Intrahepatic distant recurrence following complete radiofrequency ablation of small hepatocellular carcinoma: risk factors and early MRI evaluation
2015-12-24
Shanghai, China
Intrahepatic distant recurrence following complete radiofrequency ablation of small hepatocellular carcinoma: risk factors and early MRI evaluation
Ruo-Fan Sheng, Meng-Su Zeng, Zheng-Gang Ren, Sheng-Long Ye, Lan Zhang and Cai-Zhong Chen
Shanghai, China
BACKGROUND: Radiofrequency ablation (RFA) is related to a high intrahepatic distant recurrence (IDR) rate, and the associations between IDR and relevant imaging features have not yet been fully investigated. This study aimed to determine both clinical and imaging risk factors of IDR after complete RFA for HBV-related small hepatocellular carcinoma (HCC) (≤3 cm).
METHODS: Thirty-five patients (29 men and 6 women; mean age 60.7 years) with 40 HBV-related small HCCs who underwent complete RFA were included in our study. The incidence and potential clinical and MR imaging risk factors for IDR after RFA were assessed using the Kaplan-Meier method, the log-rank test and a stepwise Cox hazard model.
RESULTS: The median follow-up period was 25 (4-45) months, and IDR was observed in 20 (57.1%) patients. The 12- and 24-month cumulative IDR-free survival rates were 76.7% and 61.3%, respectively. Univariate analysis revealed that pretreatment albumin <3.5 g/dL (P=0.026), multinodular tumor (P=0.032), ablative margin <3 mm (P=0.007), no or disrupted periablational enhancement within 24 hours (P=0.001) and at 1 month (P=0.043) after RFA, and hyperintensity of the central ablative zone on T1-weighted images (T1WI) at 1 month after RFA (P=0.004) were related to IDR. Multivariate analysis showed that pretreatment albumin <3.5 g/dL (P=0.032), multinodular tumor (P=0.012), no or disrupted periablational enhancement within 24 hours after RFA (P=0.001), and hyperintensity of the central ablative zone on T1WI at 1 month after RFA (P=0.003) were independent risk factors for IDR. During the 1-month follow-up, the apparent diffusion coefficient exhibited an up-and-down evolution without significant value in the prediction of IDR following RFA.
CONCLUSIONS: Patients with HBV-related small HCC had a high IDR rate after RFA. The risk factors included low serum albumin, multiple nodules, lesions with no or disrupted periablational enhancement and persistent hyperintensity in the central ablative zone on T1WI within 1 month after RFA.
(Hepatobiliary Pancreat Dis Int 2015;14:603-612)
hepatocellular carcinoma;
radiofrequency ablation;
recurrence;
magnetic resonance imaging
Introduction
In recent decades, the incidence of primary liver can
cer has significantly increased. It is the fifth most
frequently diagnosed cancer in men (seventh in women) and the second most frequent cause of cancer death (sixth in women) worldwide; hepatocellular carcinoma (HCC) is the most common type of liver cancer.[1]Approximately 70%-90% of HCCs worldwide are attributable to underlying chronic hepatitis B or C, and HBV infection is the dominant risk factor in Eastern Asia and sub-Saharan Africa.[2,3]The present study focused on the patients with HBV-related small HCC.
The optimum therapy for patients with HCC is surgical resection or orthotopic liver transplantation. However, only 9%-27% of patients are eligible for resection, and a shortage of donors limits the transplantation.[4]Local ablative therapy, particularly radiofrequency abla-tion (RFA), is a suboptimal modality and HCC patients treated with RFA have relative good outcomes. Many studies[5-7]confirmed that there are no significant differences in overall survival between RFA and resection for HCC, especially small tumors less than 3 cm in diameter. Compared with surgical resection, RFA has many advantages, such as reduced morbidity and mortality, low cost, and good repeatability.[8]However, RFA has been associated with a higher recurrence rate and especially frequent intrahepatic distant recurrence (IDR).[5-7]It is important to elucidate the incidence and risk factors of IDR to improve prognosis. In addition, because complete necrosis can be achieved in more than 90% of HCC tumors smaller than 3 cm[9]and the complete tumor ablation rate decreases when the tumor size exceeds 3 cm,[5]we chose lesions less than 3 cm, which coincided with the Barcelona Clinic Liver Cancer (BCLC) current strategy.[10]
To date, few studies have analyzed the risk factors for IDR following RFA alone, and its associations with relevant imaging features have not yet been fully investigated.[11,12]Because MR imaging (MRI) is a widely used imaging tool to investigate HCC in clinical practice, the present study aimed to investigate not only the clinical, but also the potential MRI risk factors of IDR after complete RFA for HBV-related small HCC. The study focused on early imaging changes before and within 1 month after RFA to provide early implications for advanced warning and to assist in the establishment of an appropriate follow-up schedule for different individuals.
