses.
Methods:We retrospectively analyzed the UDS data of 3265 neurologically intact women with LUTS(2002-2014).Five UDS patterns were identified:normo-active detrusor/sphincter(NA,or DSI,detrusor/sphincter intact),idiopathic detrusor overactivity(IDO),idiopathic sphincter overactivity(ISO),IDO+ISO,and detrusor underactivity(DUA).Analyses of UDS pattern distribution and stratification were performed(based on a modification of the European Urological Association-Madersbacher classification system),and their correlations with bladder outlet obstruction(BOO)and stress urinary incontinence(SUI)status were evaluated via logistic regression analysis.
Results:NA,IDO,IDO+ISO,ISO,and DUA were noted in 927(28.4%),678(20.8%),320(9.8%), 689(21.1%),and 651(19.9%)cases,respectively.Moreover,storage,storage+voiding,and voiding symptoms were noted in 62.4%,21.1%,and 16.5%cases,respectively,whereas BOO and SUI were observed in 12.1%and 29.0%cases,respectively.The risk factors for BOO included NA,IDO,ISO,and IDO+ISO,whereas the protective factors against BOO included storage symptoms,SUI,storage+voiding symptoms,and complaint duration within 1-12 months.NA was the only risk factor for SUI,whereas BOO,storage+voiding symptoms, IDO,and storage symptoms were protective factors for SUI.Conclusion:Five UDS patterns were identified among neurologically intact women with LUTS. Functional abnormalities of the detrusor and/or sphincter were the main causes of LUTS,and were correlated with the BOO or SUI status.Thus,the UDS pattern can provide additional information regarding the risk factors for BOO or SUI status,as compared to symptomatic typing.ⓒ2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
1.Introduction
A prior epidemiological study of lower urinary tract symptoms(LUTS)among 18,992 respondents in China indicated that 55.5%of adult women experienced LUTS,and that nocturia,urgency,and stress urinary incontinence(SUI) were the more prevalent conditions[1].Moreover,LUTS negatively affects the mental well-being of female patients,and its prevalence is known to increase with age;in fact,it has been found to affect up to 55%of elderly individuals in France,Germany,the UK,and the USA[2]. Neurologically intact male or female patients with LUTS may suffer from various urodynamic disorders or a combination of them,including normo-active detrusor/sphincter (NA),idiopathic detrusor overactivity(IDO),idiopathic sphincter overactivity(ISO),IDO+ISO,or detrusor underactivity(DUA)[3-5].In patients with disorders such as bladder outlet obstruction(BOO),SUI,and overactive bladder(OAB),LUTS can be further stratified into the following three categories:storage,voiding,and postmicturition symptoms.However,a secondary analysis of data from the EPIC study(a multinational population-based survey of 19,165 adults)indicated a marked overlap of storage,voiding,and postmicturition symptoms among men in general(n=7210)and among men with OAB symptoms (n=502);furthermore,men with OAB were more likely to experience multiple LUTS subtypes[6].Among the men with OAB symptoms(n=502),29.3%exhibited only storage symptoms(probably closely related to IDO),whereas the others exhibited voiding and/or postmicturition symptoms alone or in combination with storage symptoms[6].However,symptomatic evaluation alone is not very efficient for determining the treatment for LUTS.Hence,elucidation of the intrinsic nature of detrusor and/or sphincter dysfunction is vital.
These findings suggest that a comprehensive urologic assessment of male patients is needed,and such analysis should also be performed in female patients.In our center, comprehensive urodynamic study(UDS)is routinely performed in patients with LUTS who are unresponsive to medical treatment or in patients with more complex complaints.Moreover,a previous retrospective study developed a classification system for UDS patterns for elderly male patients with non-neurogenic LUTS,which can be used as a reference guideline for diagnosis and treatment[7].
In the present study,we focused on such UDS analyses among adult female patients with LUTS.Through the analysis of individualized UDS data,we aimed to obtain comprehensive information regarding the general and stratified distribution as well as the prevalence of various UDS patterns and their correlation with BOO or SUI status among neurologically intact adult female patients with LUTS by using the current International Continence Society (ICS)definitions[8].
Furthermore,urethral sphincter pseudodyssynergia or poor relaxation of the urethral sphincter,which is actually a surrogate symptom of non-neurogenic lower urinary tract dysfunction(LUTD)and is represented by ISO in the present study,can be identified using anal sphincter electromyography(EMG)[4,5].The functional status of the detrusor and sphincter(either overactive,normo-active,or underactive) can be classified according to the European Urological Association(EUA)-Madersbacher classification system for neurogenic LUTD[4],and such functional disorders may develop in either neurologically intact adult male or female patients[5,7,9,10].In the present study,we aimed to establish a modified version of the urodynamic pattern classification system for non-neurogenic LUTD based on this Madersbacher classification system for neurogenic LUTD.
2.Patients and methods
2.1.Creation of a urodynamic pattern classification system for non-neurogenic LUTS
Considering the absence of sphincter underactivity(SUA)in several guidelines,we established a UDS pattern classif ication system for patients with non-neurogenic LUTS, which was based on a modified version of the EUAMadersbacher classification system[4](Fig.1).In addition to the omission of three subtypes of SUA,we included detrusor/sphincter intact as a subtype of NA.
