The use of the greater trochanter marker in the thigh segment model: Implications for hip and knee frontal and transverse plane motion
2016-04-25ValentinaGraciGretchenSalsichDepartmentofNeurologyUniversityofMarylandSchoolofMedicineBaltimoreMD21201USAPrograminPhysicalTherapySaintLouisUniversityBaltimoreMD63104USAReceived15April2014revised26August2014accepted28Sept
Valentina Graci*,Gretchen B.SalsichDepartment of Neurology,University of Maryland School of Medicine,Baltimore,MD 21201,USAProgram in Physical Therapy,Saint Louis University,Baltimore,MD 63104,USAReceived 15 April 2014; revised 26 August 2014; accepted 28 Septemer 2014 Availale online 20 January 2015
The use of the greater trochanter marker in the thigh segment model: Implications for hip and knee frontal and transverse plane motion
Valentina Gracia,*,Gretchen B.SalsichbaDepartment of Neurology,University of Maryland School of Medicine,Baltimore,MD 21201,USA
bProgram in Physical Therapy,Saint Louis University,Baltimore,MD 63104,USA
Received 15 April 2014; revised 26 August 2014; accepted 28 September 2014 Available online 20 January 2015
Peer review under responsibility of Shanghai University of Sport.
* Corresponding author.
E-mail address: vgraci@som.umaryland.edu (V.Graci).
http://dx.doi.org/10.1016/j.jshs.2015.01.002
2095-2546/©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.
Abstract
Background: The greater trochanter marker is commonly used in 3-dimensional (3D) models; however,its influence on hip and knee kinematics during gait is unclear.Understanding the influence of the greater trochanter marker is important when quantifying frontal and transverse plane hip and knee kinematics,parameters which are particularly relevant to investigate in individuals with conditions such as patellofemoral pain,knee osteoarthritis,anterior cruciate ligament (ACL) injury,and hip pain.The aim of this study was to evaluate the effect of including the greater trochanter in the construction of the thigh segment on hip and knee kinematics during gait.
Methods: 3D kinematics were collected in 19 healthy subjects during walking using a surface marker system.Hip and knee angles were compared across two thigh segment definitions (with and without greater trochanter) at two time points during stance: peak knee flexion (PKF) and minimum knee flexion (MinKF).
Results: Hip and knee angles differed in magnitude and direction in the transverse plane at both time points.In the thigh model with the greater trochanter the hip was more externally rotated than in the thigh model without the greater trochanter (PKF:−9.34°±5.21°vs.1.40°±5.22°,MinKF:−5.68°±4.24°vs.5.01°±4.86°; p<0.001).In the thigh model with the greater trochanter,the knee angle was more internally rotated compared to the knee angle calculated using the thigh definition without the greater trochanter (PKF: 14.67°±6.78°vs.4.33°±4.18°,MinKF: 10.54°±6.71°vs.−0.01°±2.69°; p<0.001).Small but significant differences were detected in the sagittal and frontal plane angles at both time points (p<0.001).
Conclusion: Hip and knee kinematics differed across different segment definitions including or excluding the greater trochanter marker,especially in the transverse plane.Therefore when considering whether to include the greater trochanter in the thigh segment model when using a surface markers to calculate 3D kinematics for movement assessment,it is important to have a clear understanding of the effect of different marker sets and segment models in use.
©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.
Keywords:3D motion analysis; Thigh segment model; Transverse plane motion
1.Introduction
In gait analysis using surface marker systems,the greater trochanter (GT) has been employed as a bony landmark for the orientation of the thigh segment,1,2and it is still commonly used.3-9However,some authors found poor intra- and interrater precision in the identification of the GT.10Inaccuracies in defining the GT position for the definition of the anatomical frame of reference of the thigh were found to cause variability in hip and knee joint kinematics across different estimated GT positions.10,11
Understanding the influence of GT marker on biomechanical calculations derived from hip and knee models is important when quantifying frontal and transverse plane hip and knee kinematics,parameters which are particularly relevant to investigate in individuals with conditions such as patellofemoral pain,knee osteoarthritis,anterior cruciate ligament (ACL) injury,and hip pain.The frontal and transverse plane motionof the hip and knee joints during gait is small,hence small differences across hip and knee models could lead to different or misleading clinical conclusions.For example,one model might reveal excessive hip internal rotation or knee valgus while another might not.This issue is particularly relevant when making clinical judgments on lower limb alignment in individuals with patellofemoral pain for the presence of dynamic knee valgus (i.e.,excessive hip adduction and internal rotation,and knee abduction and external rotation) which is a proposed mechanism for patellofemoral pain.12Furthermore the GT marker included or excluded in the thigh definition may also have different effects on the knee angles.These effects may impact clinical judgments based on knee angles when examining individuals with knee pain or ACL injury.
