A history of low back pain affects pelvis and trunk coordination during a sustained manual materials handling task
2016-04-25JosephSeyShneSuerTejshPtelTnjRoyMilitryPerformnceDivisionArmyReserchInstituteofEnvironmentlMedicineNtickMA01760USABiophysicsndBiomediclModellingDivisionArmyReserchInstituteofEnvironmentlMedicineNtickMA01760USAReceivedMrch
Joseph F.Sey*,Shne G.SuerTejsh Ptel,Tnj C.RoyMilitry Performnce Division,U.S.Army Reserch Institute of Environmentl Medicine,Ntick,MA 01760,USABiophysics nd Biomedicl Modelling Division,U.S.Army Reserch Institute of Environmentl Medicine,Ntick,MA 01760,USA Received 1 Mrch 2015; revised 20 July 2015; ccepted 20 Novemer 2015 Aville online 11 Jnury 2016
A history of low back pain affects pelvis and trunk coordination during a sustained manual materials handling task
Joseph F.Seaya,*,Shane G.Sauera,Tejash Patelb,Tanja C.RoyaaMilitary Performance Division,U.S.Army Research Institute of Environmental Medicine,Natick,MA 01760,USAbBiophysics and Biomedical Modelling Division,U.S.Army Research Institute of Environmental Medicine,Natick,MA 01760,USA Received 1 March 2015; revised 20 July 2015; accepted 20 November 2015 Available online 11 January 2016
Peer review under responsibility of Shanghai University of Sport.
* Corresponding author.
E-mail address: joseph.f.seay.civ@mail.mil (J.F.Seay).
http://dx.doi.org/10.1016/j.jshs.2016.01.011
2095-2546/©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.
Abstract
Purpose: The purpose of this study was to compare the coordination between the trunk and the pelvis during a sustained asymmetric repetitive lifting task between a group with a history of low back pain (LBP; HBP) and a group with no history of LBP (NBP).
Methods: Volunteers lifted a 11-kg box from ankle height in front to a shelf 45°off-center at waist height,and lowered it to the start position at 12 cycles/min for 10 min.Lifting side was alternated during the trial.Continuous relative phase was used to calculate coordination between the pelvis and trunk rotation at the beginning (Min 1),middle (Min 5),and end of the bout (Min 9).
Results: While there were no main effects for group,a significant interaction between time and group indicated that,in the frontal plane,the NBP group coordination was more anti-phase toward the end of the bout,with no such differences for the HBP group.Analysis of sagittal-axial (bend and twist) coordination revealed the HBP group coordination was more in-phase at the end of the bout over the entire cycle and for the lifting phase alone,with no such differences for the NBP group.
Conclusion: Differences between groups demonstrate residual consequences of LBP in an occupational scenario,even though the HBP group was pain-free for>6 months prior to data collection.More in-phase coordination in the HBP group may represent a coordination pattern analogous to “guarded gait”which has been observed in other studies,and may lend insight as to why these individuals are at increased risk for re-injury.
©2016 Production and hosting by Elsevier B.V.on behalf of Shanghai University of Sport.
Keywords:Lifting; Lowering; Occupational biomechanics; Relative phase; Relative phase variability
1.Introduction
Low back pain (LBP) has long ago reached epidemic proportions in the US,with four out of five people experiencing LBP at least once in their lives.1,2LBP is also the most common reason for seeking medical care for civilians3and military alike.4,5In military cohorts,back pain-related medical issues were among the top three leading causes for lost duty days for U.S.soldiers as recently as 2011.5,6Issues related to back pain have also ranked among the highest risk factors for permanent disability within 5 years of onset at 20%.7
Symptoms resolve for most individuals who experience LBP,and these individuals return to pre-injury work and activity levels pain-free within 8 weeks.8While the majority of healthcare resources are spent on those individuals for whom LBP lasts longer,1the others who return to occupational and recreational activity with a history of LBP (HBP) are more likely to experience recurring episodes of LBP.Within 1 year after initial LBP episode,epidemiological studies report recurring episodes at rates ranging from 24% to 50%.9,10
Research estimates that only 6%-15% of reported LBP episodes are first-time episodes;11with over 85% of annual LBP cases being recurrences.It is not surprising that HBP places individuals at increased risk for future episodes.This notion is supported by other studies which report 24%-50% of those who suffer initial LBP episodes have a recurring episode of LBP within 1 year,9and that chance of recurrence increases with age.9In collegiate athletes,one study reported that athletes with HBP were three to six times more likely to suffer a bout of LBP during their collegiate career than activity-matched athletes who never had LBP.12In the U.S.military,a high disability rate due to LBP,combined with a 19% disability rate leads to an estimate that approximately 80% of soldiers return to full dutyafter LBP,and that approximately 24% of the U.S.Army can be categorized as HBP.6,7,13
The athletic literature has demonstrated that there are functional consequences to having HBP.Collegiate athletes with HBP,who had returned to full activity levels within their sport for quite some time,ran significantly slower on the shuttle run when compared to sport-matched controls with no history,14suggesting that their performance-related residual effects were associated with HBP.Also differences have been observed in walking and running mechanics between those with and without LBP.When comparing runners with mild to moderate LBP vs.runners with HBP vs.runners who have never experienced LBP (NBP),research has documented increases in knee stiffness,15more in-phase pelvis-trunk coordination,16and decreases in coordination variability.17These disparities are consistent with the“guarded gait”typically associated with more severe LBP.