2.2.Subjects and criteria
We examined a total of 3265 women with LUTS from May 2002 to November 2014 who presented to the out-patient clinic or were hospitalized;of these,2085 directly visited the hospital from the community and 1180 we referred by tertiary centers.All the patients were of Chinese ethnicity, except for five Caucasian patients from Russia and Kazakhstan.Patients with occult or overt neuropathy (multiple sclerosis,multiple system atrophy,dementia, Parkinson’s disease,diabetes mellitus,cerebrovascular disorder,spinal cord injury,and other conditions),heavy pelvic organ prolapse,previous transurethral or pelvic surgery,and active urinary tract infection were excluded. Symptoms were stratified as storage symptoms, storage+voiding symptoms,and voiding symptoms;uncommon postmicturition symptoms were classified as voiding symptoms.Storage symptoms included increased micturition frequency,nocturia,urinary urgency,and urinary incontinence;voiding symptoms included slow or weak stream,hesitancy,and terminal dribble;and postmicturition symptoms included the sensation of incomplete emptying and postmicturition dribble[8].In addition to symptomatic stratification,female patients with LUTS were further stratified according to the extent of BOO(absence of BOO,mild BOO,and typical BOO),the extent of SUI(SUI and absence of SUI),age(18-39,40-59,60-79,or 80-97 years),and their first test date(2002-2006,2007-2010, and 2011-2014).The duration of their complaint(range 1-480 months)was subdivided into four quartiles(1-12, 12-36,36-72,and 72-480 months),and was used as an independent variable in subsequent logistic regression analysis.
Patients with NA,IDO,IDO+ISO,and ISO were treated with anti-muscarinic agents,α adrenergic antagonist,or baclofen(GABA-ergic[γ-aminobutyric acid]-agonist), respectively[7].Moreover,patients with DUA underwent a treatment regimen involving continuous indwelling catheterization without clamping of the draining tube,pyridostigmine bromide,baclofen,α-adrenergic antagonist,and decoctions of Chinese medicinal herbs,for 4-6 weeks[7]. Furthermore,transurethral incision of the bladder neck or sacral neuromodulation(InterStim therapy)could be attempted in patients who were unresponsive to the abovementioned treatments[11-13].The results of the treatment were monitored and carefully assessed.
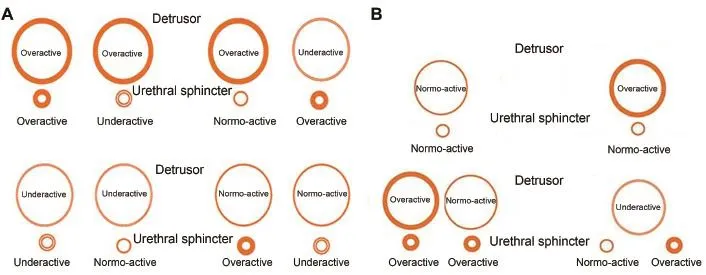
Figure 1Classification system of urodynamic patterns in neurogenic or non-neurogenic lower urinary tract dysfunction.(A) European Urological Association(EUA)-Madersbacher classification system of neurogenic lower urinary tract dysfunction.(B) Classification system for urodynamic patterns in patients with non-neurogenic LUTS based on a modified version of the EUAMadersbacher classification system.
2.3.Urodynamic study program
The UDS(Urovision Janus,Life Tech,USA;Solar,MMS,the Netherlands;and Andromeda,Germany)included maximum flow rate(free Qmax)assessment,filling cystometrography(CMG),voiding pressure-flow study(PFS), anal sphincter EMG,and urethral pressure profilometry (UPP)according to previously described techniques [5,9,14].The methods,definitions,and units used were based on the standards recommended by the ICS,except where specifically noted[8].CMG and PFS were performed by using an 8F dual lumen catheter(Xubu Medical Appliance Company,Dantu,Jiangsu,China),with the infusion of normal saline at a rate of 50 mL/min,after which bladder pressure(Pves)was recorded.Intra-abdominal pressure (Pabd)was recorded by using a 12F transrectal balloon catheter(Cook Urological Incorporated,IN,USA).Anal sphincter EMG was simultaneously recorded by two needleguided-wire electrodes placed at the 3 and 9 o’clock positions to the anus[5].After catheterization,the postvoid residual urine was evacuated and measured.Thereafter, CMG and PFS were completed with the patients sitting or squatting on a commode,with the uroflowmeter placed below,to collect the voided liquid.The maximum flow rate (Qmax)and detrusor pressure(Pdet=Pves-Pabd)were consecutively measured by asking the patient to void. Involuntary phasic or terminal detrusor overactivity was considered to indicate the presence of IDO[8].After the end of the UPP,the maximum urethral closure pressure and the functional profile length were recorded.The qualif ication and quantification of BOO were performed based on the female BOO standards of the Blaivas nomogram[15], whereas the ICS nomogram and Schaefer nomogram were also occasionally used.
NA was diagnosed based on the absence of a urodynamically visible detrusor and/or sphincter dysfunction during UDS. Theoretically,NA also includes certain types of bladder oversensitivity,such as type 1 OAB[16]or a condition that was previously described as sensory urgency[8,17].IDO was diagnosed based on the presence of urodynamically visible detrusor overactivity during UDS(either phasic or terminal).IDO includes type 2,3 and 4 OAB,or the conditionprevious described as motor urgency[8].IDO+ISO represented the simultaneous occurrence of IDO and ISO.A diagnosis of ISO was confirmed based on the presence of increased external sphincter activity during voluntary voiding,as indicated by increased sphincter activity with a sustained detrusor contraction during PFS or simply by a minus tense/loose(TL)value[9].DUA is defined as a contraction of reduced strength and/or duration that results in prolonged bladder emptying and/or a failure to achieve complete bladder emptying within a normal time span[8].