The effect of the GT marker included vs.excluded in the thigh segment on both hip and knee angles is still unclear.Therefore the scope of this study was to evaluate the effect of including the GT in the construction of the thigh segment on hip and knee kinematics during gait.In the present study,we compared hip and knee angles using two thigh segment definitions (with and without GT) during walking.
Because the GT marker is used to define the orientation of the frontal plane of the thigh,we hypothesized that the GT would influence the magnitude and direction of hip and knee transverse plane angles to a greater extent than sagittal and frontal plane angles.
2.Methods
2.1.Participants
Nineteen subjects (10 males),with age 27.19±5.66 years,height 1.70±0.05 m,mass 71.41±9.44 kg,and body mass index 24.57±2.89 kg/m2(mean±SD) participated in this study.Subjects reported no unresolved or recent musculoskeletal injuries,surgeries,or pain.The study was approved by the Institutional Review Board of Saint Louis University and all subjects read and signed an informed consent form before participating.The dominant leg was assessed by asking subjects which leg they would kick a ball with.13All subjects were right leg dominant.
2.2.Procedures
Kinematic data were collected (120 Hz) using an 8-camera 3-dimensional (3D) motion capture system (Vicon Nexus,Oxford,UK).Reflective markers were placed on: iliac crests,anterior and posterior superior iliac spines,the medial and lateral femoral epicondyles (approximating the knee flexion/extension axis),GTs (superior aspect),medial and lateral malleoli (approximating the ankle flexion/extension axis) (Fig.1A).Quadrangular clusters with four markers on each were placed on thighs and shanks.The markers on the GTs,femoral epicondyles,and malleoli were removed after calibration (Fig.1A).Subjects performed three walking trials on a 7-m walkway using their customary speed (mean 1.41 m/s).Data were collected in one session.

Fig.1.(A) Schematic of the marker placements.Black points represent the markers that were used only for tracking the segment movement during walking.Red points represent the markers that were used also in the calibration trial for the construction of the 6-degree-of-freedom model.The markers on the greater trochanters (GT),femoral epicondyles,and malleoli were removed after calibration.(B) Schematic of the thigh and shank segment definitions and the hip and knee models used.
2.3.Data analysis
Visual3D (C-Motion,Inc.,Germantown,MD,USA) was used to construct a 6-degree-of-freedom model that incorporated the pelvis,thigh,and shank segments.For the pelvis the CODA model (Charnwood Dynamics Ltd.,Leicestershire,UK) was used.The coordinates of the hip joint center were calculated according to the Bell’s method14,15as a percentage of the distance between anterior superior iliac spines (i.e.,36% in the sagittal plane,19% in the frontal plane,and 30% in the transverse plane).We defined two thigh segments: 1)Thigh_without GT,where the frontal plane was defined by the hip joint center and femoral epicondyles,and 2) Thigh_GT,where the frontal plane was defined by the GT,hip joint center,and femoral epicondyles (i.e.,a plane is fit to the four markers so that the sum of the squared distances between the targets and the frontalplane is minimized).We defined a shank segment where the frontal plane definition included the femoral epicondyles and the midpoint between the malleoli as the proximal and distal end respectively.For the thigh and shank segments,the frontal plane defined the orientation of the X axis.The Z axis passed through the midpoints of the proximal and distal endpoints of the segments.TheY axis was orthogonal to both X and Z axes.