In the ergonomic literature,studies have implied that participating in manual materials handling tasks is among the work-related factors associated with LBP.18-21There is also an increased risk of occupational LBP with any job task which involves the motion combinations of bending and twisting from the waist (trunk sagittal lean and rotation).3,22,23Such factors are also a consideration in the military,where one report indicates that slightly more than 2/3 of U.S.soldier occupational tasks involve lifting and lowering between the ground and waist height.24However,few studies have explored differences in lifting mechanics between individuals with and without HBP; insight into these differences could elucidate adaptations due to LBP.A recent study has reported differences in lifting mechanics between soldiers with and without HBP; specifically,individuals with HBP maintained more consistent mechanics (range of motion and angular velocity) during a 10-min lift/lower task than those with NBP.25
Dynamical systems measures,such as continuous relative phase (CRP) analysis,have been able to provide information on how segments interact relative to each other.Relative phase has been utilized in the past to incorporate angular position and angular velocity information over an entire motion cycle which compliments kinematic analyses.26Data analyzed using relative phase angle (CRPθ) and CRPθ variability have demonstrated differences in lower limb27,28and pelvis-trunk coordination17,29between individuals with and without LBP.Additionally,these measures can be adapted to analyze segmental interactions which incorporate asymmetric motions,such as trunk bend and twist (sagittal bend and axial rotation) during running.30Using such techniques to analyze interactions between the pelvis and trunk during a manual materials handling paradigm will allow for additional insights into the“bend and twist”motions associated with occupational LBP.
The purpose of this study was to compare the coordination and coordination variability profiles of the trunk and the pelvis during a sustained asymmetric repetitive lifting task between an HBP and an NBP group during a repeated box lift/lower paradigm.We chose a 10-min asymmetric lift/lower paradigm in order to simulate a typical time-modulated occupational scenario.We chose a box mass of 11 kg and cadence of 12 lift/lower cycles/min in order to provide sufficient physical stress to elicit any time-related differences between the groups and to ensure that all participants were performing the same amount of work at the same rate,while maintaining the safety of our participants with HBP.We hypothesized that the HBP group would demonstrate different coordination mechanics over time as compared to the NBP group.Specifically,we expected the HBP group to display more in-phase coordination (CRPθ; values closer to 0),which would represent“guarded mechanics”often associated with LBP during gait.Consistent with previous coordination findings,29we also hypothesized that the HBP group would demonstrate decreased coordination variability,demonstrating a decreased ability to adapt after the resolution of LBP and/or over time.
2.Materials and methods
2.1.Participants
Twenty healthy male soldiers gave informed consent to participate in this study.Ethical approval was granted by the U.S.Army Research Institute of Environmental Medicine’s institutional review board.The investigators adhered to the policies for protection of human subjects as prescribed DoD Instruction 3216.02 and the research was conducted in adherence with the provisions of 32 CFR Part 219.Participants were asked about their history with LBP.LBP was defined as pain,soreness,or tightness that prevented a person from performing their usual duty or training regimen for more than 3 days.Because we were interested in non-specific LBP,participants were excluded from participation if they reported that their LBP was the result of traumatic injury,or if they were medically diagnosed with a slipped or bulging inter-vertebral disc.Those who had never experienced a bout of LBP were placed in the NBP group (n = 11; 176.8±5.2 cm; 81.6±14.0 kg; 26±6 years).If a participant had experienced a bout of LBP that lasted less than 6 weeks and have had no symptoms for at least 6 months,then they were placed in the history of back pain group (n = 9; 176.4±5.1 cm; 81.0±11.4 kg; 24±5 years).Participants were also excluded from participation if they reported any current or prior musculoskeletal injuries or medical conditions that would either interfere with their completion of the testing or that would predispose them to injury during the testing.
2.2.Equipment
A detailed description of the methods used in this study has been published previously.25A custom 3-shelf station was constructed for this experiment.Two platforms were affixed to the left and right of a central vertical channel,angled at 45°.Within the central channel a small step was built atop an adjustable floor (Fig.1).Foam blocks could be inserted to adjust the floor height so that the two platforms would be at waist height of the participant standing on the flooring.The low central platform shielded the participant’s feet,while creating an ankle height shelf for an 11-kg box with handles to be placed directly in front of the participant.The box was lifted and lowered from shelf to shelf at a fixed cadence maintained using a metronome (KDM-2; KORG USA Inc.,Melville,NY,USA).
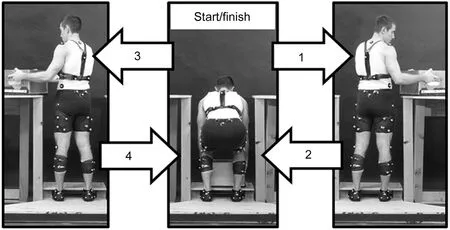
Fig.1.Representation of a complete lift/lower cycle.The 11-kg box lift was initiated from the center position and completed on the right platform.The box was then returned to the center before repeating the pattern to the left side.Each step (1,2,3,4) is allotted 2.5 s.Trunk motion was tracked using the three markers on the torso harness and pelvic was tracked using the sacral triad.During actual data collection,sacral markers were secured with tape.