2.5.Study design
The study was approved by the local ethics committee,and all participants provided written informed consent.Our diagnosis and treatment program was first based on whether the detrusor was severed or intact,followed by the type of UDS pattern if a satisfactory PFS result was available,and then according to the five UDS patterns, particularly DUA,regardless of whether PFS results were available.The program has been mapped as a flowchart in Fig.2.
2.6.Statistical analysis
SPSS version 17.0(SPSS,Chicago,IL,USA)for Windows was used for statistical analysis.For all analyses,the variables are presented as patient number and percentage of the entire cohort.Categorical data were analyzed using the Chi-square test with Fisher’s exact probability test as appropriate,and each UDS pattern was compared with the other four patterns overall[18].A p value of<0.05 was considered statistically significant.
The likelihood of clinical progression to BOO or SUI was evaluated with the other clinical and UDS variables.In the binary logistic regression analysis,the formula was as follows:


Figure 2Study design,flow diagram,outcome,and treatment trends of neurologically intact female patients aged>18 years with LUTS.BPS/IC,bladder pain syndrome/interstitial cystitis;DUA,detrusor underactivity;IDO,idiopathic detrusor overactivity; ISO,idiopathic sphincter overactivity;NA,normo-active detrusor/sphincter;TURN,transurethral resection of the bladder neck; LUTS,lower urinary tract symptoms;UDS,urodynamic study.
Either BOO or SUI was used as the dependent variable (Y1 and Y2).β0remained constant in each formula.Theindependent variables were as follows:X1,patient age(4 dummy variables:18-39,40-59,60-79,and≥80 years); X2,test dates(3 dummy variables:2002-2006,2007-2010, and 2011-2014);X3,complaint durations(4 dummy variables:1-12 months,12-36 months,36-72 months,and 72-480 months);X4,symptomatic typing(3 dummy variables:storage symptoms,storage+voiding symptoms,and voiding symptoms);X5,UDS patterns(5 dummy variables: NA,IDO,IDO+ISO,ISO,and DUA);and X6,BOO(absence or presence,when SUI was the dependent variable)or SUI (absence or presence,when BOO was the dependent variable).
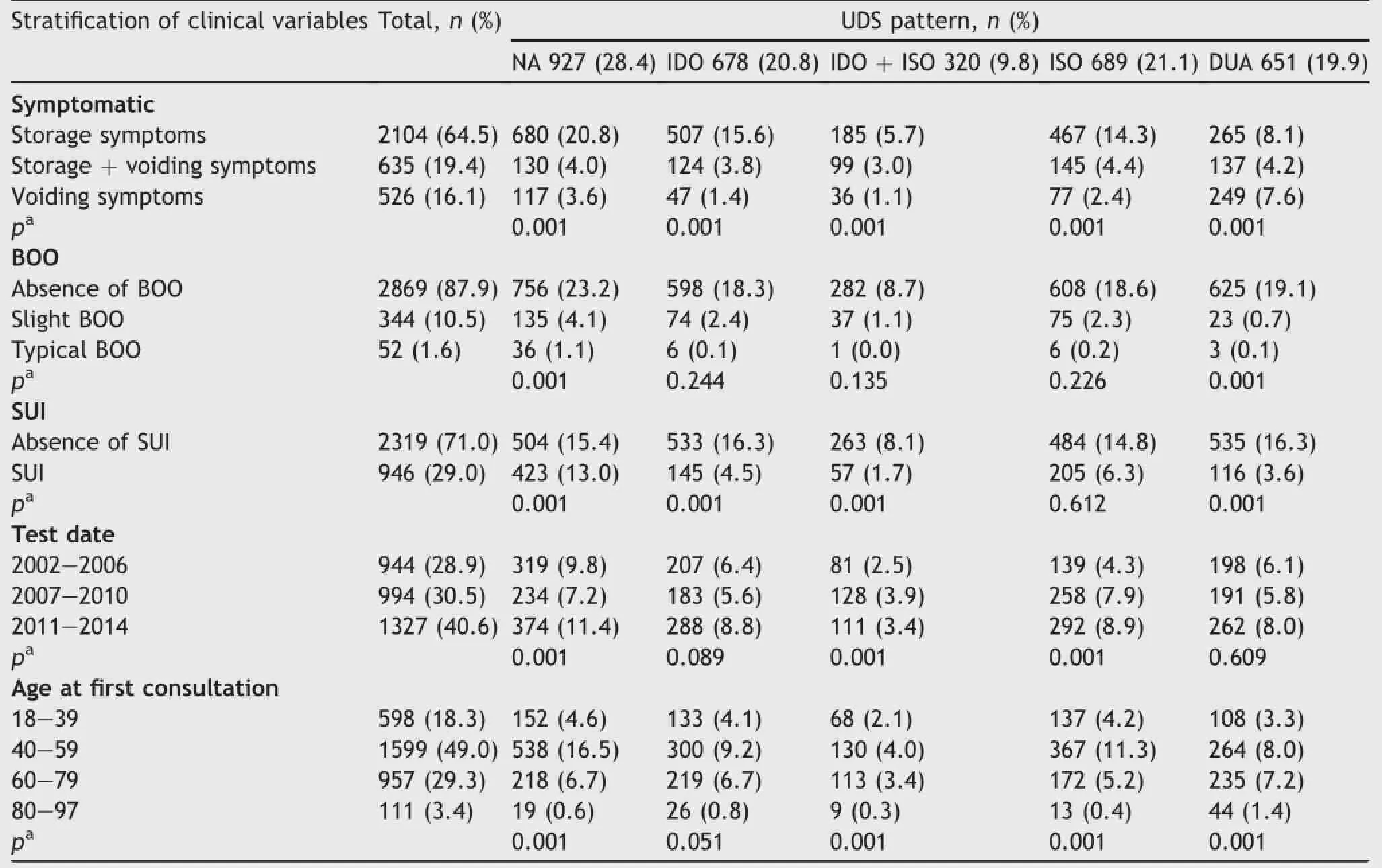
Table 1UDS pattern distribution of adult female patients neurologically intact with LUTS from 2002 to 2014.(n=3265).
