血清总唾液酸、唾液酸酶和超敏C反应蛋白联合检测对急性心肌梗死患者诊断和预后评估的临床价值
2016-03-13周方元李艳戴雯
周方元,李艳,戴雯
(武汉大学人民医院检验科,湖北 武汉 430060)
血清总唾液酸、唾液酸酶和超敏C反应蛋白联合检测对急性心肌梗死患者诊断和预后评估的临床价值
周方元,李艳,戴雯
(武汉大学人民医院检验科,湖北 武汉 430060)
目的 探讨联合检测血清总唾液酸(TSA)、唾液酸酶(NEU)及超敏C反应蛋白(hs-CRP)在急性心肌梗死(AMI)患者的诊断和预后评估中的临床价值。方法 收集2015年8~12月武汉大学人民医院的AMI患者210例(病例组)及同期体检健康者99例(对照组),其中病例组患者根据AMI类型分为ST段抬高型AMI组(STEMI组)和非ST段抬高型AMI组(NSTEMI组);根据AMI部位,分为前壁梗死组和下壁梗死组;根据是否院内死亡,分为院内死亡组和存活组。分别检测各组受检者的血清TSA、NEU、hs-CRP的浓度,并对其结果进行统计学分析。结果 病例组患者的血清TSA水平为717 mg/L,明显高于对照组的568 mg/L,差异有统计学意义(U=2 346.5,P<0.01),血清NEU水平为16.69 ng/mL,明显高于对照组的13.32 ng/mL,差异有统计学意义(U=5 465.0,P<0.01),血清hs-CRP水平为14.34 mg/dL,明显高于对照组的0.35 mg/dL,差异有统计学意义(U=458.0,P<0.01);STEMI组和NSTEMI组之间各指标差异无统计学意义(P>0.05);前壁梗死组患者的血清TSA水平为746 mg/L,明显高于下壁梗死组的648 mg/L,血清hs-CRP水平为19.63 mg/dL,明显高于下壁梗死组的7.80 mg/dL,差异均有统计学意义(U=2 302.5、2 169.5,P均<0.01);院内死亡组的TSA水平为948 mg/L,明显高于存活组的697 mg/L,hs-CRP水平为58.37 mg/mL,明显高于存活组的11.00 mg/mL,差异均有统计学意义(U=1006.5、1052.0,P均<0.01);AMI患者血清TSA与hs-CRP呈显著负相关(r=0.623,P<0.01);绘制受试者工作特征曲线后显示,用血清TSA诊断AMI时,曲线下面积为86.0%(P<0.01),用血清hs-CRP诊断AMI时,曲线下面积为97.3%(P<0.01),联合血清TSA和hs-CRP诊断AMI时,曲线下面积为97.4%(P<0.01)。结论 联合检测血清TSA、NEU和hs-CRP对于AMI患者的诊断和预后评估都具有重要意义。
急性心肌梗死;唾液酸;唾液酸酶;超敏C反应蛋白;诊断;预后评估
急性心肌梗死(acute myocardial infarction,AMI)是在冠状动脉狭窄的基础上,由于粥样硬化斑块破裂,导致血小板在破裂处聚集形成血栓而引起的心肌缺血和坏死[1]。我国AMI的发病率为45/100 000~55/100 000,且国内的流行病学调查显示,AMI在小于60岁人群中的发病率逐渐升高,AMI的发病年龄呈现年轻化趋势[2-3]。目前,临床上主要依靠特征性的心电图变化、血清标志物的动态变化等来诊断AMI和监测AMI病情变化。AMI的血清标志物除肌酸激酶同工酶(CK-MB)及心肌钙蛋白I(cTnI)等特异性心肌坏死标志物外,还常用急性炎症标志物超敏C反应蛋白(high sensitivity C-reactive protein,hs-CRP)动态监测病情变化。