For purposes of recording movement,reflective markers were placed bilaterally on skin and clothing locations corresponding to the participants’body segments.25Threedimensional (3D) motion of these reflective markers were captured using 12 Motion Capture Unit (MCU) cameras (Qualisys AB,Goteborg,Sweden) surrounding the lifting station.The reflective markers defining the local segment coordinate systems for the pelvis were placed bilaterally on the anterior superior iliac spines (ASIS),posterior superior iliac spines (PSIS),sacrum,greater trochanter (GT),and iliac crest (ILCR,directly superior to the GT during quiet standing).The trunk segment was defined using calibration markers placed bilaterally on the iliac crest and on the acromioclavicular joints (Fig.1).The PSIS and sacrum markers were used to track pelvic movement.Markers on a rigid lightweight molded plastic frame secured to the posterior aspect of the trunk were used to track the motion of the trunk (Fig.1).
2.3.Procedures
Once a participant gave informed consent and medical clearance was granted,data were collected in a single session.Upon arrival to the lab,the participant’s anthropometrics were recorded.Next the participant was given instructions for the session.Specifically,participants were told to perform the lift while maintaining the pace set by the metronome,to keep their feet stationary during the entire bout,and to fully release their fingers from the box at each platform.No additional lifting technique instructions were provided.
Following the instructions,the participant was asked to practice the box lifting task.Once the participant was comfortable with the movement and felt sufficiently warmed up,and the investigator was satisfied with the participant’s ability to maintain the cadence,the reflective markers were placed as previously described.25
The lifting task itself required the participant to first lift the 11-kg box from the low platform to the right elevated shelf and back before going to the left side.The box lift was performed without stopping for 10 min at a rate of 12 lift/lower cycles per minute alternating between the elevated platforms.Kinematic data were collected at Min 1,Min 5,and Min 9 for 65 s to ensure six lift/lower cycles to each side were captured.
2.4.Data processing
Marker data were tracked using Qualysis Track Manager software (Qualisys AB).Visual 3D motion analysis software (C-Motion Inc.,Germantown,MD,USA) was used to filter motion data (low pass,second order Butterworth filter at 15 Hz) and calculate 3D segmental angles and velocities for the pelvis and trunk segments.For the purposes of analysis,custom MATLAB software (The MathWorks,Inc.,Natick,MA,USA) was used to divide the data into lifting and lowering phases of the cycle for both left (lifting to the left,lowering from the left) and right sides (lifting to the right,lowering form the right).Four points on the front of the box were averaged to ascertain box position,which was used to define lifting and lowering phases based on position and acceleration profiles of the box,and excluded portions of the lift where the box was at rest (i.e.,zero acceleration).This allowed for examination of both phases separately and excluded periods of time during which the box was resting on any of the shelves.
Once the sides and action were determined,continuous relative phase (CRPθ) calculations were initiated by combining the segmental angles and velocities to create a position-velocity phase plane.The phase plane was normalized to the unit circle to later correct for any frequency and amplitude differences between the pelvis and trunk segments.31Next phase angles were generated from the phase plane through the use of the arctangent function.CRPθ was then calculated as the absolute value of the difference between the phase angles of each segment.CRPθ was calculated for each of the six complete lifting and lowering cycles to/from the right and left sides.CRPθ variability (CRPvar) could now be calculated as the average of each cycle’s deviation from the mean CRPθ value within a given time point (Min 1,Min 5,or Min 9).
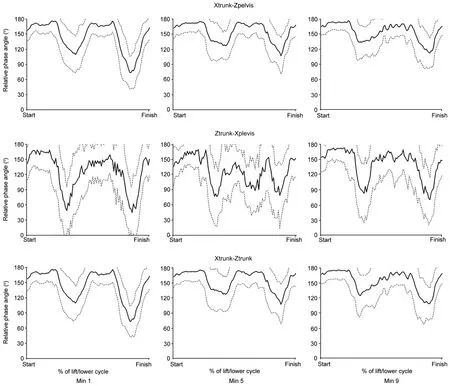
Fig.2.Exemplar plots of CRPθ(solid dark line) and CRPvar (lighter dashed lines) for sagittal-axial for one exemplar subject.CRP = continuous relative phase.
We analyzed single plane interactions in the sagittal and transverse planes.In order to examine pelvis-trunk coordination during the bending and twisting motion,we analyzed three additional segmental interactions.Within the trunk segment we examined the sagittal plane and transverse plane interactions (Xtrunk-Ztrunk).While this combination has been utilized previously to demonstrate differences in pelvis-trunk coordination between runners with and without LBP,30it does not involve the pelvis,which is more integral to lifting during a manual materials handling task.Therefore,we decided to examine the interaction between pelvis anteriorposterior tilt and trunk axial rotation (Xpelvis-Ztrunk) and trunk anterior lean with respect to pelvis rotation (Xtrunk-Zpelvis).Fig.2 represents an exemplar sagittal-axial relative phase resultant plot for one exemplar subject.