Data were collected and processed inVicon for marker labelling and in Visual3D to apply the 6-degree-of-freedom model.Marker trajectories were lowpass filtered (6 Hz,4th order Butterworth filter) and joint angles were calculated using a Cardan sequence of rotations (X medial-lateral direction,Y anterior-posterior direction,Z vertical direction) in Visual3D.The data were not normalized to the standing calibration.Data were then imported in Matlab R2010b (The MathWorks,Inc.,Natick,MA,USA).For each trial,one stride of each subject’s right leg was used for the analysis.
Two time events relevant in weight bearing tasks were selected: peak knee flexion (PKF) during the initial stance phase and minimum knee flexion (MinKF) before toe off.PKF approximates the point of maximal knee joint loading and MinKF approximates the point of full knee extension or “locking”.These two time points are important when investigating movement patterns in people with ACL injuries and patellofemoral pain.PKF and MinKF were calculated as a percentage of the gait cycle for each individual model.Between models,the time points differed by less than 0.1%.The dependent measures were the hip and knee angles calculated at PKF and MinKF in three planes (sagittal,frontal,and transverse).Angles were expressed in the reference frame of the proximal segment.Positive values represent flexion,adduction,and internal rotation.Dependent measures were averaged across repetitions.Using the data collected on Day 1,paired t test were performed comparing the hip angles calculated using the two thigh segment models: Hip_noGT (the angle defined by Thigh_without GT relative to pelvis) and Hip_GT (the angle defined by Thigh_GT relative to pelvis) (Fig.1B).Paired t test were also used to compare the knee angles calculated using the two thigh segments: Knee_noGT (the angle defined by the shank relative to Thigh_without GT) and Knee_GT (the angle defined by the shank relative to Thigh_GT),(Fig.1B).The Bonferroni-corrected α level was set at p≤0.004 (= 0.05/12) to account for the number of comparisons.Between-day intrarater reliability of the hip and knee angles was calculated using the intraclass correlation coefficient ICC(3,3).Data on 15 subjects were collected on two occasions,averaging 4.52±1.89 days apart.The ICCs were used to estimate the standard error of measurement (SEM).
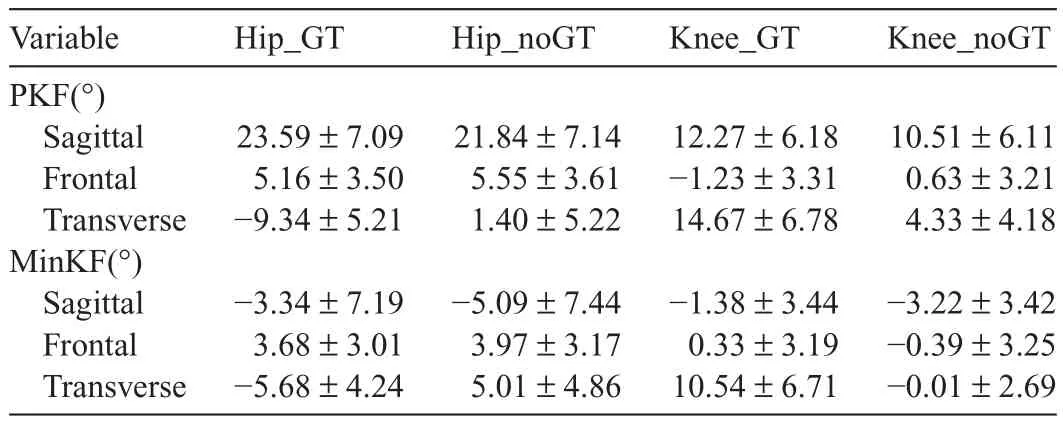
Table 1Hip_GT,Hip_noGT,Knee_GT,and Knee_noGT represent the hip and knee angles with the thigh model that includes and excludes GT.(mean±SD).
3.Results

Fig.2.Hip and knee angles at peak knee flexion (PKF) (A,C) and minimum knee flexion (MinKF) (B,D) in the three plane of motion (X sagittal,Y frontal,Z transverse) (mean±SD).Positive values represent flexion,adduction,and internal rotation.*p<0.05.