当机体发生炎症时,特别是急性炎症时,血清中唾液酸(SA)的主要来源是富含SA的炎症反应性蛋白[4],这一过程是通过唾液酸酶(neuramidinase,NEU)的作用完成的[5]。因此,本研究拟通过检测AMI患者心肌梗死发生后不同时间段内的血清总唾液酸(total sialic acid,TSA)、hs-CRP、NEU等指标的含量,来评价血清TSA与hs-CRP的相关性、变化趋势及对AMI的诊断能力,以此评估血清总唾液酸(TSA)、NEU及hs-CRP联合应用对AMI的临床价值。
1 资料与方法
1.1 一般资料 实验对象为2015年8~12月期间武汉大学人民医院心内科因AMI入院的病例且符合入选标准者。入选标准:(1)符合AMI诊断标准[6-10];(2)从发病到入院的时间<24 h;(3)临床资料较为完整全面。共收集到AMI病例210例。另收集了99名同期来院的健康体检者,归为对照组。此外,根据AMI的类型,将病例组再分为ST段抬高型心肌梗死组(STEMI组,98例)和非ST段抬高型心肌梗死组(NSTEMI组,112例);根据AMI的梗死部位,将病例组再分为前壁梗死组(103例)和下壁梗死组(67例),其余患者为其他部位的心肌梗死,未纳入本分组项目;根据是否发生院内死亡,将病例组再分为院内死亡组(33例)和存活组(177例)。实验对象排除标准:(1)入院时同时患有其他严重疾病者,如:肿瘤、感染、卒中、免疫学疾病、糖尿病及明显的其他原因所致肝肾功能异常;(2)在住院期间发生感染中毒性休克等并发症者;(3)已经接受降脂或溶栓治疗者;(4)已进行过透析治疗者;(5)年龄<18岁者;(6)临床资料不完善,缺失关键信息者;(7)住院时间<2 d者。
1.2 观察指标与检测方法 观察两组受检者的血清TSA、NEU和hs-CRP水平。(1)标本采集:于清晨空腹静脉采血两管,每管约3 mL,离心后取上清,所有标本均无溶血。(2)取血清样本100µL于生化仪样品杯中,编号后上全自动生化分析仪机器自动检测。TSA采用酶分析法测定,hs-CRP采用免疫比浊法测定;另一管-80℃保存,待统一ELISA检测NEU水平。检验过程严格按照试剂和仪器操作说明书进行。
1.3 统计学方法 采用SPSS22.0软件进行统计学分析。采用Kolmogorov-Smironv检验(K-S检验)对数据进行正态分布检验。计量资料用中位数(四分位数)表示,两组间数据比较采用Mann-Whitney U检验;多组数据之间比较采用非参数Kruskal-Wallis H检验。计数资料比较采用χ2检验。各指标之间的相关性采用Spearman相关系数进行描述。以受试者工作特征曲线(Receiver operating characteristic curve,ROC曲线)评估各指标及联合指标诊断AMI的能力,以二元Logistic回归计算两指标联合后的预测概率[11]。以P<0.05为差异有统计学意义。
2 结果
2.1 两组受检者的一般资料比较 经K-S检验发现各组数据均呈非正态分布。经χ2检验得出,对照组与AMI组之间,在性别组成上差异无统计学意义(χ2= 0.713,P=0.652)。经Mann-Whitney U检验得出,对照组与AMI组年龄构成差异无统计学意义(U=10 065.0,P=0.652)。与对照组比较,AMI组的血清TSA、NEU及hs-CRP水平都明显升高,差异均有统计学意义(U值分别为2 346.5、5 465.0、458.0,P均<0.01),见表1。