2.5.Statistical analysis
Group means were reported for CRPθ and CRPvar in both groups during the lifting and lowering portions of the total cycle at the beginning (Min 1),middle (Min 5),and end (Min 9) of the trial,and for both the right and left sides.Initially a 3-way analyses of variance (ANOVA) was conducted to examine the relationship between group (HBP,NBP),time (Min 1,Min 5,Min 9) and side (L,R).While the results of this analysis revealed no significant interactions involving side (group×side,time×side,or group×time×side),several main effects for time did emerge.Two-way repeated measures ANOVA were conducted to examine the relationships between LBP group (HBP,NBP) and time (Min 1,Min 5,Min 9) for each variable examined for each side of the body.Holm-Sidakpost hoc analysis was performed when significant interactions or main effects (p≤0.05) were reported.In order to supplement the interpretation of statistically significant results,effect sizes (ES) were calculated to assess the practical importance of a difference between means,estimated as the difference between two means over a pooled standard deviation.Cohen32proposed that ES>0.8 represent large practical differences and that ES>0.5 is clinically meaningful when comparing two means within biological systems.Data were analyzed using SigmaPlot (version 12.0; Systat Software,Inc.,San Jose,CA,USA).
3.Results
3.1.Single-plane analyses
In the sagittal plane there was a main effect for time for CRPvar while lifting to the right side (p = 0.013).When averaged across groups,CRPvar was greater at Min 1 than Min 5 (p = 0.01) (ES = 0.7).There were no interactions or other main effects,nor were there any significant findings while lifting to the left side (Table 1).
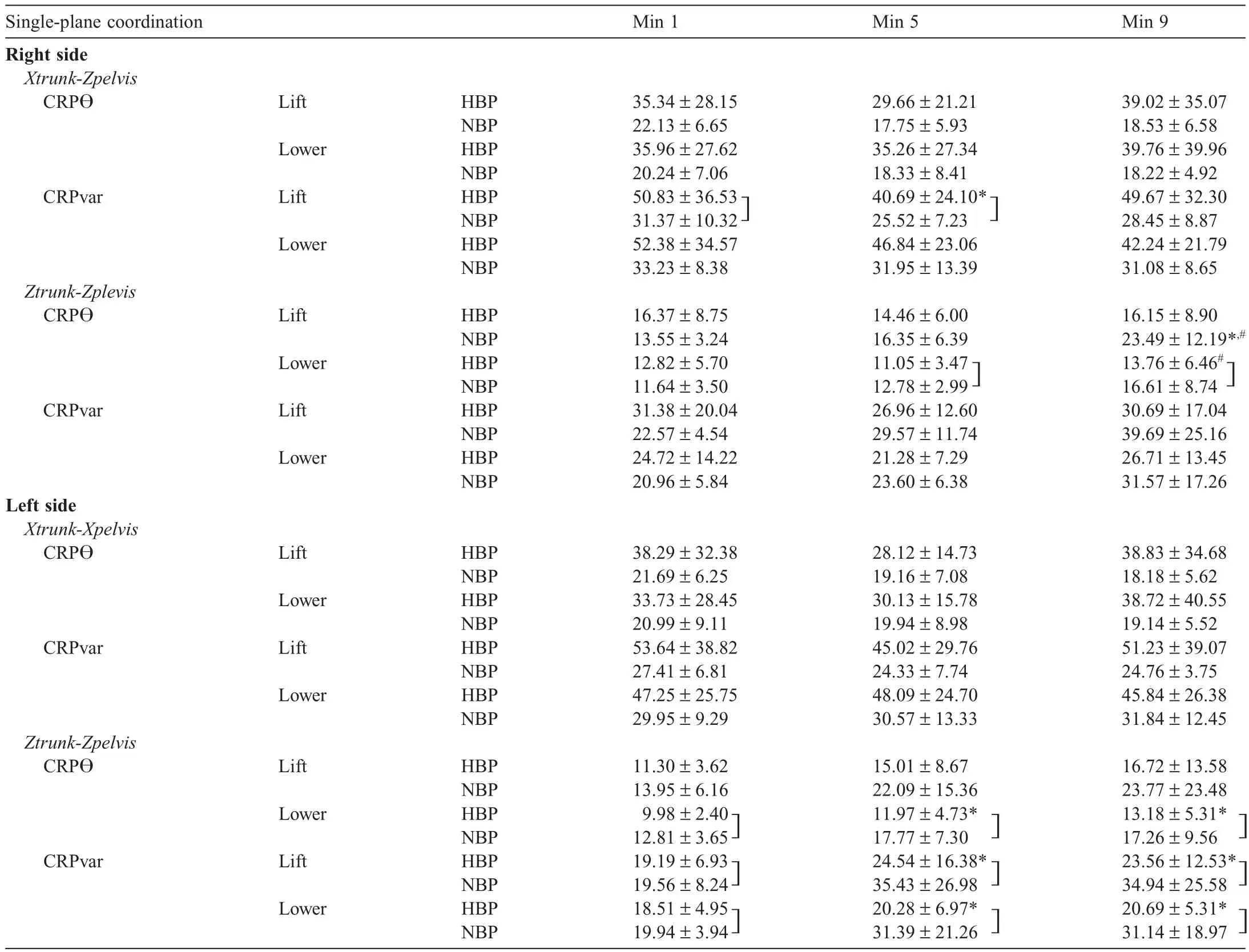
Table 1Single-plane coordination (CRP) and coordination variability (CRPvar) results.