All hip and knee angles differed between conditions (GT vs.NoGT) at both time points (Table 1,Fig.2).In the transverse plane at both time points,Hip_GT was in greater external rotation compared to Hip_noGT (PKF:−9.34°±5.21°vs.1.40°±5.22°,MinKF:−5.68°±4.24°vs.5.01°±4.86°;p<0.001),whereas Knee_GT was in greater internal rotation compared to Knee_noGT (PKF: 14.67°±6.78°vs.4.33°±4.18°,MinKF: 10.54°±6.71°vs.−0.01°±2.69°; p<0.001).Abbreviations: SEM°= standard error of measurements; GT = greater trochanter; ICC = intraclass correlation coefficient; PKF = peak knee flexion; MinKF = minimum knee flexion during the stance phase.

Table 2Between-day reliability and SEM°of the kinematics variables.
In the sagittal plane,Hip_GT was in greater flexion at PKF and less extension at MinKF compared to Hip_noGT (PKF: 23.59°±7.09°vs.21.84°±7.14°,MinKF:−3.34°±7.19°vs.−5.09°±7.44°; p<0.001).Knee_GT also was in greater flexion at PKF and less extension at MinKF compared to Knee_noGT (PKF: 12.27°±6.18°vs.10.51°±6.11°,MinKF: −1.38°±3.44°vs.−3.22°±3.42°; p<0.001).
In the frontal plane at both time points,Hip_GT was in less adduction compared to Hip_noGT (PKF: 5.16°±3.50°vs.5.55°±3.61°,MinKF: 3.68°±3.01°vs.3.97°±3.17°; p<0.001).Knee_GT was in greater abduction (valgus) at PKF(−1.23°±3.31°vs.0.63°±3.21°,p<0.001) and in greater adduction (varus) at MinKF (0.33°±3.19°vs.−0.39°±3.25°,p = 0.001) compared to Knee_noGT.The hip and knee angles had good-to-excellent reliability (ICC(3,3)>0.65)16and low SEM (Table 2).
4.Discussion

Fig.3.Time series curves of the hip (A-C) and knee angles (D-F) in the three plane of motion normalized as % stride cycle and averaged across subjects.The black thick bars represent the time points corresponding to peak knee flexion (PKF) and minimum knee flexion (MinKF).Thick lines represent the means.Error bars represent the SD at each time point.
The aim of this study was to test if/how the GT marker used for the definition of the frontal plane of the thigh affects hip and knee kinematics during gait.The differences in hip and knee angles with and without GT were greater in the transverse planecompared to the sagittal and frontal planes,but so was the variability (Fig.2).During the stance phase,the hip was externally rotated when the GT was included but internally rotated when the GT was not included (Fig.3C).The use of the thigh segment without GT in the hip angle calculation seems to reflect the transverse plane hip motion reported for healthy subjects.17,18However,without“gold-standard”bone pin studies for comparison,it is difficult to make a definitive statement as to which hip model is preferable.That said,when attempting to compare data with other investigators,it is important to consider the marker set and model configurations used across laboratories,as different marker sets and models may lead to different clinical interpretations.
In the transverse plane,Knee_noGT was in internal rotation at PKF and in external rotation at MinKF,similar to what has been reported.19,20Knee_GT presented higher values of internal rotation at PKF compared to the other knee angles and it was in internal rotation at MinKF (Fig.2D).Therefore when the GT is used in the thigh segment,the knee may be more internally rotated throughout the task.Knee_noGT,instead,oscillated around zero throughout the gait cycle (Fig.3F).Our knee results may be comparable to those of investigators who used bone-pin techniques.Knee_noGT showed only a few degree of internal rotation at 15% and 30% of stance (Fig.3F),and both knee angles are close to 0°in the midstance phase.Lafortune and collegues21found that at 25% and 35% of the stance phase the knee was internally rotated 5°while at mid-stance the transverse angle was close to 0°.Similarly Reinschmidt and colleagues22reported that the knee transverse plane angle was close to 0°around midstance,fluctuating from internal rotation in early stance to few degrees of external rotation in late stance.