表1 两组受检者一般资料比较
2.2 血清TSA、NEU和hs-CRP与AMI类型、梗死部位及院内死亡的关系分析 根据各相关因素分组后,经Mann-Whitney U检验得出,在STEMI组与NSTEMI组之间,血清TSA、NEU及hs-CRP水平差异均无统计学意义(U=5 235.0、5 277.5、4 844.0,P= 0.565、0.983、0.248);与下壁梗死组比较,前壁梗死组的血清TSA和hs-CRP水平明显升高(U=2 302.5、216.5,P均<0.01),而血清NEU水平差异无统计学意义(U=3 080.0,P=0.354);与存活组比较,院内死亡组的血清TSA、hs-CRP水平明显升高(U=1 006.5、1 052.0,P均<0.01),而血清NEU水平差异无统计学意义(U= 2 514.0,P=0.384),见表2、表3和表4。

表2 血清TSA、NEU和hs-CRP与AMI类型的关系
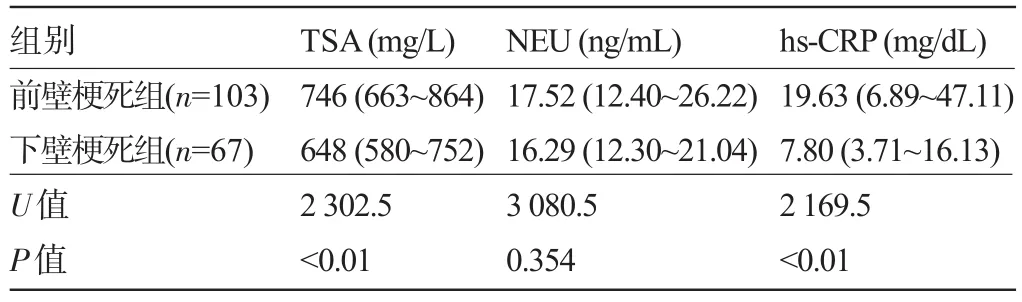
表3 血清TSA、NEU和hs-CRP与AMI梗死部位的关系
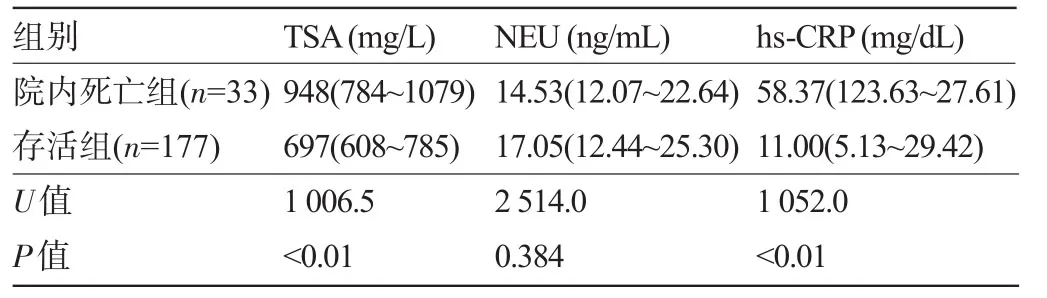
表4 血清TSA、NEU和hs-CRP与AMI院内死亡的关系
2.3 AMI患者血清TSA与hs-CRP的相关性 在AMI患者中,血清TSA与hs-CRP水平呈显著正相关(r=0.623,P<0.01)
2.4 血清TSA和hs-CRP诊断AMI的ROC曲线 绘制ROC曲线后显示,血清TSA诊断AMI的ROC曲线下面积为86.0%(P<0.01),当约登指数(Youden index,YI)最大时,YI=0.669,血清TSA浓度为645 mg/L,灵敏度为68.1%,特异度为98.8%。血清hs-CRP诊断AMI的ROC曲线下面积为97.3%(P<0.01),当YI最大时,YI=0.859,血清hs-CRP浓度为2.02 mg/dL,灵敏度为89.4%,特异度为97.3%。联合血清TSA与hs-CRP诊断AMI的ROC曲线下面积为97.4%(P<0.01),当YI最大时,YI=0.867,灵敏度为89.4%,特异度为97.3%,见图1。

图1 血清TSA、hs-CRP、TSA联合hs-CRP诊断AMI的ROC曲线
3 讨论
AMI是在动脉粥样硬化斑块破裂、糜烂或血栓形成的基础上导致冠状动脉闭塞,进而引起的急性心肌血流量和氧供不足[12]。AMI作为一种致死性的冠心病,是世界上主要死亡原因之一[13],尽管运用了包括溶栓、经皮冠状动脉介入治疗(percutaneous coronary intervention,PCI)和冠状动脉旁路移植术(coronary artery bypass grafting,CABG)等在内的血运重建技术,已成功降低了AMI患者的死亡率,但是AMI患者仍然面临着一定的院内死亡风险[14],并且血运重建术自身也可引发一些严重的并发症,如支架内血栓形成、缺血再灌注损伤和PCI后无复流现象等[15]。因此,AMI及其并发症的防治,受到越来越多的关注。
SA和hs-CRP都是由肝脏合成的一种全身性炎症反应急性期非特异性标志物,正常状态下二者在血清中的含量很少,都是心血管事件危险性强有力的预测因子[16-17]。本研究中证实,在AMI患者中,血清TSA和hs-CRP水平都明显升高,而与之相关的NEU的血清水平也随之明显升高,一方面说明检测血清TSA和hs-CRP对于AMI的诊断有一定的临床意义,另一方面说明在发生AMI时,血清中NEU的水平明显上调,将SA从富含SA的急性时相反应蛋白中分解下来,侧面印证了急性炎症时血清中的SA主要来源于急性时相反应蛋白这一假设,为进一步研究SA与hs-CRP的关系奠定了基础。