Transverse plane comparisons revealed a group×time interaction for CRPθ while lifting to the right side (p = 0.024),with post hoc analyses revealing that,within the NBP group,CRPθ was significantly greater at the end of the bout than at the beginning or the middle (p<0.001 and p = 0.009,respectively).There were also main effects for time while lowering from the right for CRPθ(p = 0.03) and CRPvar (p = 0.04) (Table 1).CRPθ values were significantly greater at the end of the bout (Min 9) than in the middle (Min 5,p = 0.05).However,all significant results were translated to small practical differences,with ES<0.4.While lifting to the left there was a main effect of time for CRPvar,with post hoc analyses revealing that CRPvar at Min 1 was significantly less than at Min 5 and Min 9 (both p≤0.05).There were also main effects of time for CRPθand CRPvar while lowering from the left.Post hocs revealed that CRPθ values were greater (more anti-phase) in the beginning than at the middle or at the end of the bout (both p≤0.02),and CRPvar was significantly less at the beginning than at the other two time points (both p≤0.05).All left side ES≤0.5,suggesting differences may be approaching clinical significance.
There were no further significant interactions or main effects in any plane for CRPθ or CRPvar for either component phase.
3.2.Bend and twist comparisons
Analysis of trunk anterior lean and axial rotation (Xtrunk-Ztrunk) revealed a main effect for time in CRPvar while lowering from the right (p = 0.009),with CRPvar at Min 9 significantly greater than at Min 5 and Min 1 (p≤0.012) (ES≤0.7).When lowering from the left,there was a main effect for time,with post hoc analyses revealing that CRPθ was more anti-phase at Min 1 than at Min 9 (p = 0.03).CRPvar was also significantly less at the beginning of the bout than in the middle or at the end (both p≤0.04,ES<0.4) (Table 2).
Analysis of pelvis sagittal and trunk rotation (Xpelvis-Ztrunk) revealed a group time interaction for CRPθ(p = 0.03) and CRPvar (p = 0.04) during the lifting phase from the right (Table 2).For CRPθ post hoc analysis revealed that,within the HBP group,Min 5 was greater than Min 9 (p = 0.010).Post hocs showed that CRPvar was greater for Min 1 and Min 9 than Min 5 within the HBP group (p≤0.04).All significant relationships had clinically meaningful ES ranging from 0.5 to 0.7.There were no significant relationships between group and time when lifting to the left or lowering from the left side.
Analysis of trunk forward lean relative to pelvis axial rotation (Xtrunk-Zpelvis) revealed group time interactions for CRPvar during the lifting phase (p = 0.006).Post hoc analysis revealed that,within the HBP group,CRPvar was lower at Min 1 and Min 5 than Min 9 (p = 0.004).Additionally,during the lifting phase,CRPvar for the HBP group was significantly greater than the NBP group at Min 9 (p = 0.008).All significant relationships in the Xtrunk-Zpelvis coupling while lifting to or lowering form the right-hand side had ES ranging from 0.8 to 1.3,indicating large practical differences.While lifting to the left side,CRPθ was more anti-phase during Min 1 than Min 5 and Min 9 (p≤0.04,ES = 0.4) (Table 2).
There were no further significant interactions or main effects in any plane for CRPθ or CRPvar for either component phase.
4.Discussion
The purpose of this study was to examine differences in pelvis-trunk coordination and coordination variability during a repetitive box lifting and lowering task between individuals with and without HBP.We hypothesized that individuals with HBP would demonstrate more in-phase coordination mechanics than those without,and that differences would be exacerbated over time.The majority of our main effect significant results were time-related (time-related hypotheses supported),where coordination or variability changed relative to the beginning of the lifting bout,regardless of group.There were no main effects for group,likely because both groups were highly functional; however,analysis of significant group×time interactions revealed that there were group-related adaptations (Table 2).Analysis of sagittal-axial (bend and twist) coordination revealed the HBP group coordination was more in-phase at the end of the lifting phase,with no such differences for the NBP group (Table 2).
4.1.Comparison to kinematic analysis
Results of transverse plane are consistent with transverse plane range of motion (ROM) and angular velocity results from the same cohort.25Briefly,there was no difference in pelvis and trunk segmental ROM between groups at the beginning of the bout; however,at the end of the bout,the NBP ROM decreased,while the HBP ROM remained constant throughout the bout.Ultimately this was interpreted as less constrained lifting mechanics over the entire lifting bout for the group who had never experienced LBP; the NBP group maintained the assigned lift/lower pace by utilizing their arms.25
The results of the current study compliment the kinematic findings.The more consistent kinematics observed in the HBP group were considered protective,somewhat analogous to the guarded gait which is typical of individuals who are experiencing LBP.33Results from the current study revealed significant differences in transverse plane coordination and variability during the lowering phase,and no group differences.Regardless of which phase of the lifting cycle was examined,the HBP group coordination mechanics became more in-phase (i.e.,decreasing CRP) toward the end of the bout.This is also consistent with a“guarding”strategy,which may be residual from the injury.However,the coordination variability generally increased for this group as time went on as well,which is consistent with more adaptable mechanics over time that one would expect from a healthy system.Therefore,while overall mechanics became more in-phase over time,the system was still able to adapt over the course of the bout.
4.2.Single-plane couplings
Main effects for time occurred during the single-plane analyses (Xtrunk-Xpelvis,Ztrunk-Zpelvis; Table 1).Where differences occurred during the lowering phase,pelvis-trunk CRPθ was more anti-phase at the end of the bout,suggesting that the pelvis and trunk were controlled more as separate segments as time progressed during the bout,and were less constrained to work as a pair.This likely developed with practice and as familiarity increased with the task.That there were no main effects for group suggests that the mechanics of both groups evolved similarly over the duration of the lifting bout.