3.Results
3.1.Distribution and stratification of UDS patternsAmong all the patients,NA,IDO,IDO+ISO,ISO,and DUA were observed in 927(28.4%),678(20.8%),320(9.8%),689 (21.1%),and 651(19.9%),respectively(Table 1 and Fig.3). Moreover,with regard to symptom distribution,storage, storage+voiding,and voiding symptoms were noted in 64.5%,19.4%,and 16.1%patients,respectively.In particular,BOO and SUI were observed in 12.1%and 29.0%patients,respectively.
由于目前的企业大多属于经营权和所属权背离,所以公司的董事会与监理会需要展现其应该具备的功能,对管理阶层开展的工作实施监管,严谨预防管理阶层造假,蒙蔽审计者,导致企业在信誉层面出现亏空,同时给公司长久的发展收益带来影响。另外作为企业的董事层,需要多加入企业的人才挑选与培养,重视公司财务近期的情况的时候,针对财务部门用人机制需要严格把控,严谨防止一人多岗,岗位不划分的状况出现。
An inter-pattern Chi-square analysis indicated that patients with storage symptoms were more likely to have NA, IDO,IDO+ISO,and ISO as compared to those with voiding symptoms or storage+voiding symptoms(p=0.001), whereas those with storage or voiding symptoms were more likely to have DUA as compared to patients with storage+voiding symptoms(p=0.001).Patients who did not have SUI were more likely to have NA,IDO,IDO+ISO, and DUA as compared to patients with SUI(p=0.001), whereas the likelihood of ISO was comparable in patients with and without SUI(p=0.612).
DUA is a general condition,and can be further subdivided into four subgroups according to sphincter function and abdominal strain type-namely,DUA1(DUA with sphincter synergia),DUA2(DUA with ISO and rectangularform abdominal strain),DUA3(DUA with sphincter synergia and gladiate-form strain),and DUA4(DUA with ISO and gladiate-form strain)(Fig.3).
3.2.Clinical variables and their correlations
The meaningful results of binary logistic regression,such as the β value(coefficient of regression),the Exp(β)(odds ratio)and its 95%confidence interval are summarized in Table 2.The risk factors for BOO(as Y1)included NA,IDO,ISO,and IDO+ISO,whereas the protective factors against BOO included storage symptoms,SUI,storage+voiding symptoms,and complaint duration within 1-12 months. Moreover,only NA was a risk factor for SUI(as Y2),whereas BOO,storage+voiding symptoms,IDO,and storage symptoms were protective factors against SUI(p=0.001).
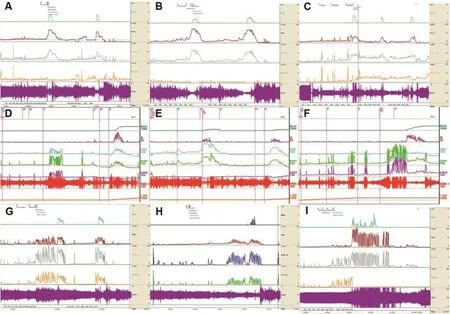
Figure 3Urodynamic patterns of neurologically intact adult female patients with LUTS:(A)normo-active detrusor/sphincter,or detrusor/sphincter intact(NA);(B)idiopathic detrusor overactivity with sphincter synergia(IDO);(C)idiopathic detrusor overactivity with idiopathic sphincter overactivity(IDO+ISO);(D)idiopathic sphincter overactivity with detrusor normo-activity(ISO); (E)NA with BOO;(F)DUA with sphincter synergia(DUA1);(G)DUA with ISO and rectangular-form strain(DUA2);(H)DUA with sphincter synergia and gladiate-form strain(DUA3);and(I)DUA with ISO and gladiate-form strain(DUA4).BOO,bladder outlet obstruction;DUA,detrusor underactivity;UDS,urodynamic study.
3.3.Results of treatment for different UDS patternsThe primary therapy chosen for patients with different UDS patterns depended on the UDS pattern;those with IDO,ISO, IDO+ISO,or even NA were treated with anti-muscarinic agents,α-adrenergic antagonist,or baclofen(Fig.2). Approximately 65%of patients exhibited a good response to their primary therapy;the regimen was changed in the patients who had a poor response.Patients with pelvic pain and poor treatment response were treated according to guideline of bladder pain syndrome/interstitial cystitis (BPS/IC)[19].Finally,five refractory cases required sacral neuromodulation therapy.Patients with both BOO or SUI underwent transurethral resection of the bladder neck (TURN)or sling procedure[9,20],whereas those with DUA underwent a specific DUA regimen over 4-6 weeks.If no response to treatment was noted,sacral neuromodulation or TURN was applied.