hs-CRP和TSA不仅可以监测机体的炎症状态,对于AMI的病情也有一定的预估作用[18-19]。本研究中发现,前壁心肌梗死患者血清TSA及hs-CRP水平都显著高于下壁心肌梗死患者,这与临床上前壁心肌梗死患者临床症状更危急,死亡率更高是相一致的[20];而院内死亡的AMI患者血清TSA及hs-CRP水平都显著高于存活组,说明二者联合检测可以初步预估AMI患者的院内死亡危险性。不仅如此,研究者还发现,STEMI患者接受PCI术后,血清内高水平的hs-CRP与低心肌灌注量和更长的住院时间有关[21];而血清高水平的TSA是AS及其并发症的长效标志物,与血管病变支数有关[22]。可见,血清TSA与hs-CRP对于AMI的预后评估具有重要意义。
急性冠脉供血不足时,心肌细胞受到损伤而导致血管收缩和白细胞浸润,由此激活和启动炎性介质的释放,炎性敏感蛋白的增加正是对这些介质的响应[23]。许多急性时相反应蛋白在其寡糖侧链的终末端位置,都连接着唾液酸残基而被糖基化,因此检测SA有助于炎症疾病的诊断[24]。血清TSA和hs-CRP具有强烈的相关性。本研究中发现,在AMI患者组,TSA与hs-CRP的相关性达到0.623,这说明TSA与hs-CRP的含量关系密切,可见,血清TSA含量的变化是与hs-CRP的含量密切相关的,在AMI发生后,检测血清TSA的含量可以反映机体的炎症状态。
当用血清TSA单独诊断AMI时ROC曲线下面积为86.0%,用血清hs-CRP单独诊断AMI时ROC曲线下面积为97.3%,联合二者诊断AMI时曲线下面积略微升高为97.4%,且能把持较高的灵敏度和特异度,说明联合检测血清TSA和hs-CRP可以改善AMI诊断的灵敏度和特异度,提高其诊断能力。
目前国内外检测血清TSA,基本采用全自动生化仪的酶法分析,能够快速、准确地检测血清TSA。而SA的物理分析方法有多种,包括薄层层析法、分光光度法、核磁共振法[25]、高效液相色谱法、高效液相色谱质谱联用技术等。这些技术不但可以用于生物样品中SA的分离和测定,还可以区分不同类型的SA[26],为SA的进一步研究提供了多样而可靠的手段。
综上所述,血清TSA和hs-CRP水平在AMI患者中升高,联合检测二者、辅以NEU的检测,不仅可以提高其诊断AMI的能力,还可以初步评估AMI患者的严重程度和院内死亡的危险性,具有重要的临床应用价值。
[1]Gao Y,Jiang D,Zhang B,et al.Renal insufficiency was correlated with 2-year mortality for rural female patients with ST-segment elevation acute myocardial infarction after reperfusion therapy:a multicenter,prospective study[J].BMC Cardiovasc Disord,2015,15(1): 1-10.
[2]胡善联,龚向光.中国急性心肌梗塞的疾病经济负担[J].中国卫生经济,2003,22(5):32-34.
[3]梁文生,蒋德谦,刘启明.中青年急性心肌梗死病人的生活方式及冠状动脉病变特征分析[J].中国心血管杂志,2007,12(2):118-123.