4.3.Sagittal-axial coupling
While there were no main effects for group,sagittal-axial (bend and twist) couplings revealed coordination differences for the HBP group over time during post hoc analyses of group×time interactions (Table 2).Specifically,the HBP group coordination became more in-phase at the end of the
bout,suggesting at least some degree of guarding occurred within the HBP group as time progressed.These findings are consistent with Jones et al.,34who reported that individuals with HBP demonstrated increased back muscle activation patterns during postural responses to trunk perturbations.The motions utilized in our paradigm were more predictable and consistent,so the guarding may have taken place during the end of the bout as HBP individuals became more tired.One potential limitation of our study is that we did not utilize electromyography (EMG); future studies utilizing these techniques in combination with lifting mechanics would elucidate this matter.
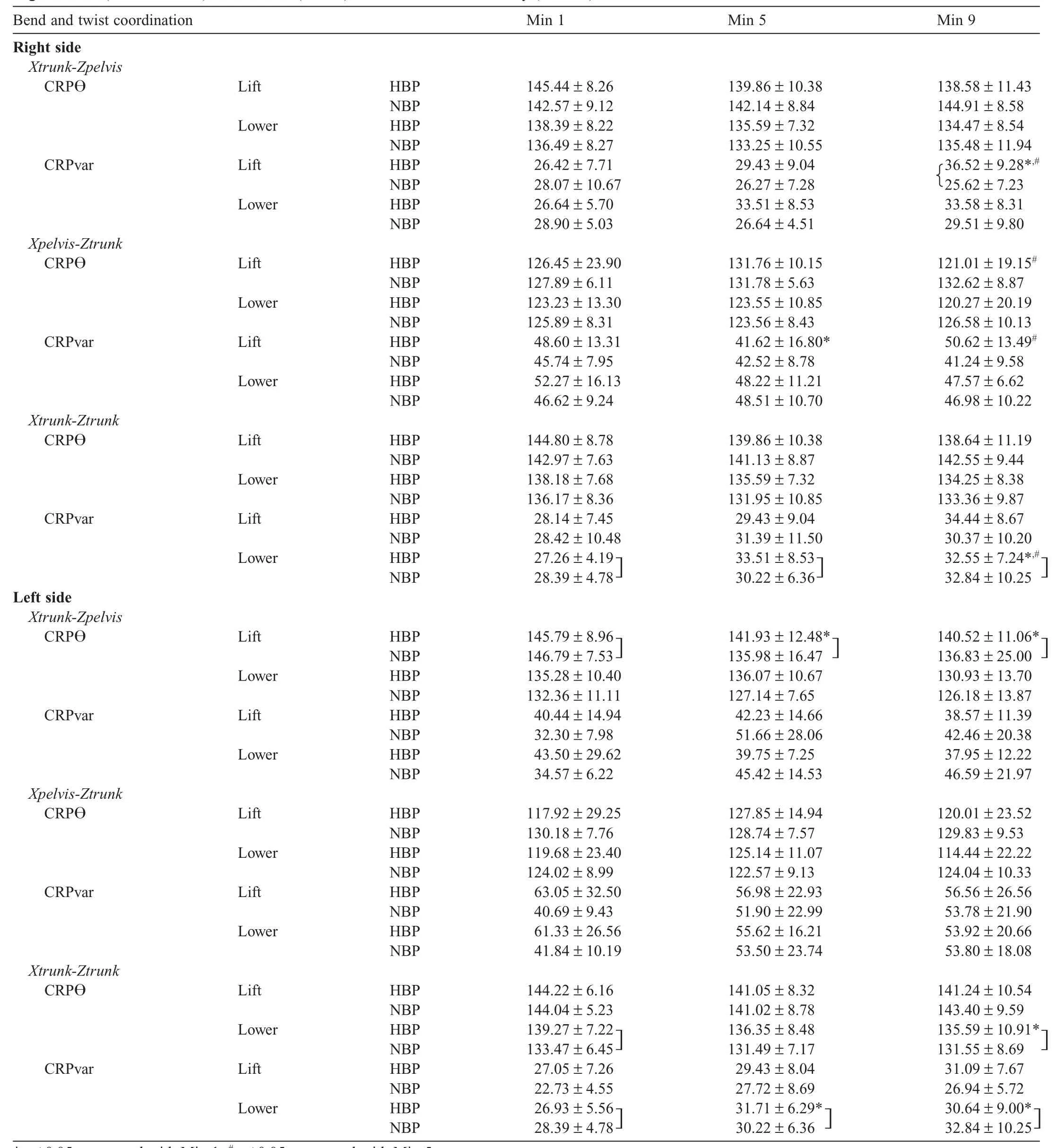
Table 2Sagittal-axial (bend and twist) coordination (CRPθ) and coordination variability (CRPvar) results.