In 2004,2009,and 2014,the DUA regimen was applied to three cases with a large residual urine volume (2500-2800 mL)that potentially had an iatrogenic origin, and excellent results were achieved(Fig.4).The ages of these patients ranged from 33 to 61 years,and the complaint duration was<1 month in all cases.Sphincter synergia or relaxation during the voiding phase despite the persistent absence of detrusor contraction was a predictive factor of DUA,and was exhibited by one patient during thefirst consultation(Fig.4G)and by the other two patients during the follow-up assessments(Fig.4B,E).
4.Discussion
Based on the results of our epidemiological research,we identified five UDS patterns among neurologically intact adult female patients with LUTS.Although 28.4%of the patients exhibited NA,nearly 70%of these patients had detrusor and/or sphincter dysfunction.We believe that this distribution should not be overlooked.Considering that 55.5%of adult women in China suffer from LUTS[1],theincidence of each pattern of detrusor and/or sphincter dysfunction would be high.However,there were no significant differences in the prevalence of IDO,IDO+ISO,or ISO between patients with mild or typical BOO and those without BOO.Moreover,logistic regression analysis indicated that these three patterns and NA were risk factors for BOO.Hence,even though UDS is an optional test in patients with LUTS in most Western countries,the pathological conclusions underlying the UDS findings should not be ignored.Logistic regression analysis is an important multivariable prediction model for determining individual prognosis or diagnosis,and the results can indicate whether further tests are needed,can be used to directly initiate treatment,and can help reassure patients that their symptoms may not likely have a serious cause[21].
According to an American Urological Association(AUA)-commissioned survey,only 11%of urologists routinely performed UDS when evaluating a“benign prostatic hyperplasia(BPH)patient”in 1995[22].In 2014,in a total of 3494 new BPH patients,the rate of application of UDS at the initial BPH evaluation was only 5.4%[23].Among female patients with LUTS,Haylen et al.[24]noted that the rate of UDS was also low,and hence,voiding difficulty may have been overlooked as a diagnosis in comparison with urodynamic SUI,OAB or uterovaginal prolapse.In particular,the authors noted that 39%of patients who were referred for an initial urogynecological assessment,including UDS,had reported voiding difficulty.In the present study,the prevalence rates of mild and typical BOO were 10.5%and 1.6% of the whole population(12.1%in total).Furthermore,we should not only consider anatomic obstruction,but also functional obstruction.Although several investigators believe that UDS,which is an invasive and expensive test (~USD 500 in the USA in 2013[20]),is not routinely warranted[22],it is important to investigate the abnormal characteristics in patients suffering from various types of LUTS.CMG and PFS,along with simultaneous EMG,can help identify IDO,ISO,DUA,SUI,or BOO.In addition to good quality equipment and operator experience,patience and awareness of the operator are also important to determine these pathological results.Moreover,the potential for surgical intervention among patients with an intact detrusor should also be considered,and it is essential to validate their functional status in order to not only improve or relieve their symptoms,but to cure them.Accordingly,a balance should be maintained between reducing medical expenses and ensuring necessary examination in these patients.
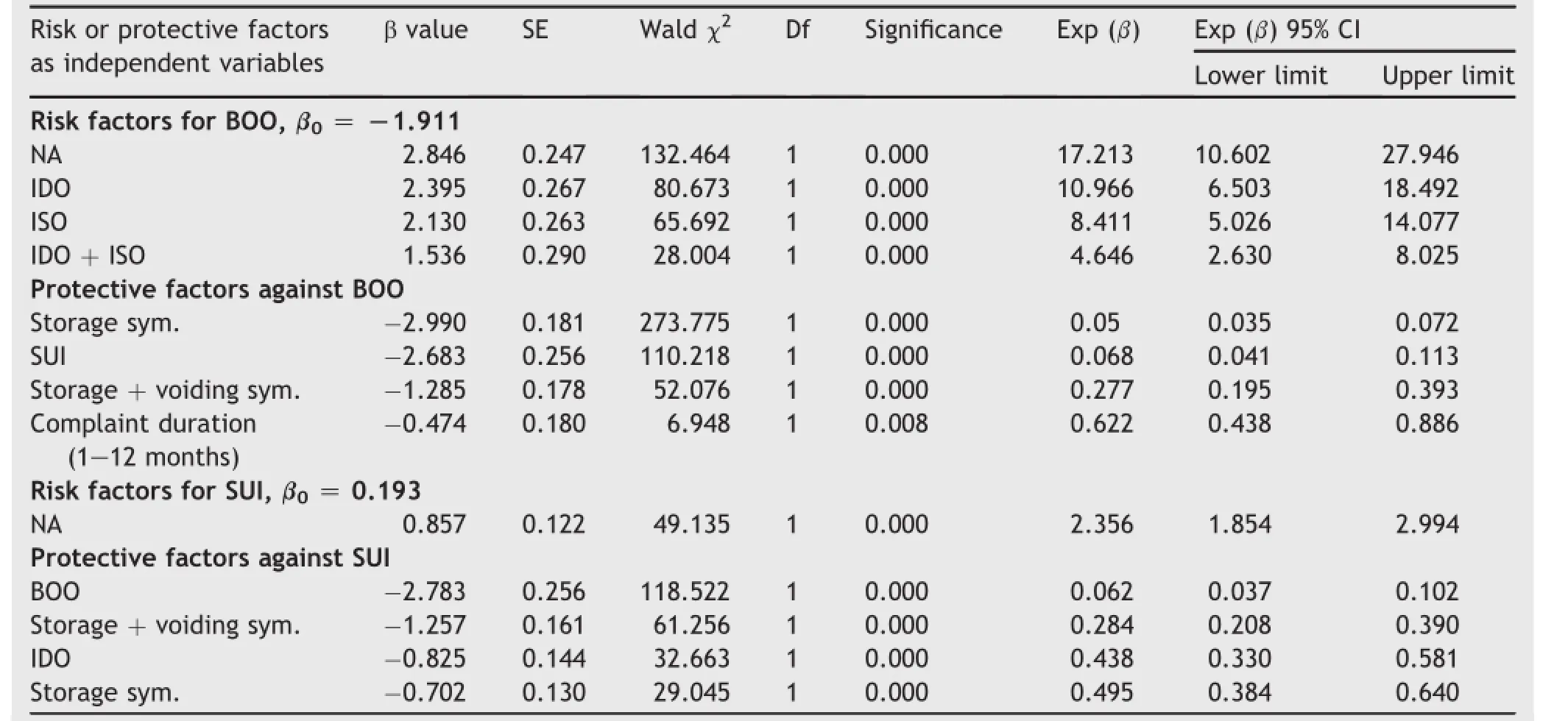
Table 2Independent variable risk and protective factors for or against BOO or SUI as dependent variables by binary logistic regression analysis in adult female patients neurologically intact with LUTS from 2002 to 2014(n=3265).