[4]Süer Gökmen S,Kazezoðlu C,Sunar B,et al.Relationship between serum sialic acids,sialic acid-rich inflammation-sensitive proteins and cell damage in patients with acute myocardial infarction[J].Clin Chem Lab Med,2006,44(2):199-206.
[5]Miyagi T,Yamaguchi K.Mammalian sialidases:physiological and pathological roles in cellular functions[J].Glycobiology,2012,22 (7):880-896.
[6]Chinese Society of Cardiology of Chinese MedicalAssociation.Guideline for diagnosis and treatment of patients with unstable angina and non-ST-segment elevation myocardial infarction[J].Chinese Journal of Cardiology,2007,35(4):295-304.
[7]Chinese Society of Cardiology of Chinese Medical Association.Recommendation of the application of universal definition of myocardial infarction in China[J].Chinese Journal of Cardiology,2008,36(10): 867-869.
[8]China Society of Cardiology of Chinese Medical Association.Guideline for diagnosis and treatment of patients with ST-elevation myocardial infarction[J].Chinese Journal of Cardiology,2010,38(8): 675-690.
[9]Jneid H,Anderson JL,Wright RS,et al.2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non-ST-elevation myocardial infarction(updating the 2007 guideline and replacing the 2011 focused update):a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines[J].Journal of the American College of Cardiology,2012,60(7):645-681.
[10]Amsterdam EA,Wenger NK,Brindis RG,et al.2014 AHA/acc guideline for the management of patients with Non-ST-Elevation acute coronary syndromes:a report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines[J]. Journal of the American College of Cardiology,2014,64(24): e139-e228.
[11]Spruijt OA,Bogaard HJ,Heijmans MW,et al.Predicting pulmonary hypertension with standard computed tomography pulmonary angiography[J].Int J Cardiovasc Imaging,2015,31(4):871-879.
[12]Libby P.Current concepts of the pathogenesis of the acute coronary syndromes[J].Circulation,2001,104(3):365-372.
[13]White HD,Chew DP.Acute myocardial infarction[J].The Lancet, 2008,372(9638):570-584.
[14]Ma XJ,Yin HJ,Chen KJ.Appraisal of the prognosis in patients with acute myocardial infarction treated with primary percutaneous coronary intervention[J].Chinese Journal of Integrative Medicine,2009, 15(3):236-240.
[15]Tanaka A,Kawarabayashi T,Nishibori Y,et al.No-reflow phenomenon and lesion morphology in patients with acute myocardial infarction[J].Circulation,2002,105(18):2148-2152.
[16]Rajesh Kumar G,Mrudula Spurthi K,Kishore Kumar G,et al.Evaluation of hs-CRP levels and interleukin 18(-137G/C)promoter polymorphism in risk prediction of coronary artery disease in first degree relatives[J].PLoS One,2015,10(3):e0120359.
[17]Knuiman MW,Watts GF,Divitini ML.Is sialic acid an independent risk factor for cardiovascular disease?A 17-year follow-up study in Busselton,Western Australia[J].Ann Epidemiol,2004,14(9): 627-632.
[18]Cai MQ,Yang LH,Zhou XJ,et al.Clinical significance of detecting serum levels of cTnI,TNF-α and Hs-CRP in patients with acute myocardial infarction[J].Progress in Modern Biomedicine,2012,12(5): 2940-2942.
[19]Parkash A,Singla P,Seth M,et al.Study of serum total sialic acid and its correlation with atherogenic index in cases of cute myocardial infarction[J].International Journal of Pharma&Bio Sciences,2011, 2(2):8-14.
[20]Yousef ZR,Redwood SR,Bucknall CA,et al.Late intervention after anterior myocardial infarction:effects on left ventricular size,function,quality of life,and exercise tolerance:Results of the Open Artery Trial(TOAT Study)[J].Journal of the American College of Cardiology,2002,40(5):869-876.
[21]Caðli KE,Topaloðlu S,Aras D,et al.The significance of admission hs-CRP in patients undergoing primary percutaneous intervention for acute myocardial infarction[J].Turk Kardiyol Dern Ars,2009,37(1): 19-25.