As expected,the GT marker had less effect on the sagittal and frontal plane angles,since the angles differed slightly and only in magnitude (Fig.2).In the frontal plane at the knee we observed very little motion during stance.This finding is in line with the findings of previous bone pin studies,21,23and is consistent with what would be expected of healthy knee anatomy,which should restrict frontal plane motion during typical activities.However,albeit all the knee angles were close to 0°during stance,the time series curves showed that the knee angle with GT was in more abduction during the swing phase (Fig.3E).Considering that during swing,the knee is undergoing flexion with minimal ab/adduction forces,24this finding may be due to some degree of cross-talk between sagittal and frontal plane angles in the GT models.25,26
While there were significant differences in the sagittal and frontal plane angles at both time points,the differences were small (on average,less than 2°in the sagittal plane and less than 1°in the frontal plane) and less than or close to the SEM.As such,the importance of these differences is questionable,and it appears that the models (with or without GT) could be used interchangeably to quantify kinematic variables in the sagittal and frontal planes.
Our findings should be considered in light of several limitations.Poor placement of the GT marker (e.g.,too posterior) could have oriented the frontal plane of the thigh in excessive external rotation,consequently orienting the position of the shank relative to the thigh in excessive internal rotation (Fig.3C: Hip_GT curve; 3F: Knee_GT curve).The GT vertically aligned with the lateral epicondyle might have led to more similar hip and knee kinematics across models.As such,rather than only palpating the bony prominence of the GT,it would be advisable to align the GT and the lateral epicondyle marker in a vertical line to approximate the frontal plane of the thigh.Alternatively,only three points (hip joint center and the femoral epicondyles) could be used to define the frontal plane.The differences we observed in the knee angles could also be due to the orientation of the transmalleolar axis that could have biased the shank frontal plane toward excessive internal or external rotation.We minimized the risk for this bias by placing the malleolar markers to approximate the flexion/extension axis of the ankle.A second limitation is that we investigated asymptomatic healthy young adults,who had body mass indices in the normal range.Hence our findings may not be generalizable to clinical populations or obese individuals.A third limitation is that we tested a low-level task (gait),where the amount of hip and knee motion is fairly minimal.It is not clear whether the same findings would be observed in more challenging tasks that require greater amounts of lower extremity motion.
5.Conclusion
Hip and knee kinematics during gait differ across thigh segment definitions,with the greatest differences occurring in the transverse plane.Hence,when using models that employ surface markers to calculate 3D kinematics for movement assessment,it is important to have a clear understanding of the effect of different marker configurations on the key variables of interest.
Acknowledgment
This project was funded in part by the National Institute of Child Health and Human Development (No.NICHD,No.R15HD059080,and No.R15HD059080-01A1S1).
Authors’contributions
GBS and VG designed the study and analyzed the data.VG performed data collection.VG and GBS drafted and revised the manuscript.Both authors approved the final version of the manuscript and agreed on the order of presentation of the authors.
Competing interests
None of the authors declare competing financial interests.
References
1.Holden JP,Stanhope SJ.The effect of variation in knee center location estimates on net knee joint moments.Gait Posture 1998;7:1-6.
2.Pollard CD,Heiderscheit BC,van Emmerik REA,Hamill J.Gender differences in lower extremity coupling variability during an unanticipated cutting maneuver.J Appl Biomech 2005;21:143-52.
3.Ferber R,McClay Davis I,Williams 3rd DS.Gender differences in lower extremity mechanics during running.Clin Biomech 2003;18:350-7.
4.Milner CE,Hamill J,Davis I.Are knee mechanics during early stance related to tibial stress fracture in runners? Clin Biomech 2007;22: 697-703.
5.Geiser CF,O’Connor KM,Earl JE.Effects of isolated hip abductor fatigue on frontal plane knee mechanics.Med Sci Sports Exerc 2010;42: 535-45.
6.Sanna G,O’Connor KM.Fatigue-related changes in stance leg mechanics during sidestep cutting maneuvers.Clin Biomech 2008;23:946-54.
7.Willson JD,Davis IS.Lower extremity mechanics of females with and without patellofemoral pain across activities with progressively greater task demands.Clin Biomech 2008;23:203-11.