To our knowledge,the definition of SUA is not clearly provided in the literature.In the 2002 guideline of the ICS, intrinsic sphincter deficiency has been referred to as“urethral relaxation incontinence”,which should be validated by UPP[8],and is representative of SUA.Based on CMG,PFS,and EMG findings,the presence of“uninhibited sphincter relaxation”on EMG tracing during the storage phase also indicates the presence of SUA.However,thisfinding is rarely observed in patients with severe incontinence and is never noted in patients with neurogenic lesions.At our institute,the definition of DUA and its reversibility involves a 2-phase procedure,including UDS at the initial consultation,followed by reexamination at 4-6 weeks after undergoing a strict DUA regimen.This method of measurement and therapy is a novel non-standardized approach,and it is considered that patients with DUA will obtain useful results after undergoing this program[25,26].
ISO,which has also been termed as dysfunctional voiding,pseudodyssynergia,non-neurogenic neurogenic bladder,Hinman syndrome,Fowler’s syndrome or learnedvoiding dysfunction[5,27],is a type of non-neurogenic LUTD involving the simultaneous contraction of the detrusor and sphincter during the voiding phase.It has been described using a digitalization term-the TL value[12].In the guidelines for children,dysfunctional voiding is restricted to malfunction during the voiding phase only and does not include the storage phase[28].Hence,this concept should be improved.In the present study,ISO or IDO induced storage symptoms in 14.3%or 15.6%of patients,which appear to be higher than the rates for storage+voiding or voiding symptoms.Sacco and Bientinesi described preliminary data supporting the rational for using GABA analogs such as gabapentin and pregabalin in neurogenic or non-neurogenic IDO[29].Wang et al.[30] indicated that the high prevalence of symptoms is not equivalent to the severity of patient discomfort.Hence, efforts should be made to improve public and professional education,and further assessment of discomfort is required before initiating a medical intervention.The pain caused by BPS/IC is often obscure and is likely to be erroneously identified as urgency in mild cases.Moreover,it is difficult to distinguish such pain from OAB,vulvodynia,irritable bowel syndrome,endometriosis,and fibromyalgia[31]. However,these abnormalities may be related to functional somatic syndrome[32].Functional somatic syndrome may be defined as“physical symptoms that cannot be explained in terms of a conventionally defined disease,or appearing in patients who do not have proportional tissue abnormalities or pathologically defined changes in tissue that designate medical conditions”[32].Its symptoms cannot be explained by organ pathology,and there are currently no definitive diagnostic tests.Compared with PBS/IC,OAB is more likely to represent a type of functional somatic syndrome.UDS can be used to explore the intrinsic mechanism underlying the symptoms of pelvic pain,urgency,and other lower urinary tract-and pelvic floor-associated disorders.
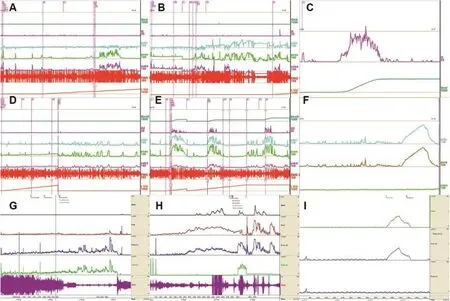
Figure 4Urodynamic image data of three neurologically intact adult female patients with acute urinary retention and residual urine volume of>2500 mL:(A)Case 1 includes a 49-year-old woman who presented with DUA4 at the first consultation;(B) Following the application of the DUA regimen for 4 weeks,Case 1 showed voiding failure during follow-up,after which the catheter was removed and fluent voiding was noted;(C)Flowmetry curve of Case 1 at 1 month after the CMG-PFS tests;(D)Case 2 includes a 33-year-old woman who presented with DUA4 at the first consultation;(E)After the DUA regimen was followed for 8 weeks,Case 2 showed disappearance of the DUA,recovery of micturition,and occasional IDO and ISO during the follow-up;(F)UPP test curves of Case 2 at the first consultation;(G)Case 3 includes a 61-year-old woman who presented with DUA1 at the first consultation;(H) After undergoing the DUA regimen for 5 weeks,Case 3 showed disappearance of the DUA,recovery of micturition,and occasional ISO during the follow-up;(I)UPP test curves of Case 3 at the first consultation.DUA,detrusor underactivity;UPP,urethral pressure profilometry.