[22]Lindberg G.Resialytion of sialic acid deficit vascular endothelium circulation cells and macromolecules may counteract the development of atherosclerosis:a hypothesis[J].Atherosclerosis,2007,192 (2):243-245.
[23]Lv S,Liu Y,Zou Z,et al.The impact of statins therapy on disease activity and inflammatory factor in patients with rheumatoid arthritis:a meta-analysis[J].Clin Exp Rheumatol,2015,33(1):69-76.
[24]Gökmen SS,Kiliçli1 G,Özçelik F,et al.Serum total and lipid-bound sialic acid levels following acute myocardial infarction[J].Clin Chem Lab Med,2000,38(12):1249-1255.
[25]Schauer R.Sialic acids:chemistry,metabolism,and function[M]. New York:Springer,1982:173-193.
[26]Nie H,Li Y,Sun XL.Recent advances in sialic acid-focused glycomics[J].J Proteomics,2012,75(11):3098-3112.
Clinical value of combined detection of serum total sialic acid,sialidase and high sensitivity C-reactive protein inpatients with acute myocardial infarction.
ZHOU Fang-yuan,LI Yan,DAI Wen.Department of Clinical Laboratory, Renmin Hospital of Wuhan University,Wuhan 430060,Hubei,CHINA
Objective To evaluate the clinical value of combined detection of serum total sialic acid(TSA), neuramidinase(NEU)and high sensitivity C-reactive protein(hs-CRP)in the diagnosis and prognosis evaluation of acute myocardial infarction(AMI).Methods Ninety-nine healthy subjects(control group)and 210 AMI patients(case group)who visited the Renmin Hospital of Wuhan University from August to December 2015 were selected as the study subjects.According to AMI type,the case group was divided into ST segment elevation type AMI group(STEMI group) and non ST segment elevation type AMI group(NSTEMI group).According to AMI site,the patients were divided into anterior wall infarction group and inferior wall infarction group.According to whether the hospital death occurred,the case group was divided into the hospital death group and survival group.The levels of serum TSA,NEU and hs-CRP were detected and then compared between groups.Results Compared with the control group,the levels of TSA,NEU, and hs-CRP in case group were significantly increased[717(612~834)mg/L vs 568(534~605)mg/L,U=2 346.5,P<0.01;16.69 ng/mL vs 13.32 ng/mL,U=5 465.0,P<0.01;14.34 mg/dL vs 0.35 mg/dL,U=458.0,P<0.01].There was no statistically significant difference in the levels of TSA,NEU,and hs-CRP between STEMI group and NSTEMI group.Compared with the inferior wall infarction group,the serum TSA level and hs-CRP level in the anterior wall infarction group were significantly increased(746 mg/L vs 648 mg/L,U=2 302.5,P<0.01;19.63 mg/dL vs 7.80 mg/dL,U=2 169.5,P<0.01). Compared with the survival group,the level of serum TSA and hs-CRP in the hospital death group were significantly increased(948 mg/L vs 697 mg/L,U=1 006.5,P<0.01;58.37 mg/mL vs 11.00 mg/mL,U=1 052.0,P<0.01).Spearman correlation analysis showed that serum TSA and hs-CRP levels were significantly positively correlated(r=0.623,P<0.01)in AMI patients.After drawing the receiver operating characteristic curve,the area under the curve was 86.0%(P<0.01) when the serum TSA was used for the diagnosis of AMI,and the area under the curve was 97.3%(P<0.01)when the serum hs-CRP was used for the diagnosis of AMI.The area under the curve was 97.4%(P<0.01)when combined serum TSA and hs-CRP was used in the diagnosis of AMI.Conclusion The combined detection of serum TSA,NEU and hs-CRP has a certain clinical value for the diagnosis and prognosis evaluation ofAMI.
Acute myocardial infarction;Sialic acid;Neuramidinase;High sensitivity C-reactive protein;Diagnosis;Prognosis evaluation
R542.2+2
A
1003—6350(2016)15—2428—04
10.3969/j.issn.1003-6350.2016.15.006
2016-03-14)
国家自然科学基金(编号:81572096)
周方元。E-mail:184546159@qq.com