8.Bohn MB,Sørensen H,Petersen MK,Søballe K,Lind M.Rotational laxity after anatomical ACL reconstruction measured by 3-D motion analysis: a prospective randomized clinical trial comparing anatomic and nonanatomic ACL reconstruction techniques.Knee Surg Sports Traumatol Arthrosc 2015;23:3473-81.
9.Castanharo R,Duarte M,McGill S.Corrective sitting strategies: an examination of muscle activity and spine loading.J Electromyogr Kinesiol 2014;24:114-9.
10.Della Croce U,Cappozzo A,Kerrigan D.Pelvis and lower limb anatomical landmark calibration precision and its propagation to bone geometry and joint angles.Med Biol Eng Comput 1999;37:155-61.
11.Della Croce U,Camomilla V,Leardini A,Cappozzo A.Femoral anatomical frame: assessment of various definitions.Med Eng Phys 2003;25:425-31.
12.Powers CM,Ward SR,Fredericson M,Guillet M,Shellock FG.Patellofemoral kinematics during weight-bearing and non-weight-bearing knee extension in persons with lateral subluxation of the patella: a preliminary study.J Orthop Sports Phys Ther 2003;33:677-85.
13.Ford KR,Myer GD,Hewett TE.Valgus knee motion during landing in high school female and male basketball players.Med Sci Sports Exerc 2003;35:1745-50.
14.Bell AL,Pederson DR,Brand RA.Prediction of hip joint center location from external landmarks.Hum Mov Sci 1989;8:3-16.
15.Bell AL,Pederson DR,Brand RA.A comparison of the accuracy of several hip center location prediction methods.J Biomech 1990;23:617-21.
16.Shrout PE,Fleiss JL.Intraclass correlations: uses in assessing rater reliability.Psychol Bull 1979;86:420-8.
17.Perry J,Burnfield JM.Gait analysis: normal pathological function.2nd.Thorofare: Slack Incoporated; 2010.
18.Lin YC,Gfoehler M,Pandy MG.Quantitative evaluation of the major determinants of human gait.J Biomech 2014;47:1324-31.
19.Ishii Y,Terajima K,Terashima S,Koga Y.Three-dimensional kinematics of the human knee with intracortical pin fixation.Clin Orthop Relat Res 1997;343:144-50.
20.Fuss FK.Principles and mechanisms of automatic rotation during terminal extension in the human knee joint.J Anat 1992;180:297-304.
21.Lafortune MA,Cavanagh PR,Sommer 3rd HJ,Kalenak A.Three-dimensional kinematics of the human knee during walking.J Biomech 1992;25:347-57.
22.Reinschmidt C,van den Bogert AJ,Lundberg A,Nigg BM,Murphy N,Stacoffa A,et al.Tibiofemoral and tibiocalcaneal motion during walking: external vs.skeletal markers.Gait Posture 1997;6:98-109.
23.Benoit DL,Ramsey DK,Lamontagne M,Xu L,Wretenberg P,Renstrom P.In vivo knee kinematics during gait reveals new rotation profiles and smaller translations.Clin Orthop Relat Res 2007;454:81-8.
24.Piazza SJ,Delp SL.The influence of muscles on knee flexion during the swing phase of gait.J Biomech 1996;29:723-33.
25.Ferrari A,Benedetti MG,Pavan E,Frigo C,Bettinelli D,Rabuffetti M,et al.Quantitative comparison of five current protocols in gait analysis.Gait Posture 2008;28:207-16.
26.Schache AG,Baker R,Lamoreux LW.Defining the knee joint flexion-extension axis for purposes of quantitative gait analysis: an evaluation of methods.Gait Posture 2006;24:100-9.
杂志排行

Journal of Sport and Health Science的其它文章
- Non-linearity in the dynamic world of human movement
- Comparing dynamical systems concepts and techniques for biomechanical analysis
- Multi-scale interactions in interpersonal coordination
- Can coordination variability identify performance factors and skill level in competitive sport? The case of race walking
- Multiscale entropy: A tool for understanding the complexity of postural control
- A history of low back pain affects pelvis and trunk coordination during a sustained manual materials handling task