The results of our study were coupling-dependent,which supports the concept posited by Hodges and Tucker35that the adaptations related to HBP are more complex and less uniform than initially posited.That our results were different between lifting and lowering phases supports the earlier work of Nelson et al.,36who reported kinematic differences in ROM lifting mechanics between lifting and lowering phases during a box lift which occurred in the sagittal plane only (symmetric).Nelson et al.36reported that lumbo-pelvic motion occurred more simultaneously during the lifting phase,and motions were more concurrent during the lowering phase of the cycle.While we would apply this interpretation of motions directly to our findings,in that more in-phase coordination corresponds to more simultaneous motion,and more anti-phase coordination to more concurrent motion,there were important differences between their study and the current study.In addition to the fact that our lifting paradigm was different from that of Nelson et al.36in that it was more asymmetric,involving motions in the sagittal and axial plane,Nelson et al.36required all participants to lift and lower without bending the knees,which likely exacerbated differences in their healthy cohort.
4.4.Right and left side comparisons
While there were different patterns of statistical significance between the right and left sides,generally the values for CRPθ and CRPvar were similar for each coupling,and followed similar trends over time.There was a group-related adaptation during lifting to the right side,where CRPvar for HBP was significantly greater than for NBP.No such difference existed for the left side.We surmise that this larger difference in CRPvar may have occurred due to the right-hand side being the dominant side in our participant pool.Since the dominant side is associated with finer motor control than the non-dominant side,we posit that side-related preference may have manifested in CRPvar during a bilateral task.In this case,lower CRPvar may signify increased control during the task.Future studies should explore this possibility further to confirm this observation.
4.5.Limitations
There were a number of limitations associated with our study.We recognize that limiting lifting frequency could have influenced coordination.Future studies could mitigate this effect by designating a specific number of lifts (for example,125 lift/lower cycles),counting lifts and collecting data during pre-designated lift intervals during the bout.We also acknowledge that we might have seen greater side-side differences between groups if we had documented which side had been more affected by LBP in our HBP group (generally speaking,idiopathic LBP does not tend to be symmetric).Despite these potential limitations,differences in lifting mechanics were observed using the current paradigm.
5.Conclusion
This study has documented changes in coordination profiles during manual materials handling paradigm over an extended bout compared to other research.Data from the current study offer a preliminary view of coordination profiles during 10 min of lifting an 11-kg box with handles at 12 lift/lower cycles per minute between individuals with and without HBP.Results indicated that coordination (CRPθ) and coordination variability (CRPvar) were sensitive enough measures to detect differences between these two highly functional groups.More in-phase coordination in the HBP group may represent a coordination pattern analogous to“guarded gait”which has been observed in other studies.While ES suggested limited practical differences in the single-plane couplings,the sagittal axial couplings in general had larger practical differences,which may lend insight as to why these individuals are at increased risk for re-injury.Our results also demonstrated the benefit of using both single-plane and multi-plane analysis for characterizing coordination profiles during an asymmetric (i.e.,out-of-plane) lift.
Acknowledgment
The opinions or assertions contained herein are the private views of the author(s) and are not to be construed as official or as reflecting the views of the Army or the Department of Defense.
Authors’contributions
JFS and TCR conceived the study,and participated in its design and coordination; SGS executed the study and reduction of video data; JFS,SGS,and TP processed the video data and conducted coordination calculations; JFS performed the statistical analysis and drafted the initial manuscript.All authors have read,contributed to,and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
None of the authors declare competing financial interests.
References
1.Scheer SJ,Watanabe TK,Radack KL.Randomized controlled trials in industrial low back pain.Part 3.Subacute/chronic pain interventions.Arch Phys Med Rehabil 1997;78:414-23.
2.Plante DA,Rothwell MG,Tufo HM.Managing the quality of care for low back pain.In: Frymoyer JW,editor.The adult spine: principles and practice.2nd ed.Philadelphia,PA: Lippincott-Raven; 1997.
3.Helfenstein M,Goldenfum MA,Siena C.Occupational low back pain.Rev Assoc Med Bras 2010;56:583-9.
4.Armed Forces Health Surveillance Center.Ambulatory visits among members of active components,U.S.Armed Forces,2006.Annual Summary 2007.April 2007.
5.Armed Forces Health Surveillance Center.Absolute and relative morbidity burdens attributable to various illnesses and injuries,U.S.Armed Forces,2011.MSMR 2012;19:4-9.
6.Reynolds K,Cosio-Lima L,Creedon J,Gregg R,Zigmont T.Injury occurrence and risk factors in construction engineers and combat artillery soldiers.Mil Med 2002;167:971-7.
7.Lincoln AE,Smith GS,Amoroso PJ,Bell NS.The natural history and risk factors of musculoskeletal conditions resulting in disability among US Army personnel.Work 2002;18:99-113.
8.Kent PM,Keating JL.The epidemiology of low back pain in primary care.Chiropr Osteopat 2005;13:13.
9.Hestbaek L,Leboeuf-Yde C,Manniche C.Low back pain: what is the long-term course? A review of studies of general patient populations.Eur Spine J 2003;12:149-65.
10.Cassidy JD,Cote P,Carroll LJ,Kristman V.Incidence and course of low back pain episodes in the general population.Spine 2005;30:2817-23.
11.Hoy D,Brooks P,Blyth F,Buchbinder R.The epidemiology of low back pain.Best Pract Res Clin Rheumatol 2010;24:769-81.
12.Greene HS,Cholewicki J,Galloway MT,Nguyen CV,Radebold A.A history of low back injury is a risk factor for recurrent back injuries in varsity athletes.Am J Sports Med 2001;29:795-800.