This study is a long-term clinical retrospective assessment conducted in a single center.Although BOO and SUI were considered,diagnosed,and stratified according to the UDS patterns,the description of the therapy and follow-up details were beyond the scope of the study and were hence not included.Moreover,although video urodynamics was not conducted and vesico-ureteral backflow,hydroureter, or hydronephrosis were not identified,three types ofmodern UDS systems were used during the 13-year period, and the obstruction at the external sphincter level was displayed as precisely as that on video UDS[3].Moreover, we observed the influence of psychological and emotional factors on the function of the lower urinary tract;however, this influence cannot be recorded in a very objective manner considering the lack of appropriate methods.The external urethral sphincter may be overactive,normal,or underactive.In the guideline for neurogenic LUTD proposed by the EAU,neurogenic LUTD was further categorized into eight subgroups[4];however,in our patients who were neurologically intact,it was difficult to identify and define SUA by using CMG,PFS,and EMG,and hence,this term is avoided in the nomenclature of UDS patterns for adult female patients with LUTS(Fig.1B).
5.Conclusion
We established a classification system for the urodynamic patterns in patients with non-neurogenic LUTS based on a modified version of the EUA-Madersbacher classification system.Among the neurologically intact adult female patients with LUTS,we identified five UDS patterns,including NA,IDO,IDO+ISO,ISO,and DUA.The UDS data were found to be very useful for the diagnosis and treatment of these patients.The risk factors for BOO included NA,IDO,ISO, and IDO+ISO,whereas the protective factors against BOO included storage symptoms,SUI,storage+voiding symptoms,and complaint duration within 1-12 months.Only NA was a risk factor for SUI,whereas the protective factors against SUI were BOO,storage+voiding symptoms,IDO, and storage symptoms.Thus,UDS patterns provide more information regarding the risk factors for BOO or SUI status as compared to symptomatic typing.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgments
The authors would like to thank Zhilian Min,Youhua Zhu, Yacheng Yao,Jizhong Ren,Yushan Liu,and Yi Gao for their outstanding efforts in data management;Zixing Zhang for the development of decoction of Chinese medicinal herbs; Xingyi Zhang for the help with image creation;Wei Qian and Jin Wang for help with statistical analysis;and Cheng Zhong,Yana Liu and Xingwei Liu for their constant technical support.
[1]Zhang L,Zhu L,Xu T,Lang JH,Li ZA,Gong J,et al.A population-based survey of the prevalence,potential risk factors,and symptom-specific bother of lower urinary tract symptoms in adult Chinese women.Eur Urol 2015;68:97-112.
[2]Abrams P,Smith AP,Cotterill N.The impact of urinary incontinence on health-related quality of life(HRQoL)in a realworld population of women aged 45-60 years:results from a survey in France,Germany,the UK and the USA.BJU Int 2015; 115:143-52.
[3]Kuo HC.Videourodynamic characteristics and lower urinary tract symptoms of female bladder outlet obstruction.Urology 2005;66:1005-9.
[4]Sto¨hrer M,Blok B,Castro-Diaz D,Chartier-Kastler E,del Popolo G,Kramer G,et al.EAU guidelines on neurogenic lower urinary tract dysfunction.Eur Urol 2009;56:81-8.
[5]Qu CY,Xu DF,Wang CZ,Chen J,Yin L,Cui X.Anal sphincter electromyogram for dysfunction of lower urinary tract and pelvic floor.In:Mizrahi J,editor.Advances in applied electromyography.Rijeka:InTech;2011.p.161-88.
[6]Irwin DE,Milsom I,Kopp Z,Abrams P,Artibani W,Herschorn S. Prevalence,severity,and symptom bother of lower urinary tract symptoms among men in the EPIC study:impact of overactive bladder.Eur Urol 2009;56:14-20.
[7]Xu DF,Cui XG,Qu CY,Yin L,Wang CZ,Chen J.Urodynamic pattern distribution among aged male patients with lower urinary tract symptoms suggestive of bladder outlet obstruction.Urology 2014;83:563-9.
[8]Abrams P,Cardozo L,Fall M,Griffiths D,Rosier P,Ulmsten U, et al.The standardisation of terminology of lower urinary tract function:report for the Standardisation Sub-committee of the International Continence Society.Neurourol Urodyn 2002;21:167-78.
[9]Xu DF,Qu CY,Meng H,Ren JZ,Zhu YH,Min ZL,et al. Dysfunctional voiding confirmed by transdermal perineal electromyography,and its effective treatment with baclofen in women with lower urinary tract symptoms:a randomized double-blind placebo-controlled crossover trial.BJU Int 2007; 100:588-92.
[10]Qu CY,Xu DF.Comprehensive urodynamics:being devoted to clinical urologic practice.World J Clin Urol 2014;3:96-112.
[11]Zhang P,Wu ZJ,Xu L,Yang Y,Zhang N,Zhang XD.Bladder neck incision for female bladder neck obstruction:long-term outcomes.Urology 2014;83:762-7.
[12]Jhang JF,Jiang YH,Kuo HC.Transurethral incision of the bladder neck improves voiding efficiency in female patients with detrusor underactivity.Int Urogynecol J 2014;25:671-6.
[13]Peeters K,Sahai A,De Ridder D,Van der Aa.Long-term followup of sacral neuromodulation for lower urinary tract dysfunction.BJU Int 2014;13:789-94.
[14]Xu DF,Zhang S,Wang CZ,Li J,Qu CY,Cui XG,et al.Lowfrequency electrotherapy for female patients with detrusor underactivity due to neuromuscular deficiency.Int Urogynecol J 2012;23:1007-15.
[15]Blaivas JG,Groutz A.Bladder outlet obstruction nomogram for women with lower urinary tract symptomatology.Neurourol Urodyn 2000;19:553-64.
[16]Blaivas JG,Chancellor MB,Weiss J,Verharren M.Atlas of urodynamics.Glossary and abbreviations.2nd ed.Blackwell Publishing;2007.p.7.
[17]Haylen BT,de Ridder D,Freeman RM,Swift SE,Berghmans B, Lee J,et al.An International Urogynecological Association (IUGA)/International Continence Society(ICS)joint report on the terminology for female pelvic floor dysfunction.Int Urogynecol J 2010;21:5-26.
[18]Chen SF,Jiang YH,Jhang JF,Lee CL,Kuo HC.Bladder management and urological complications in patients with chronic spinal cord injuries in Taiwan.Tzu Chi Med J 2014;26:25-8.
[19]Biers S,Thiruchelvam N.Bladder pain syndrome:contemporary management and future strategies.J Clin Urol 2014;7: 8-19.
[20]Nager CW,Brubaker L,Litman HJ,Zyczynski HM,Varrer E, Amundsen C,et al.A randomized trial of urodynamic testing before stress-incontinence surgery.N Engl J Med 2012;366: 1987-97.
[21]Collins GS,Reitsma JB,Altman DG,Moons KGM.Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis(TRIPOD):the TRIPOD Statement.Eur Urol 2015;67:1142-51.
[22]Mc Connell JD.Why pressure-flow studies should be optional and not mandatory studies for evaluating men with benign prostatic hyperplasia?Urology 1994;44:156-8.
[23]Auffenberg GB,Gonzalez CM,Wolf JS,Clemens JQ,Meeks W, McVary KT.An observational analysis of provider adherence to AUA guidelines on the management of benign prostatic hyperplasia.J Urol 2014;192:1483-8.
[24]Haylen BT,Krishnan S,Schulz S,Verity L,Law M,Zhou J,et al. Has the true prevalence of voiding difficulty in urogynecology patients been underestimated?Int Urogynecol J 2007;18: 53-6.
[25]Andersson KE.Bladder underactivity.Eur Urol 2014;65: 399-401.
[26]Osman NI,Chapple CR,Abrams P,Dmochowski R,Haab F, Nitti V,et al.Detrusor underactivity and the underactive bladder:a new clinical entity?A review of current terminology,definitions,epidemiology,aetiology,and diagnosis.Eur Urol 2014;65:389-98.
[27]Hinman Jr F.Nonneurogenic neurogenic bladder(the Hinman syndrome)-15 years later.J Urol 1986;136:769-77.
[28]Neve´us T,von Gontard A,Hoebeke P,Hjalmas K,Bauer S, Bower W,et al.The standardization of terminology of lower urinary tract function in children and adolescents:report from the Standardization Committee of the International Children’s Continence Society.J Urol 2006;176:314-24.
[29]Sacco E,Bientinesi R.Innovative pharmacotherapies for women with overactive bladder:where are we now and what is in the pipeline?Int Urogynecol J 2015;26:629-40.
[30]Wang YL,Hu H,Xu KX,Wang XF,Na YQ,Kang XP.Prevalence, risk factors and the bother of lower urinary tract symptoms in China:a population-based survey.Int Urogynecol J 2015;26: 911-9.
[31]Warren JW,Diggs C,Horne L,Greenberg P.Interstitial cystitis/painful bladder syndrome:what do patients mean by“perceived”bladder pain?Urology 2011;77:309-12.
[32]Warren JW.Bladder pain syndrome/interstitial cystitis as a functional somatic syndrome.J Psychosom Res 2014;77: 510-5.
Received 18 August 2015;received in revised form 9 October 2015;accepted 19 November 2015
Available online 2 December 2015
*Corresponding authors.
E-mail addresses:qu_cy@sohu.com(C.Qu),yin202@163.com(L.Yin).
Peer review under responsibility of Shanghai Medical Association and SMMU.1These authors contributed equally to this study.
http://dx.doi.org/10.1016/j.ajur.2015.11.004
2214-3882/ⓒ2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
猜你喜欢
杂志排行

Asian Journal of Urology的其它文章
- PMEPA1 guards against TGF-β-mediated prostate cancer bone metastasis
- Elevated preoperative neutrophil-tolymphocyte ratio may be associated with decreased overall survival in patients with metastatic clear cell renal cell carcinoma undergoing cytoreductive nephrectomy
- Prostate cancer volume associates with preoperative plasma levels of testosterone that independently predicts high grade tumours which show low densities(quotient testosterone/tumour volume)
- Zoledronic acid combined with androgendeprivation therapy may prolong time to castration-resistant prostate cancer in hormone-naïve metastatic prostate cancer patients-A propensity scoring approach
- Can intravesical prostatic protrusion predict bladder outlet obstruction even in men with good flow?
- Who needs further evaluations to diagnose upper urinary tract urothelial cancers among patients with abnormal findings by enhanced CT?