13.Milgrom C,Finestone A,Lubovsky O,Zin D,Lahad A.A controlled randomized study of the effect of training with orthoses on the incidence of weight bearing induced back pain among infantry recruits.Spine 2005;30:272-5.
14.Nadler SF,Moley P,Malanga GA,Rubbani M,Prybicien M,Feinberg JH.Functional deficits in athletes with a history of low back pain: a pilot study.Arch Phys Med Rehabil 2002;83:1753-8.
15.Hamill J,van Emmerik RE,Heiderscheit BC,Li L.A dynamical systems approach to lower extremity running injuries.Clin Biomech (Bristol,Avon) 1999;14:297-308.
16.Seay JF.Lumbo-sacral loads and pelvis trunk coordination in runners with chronic and resolved acute low back pain.Amherst,MA: University of Massachusetts Amherst; 2008.[Dissertation].
17.Seay JF,Van Emmerik RE,Hamill J.Influence of low back pain status on pelvis-trunk coordination during walking and running.Spine 2011;36:E1070-9.
18.Marras WS.Occupational low back disorder causation and control.Ergonomics 2000;43:880-902.
19.Nahit ES,Macfarlane GJ,Pritchard CM,Cherry NM,Silman AJ.Short term influence of mechanical factors on regional musculoskeletal pain: a study of new workers from 12 occupational groups.Occup Environ Med 2001;58:374-81.
20.Peek-Asa C,McArthur DL,Kraus JF.Incidence of acute low-back injury among older workers in a cohort of material handlers.J Occup Environ Hyg 2004;1:551-7.
21.Prado-Leon LR,Celis A,Avila-Chaurand R.Occupational lifting tasks as a risk factor in low back pain: a case-control study in a Mexican population.Work 2005;25:107-14.
22.Hoogendoorn WE,van Poppel MN,Bongers PM,Koes BW,Bouter LM.Physical load during work and leisure time as risk factors for back pain.Scand J Work Environ Health 1999;25:387-403.
23.Buller MJ,Tharion WJ,Karis A,Santee W,Mullen S,Hoyt R.Real time physiological monitoring of encapsulated team members of the 1st Civil Support Team—Weapons of Mass Destruction (CST-WMD).Natick,MA: U.S.Army Research Institute of Environmental Medicine; 2007.
24.Sharp MA,Patton JF,Vogel JA.A database of physically demanding tasks performed by U.S.Army soldiers.Human Factors and Ergonomics Society 40th Annual Meeting Proceedings.Philadelphia,PA.September 2-6,1996.p.673-7.
25.Seay JF,Sauer SG,Frykman PN,Roy TC.A history of low back pain affects pelvis and trunk mechanics during a sustained lift/lower task.Ergonomics 2013;56:944-53.
26.Hamill J,van Emmerick REA.Variability and stability: a dynamical systems perspective.J Appl Biomech 2000;16:392-3.
27.Selles RW,Wagenaar RC,Smit TH,Wuisman PI.Disorders in trunk rotation during walking in patients with low back pain: a dynamical systems approach.Clin Biomech (Bristol,Avon) 2001;16:175-81.
28.Lamoth CJ,Meijer OG,Wuisman PI,van Dieen JH,Levin MF,Beek PJ.Pelvis-thorax coordination in the transverse plane during walking in persons with nonspecific low back pain.Spine 2002;27:E92-9.
29.Seay JF,Van Emmerik RE,Hamill J.Low back pain status affects pelvis-trunk coordination and variability during walking and running.Clin Biomech (Bristol,Avon) 2011;26:572-8.
30.Seay JF,Van Emmerik RE,Hamill J.Trunk bend and twist coordination is affected by low back pain status during running.Eur J Sport Sci 2014;14:563-8.
31.Peters BT,Haddad JM,Heiderscheit BC,Van Emmerik RE,Hamill J.Limitations in the use and interpretation of continuous relative phase.J Biomech 2003;36:271-4.
32.Cohen J.Statistical power analysis for the behavioral sciences.2nd ed.Hillsdale,NJ: L.Erlbaum Associates; 1988.
33.Al-Obaidi SM,Al-Zoabi B,Al-Shuwaie N,Al-Zaabie N,Nelson RM.The influence of pain and pain-related fear and disability beliefs on walking velocity in chronic low back pain.Int J Rehabil Res 2003;26: 101-8.
34.Jones SL,Henry SM,Raasch CC,Hitt JR,Bunn JY.Individuals with non-specific low back pain use a trunk stiffening strategy to maintain upright posture.J Electromyogr Kinesiol 2012;22:13-20.
35.Hodges PW,Tucker K.Moving differently in pain: a new theory to explain the adaptation to pain.Pain 2011;152:S90-8.
36.Nelson JM,Walmsley RP,Stevenson JM.Relative lumbar and pelvic motion during loaded spinal flexion/extension.Spine 1995;20: 199-204.
杂志排行

Journal of Sport and Health Science的其它文章
- Non-linearity in the dynamic world of human movement
- Comparing dynamical systems concepts and techniques for biomechanical analysis
- Multi-scale interactions in interpersonal coordination
- Can coordination variability identify performance factors and skill level in competitive sport? The case of race walking
- Multiscale entropy: A tool for understanding the complexity of postural control
- Postural control deficits identify lingering post-concussion neurological deficits