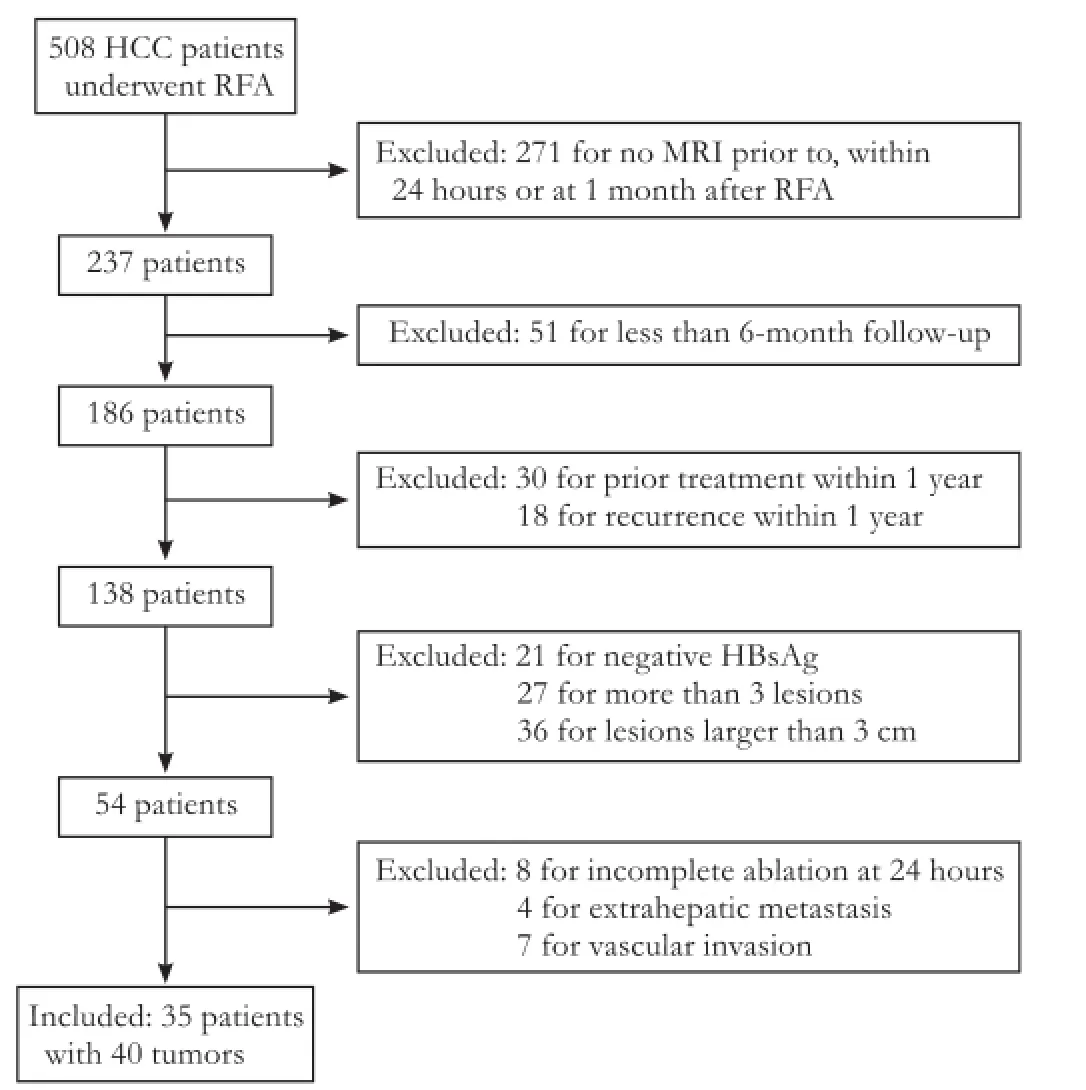
Fig. 1. Flowchart of the inclusion and exclusion procedures performed in this study.
Methods
Patients
This study was approved by the institutional review board (Approval number: B2014-002) and the need for informed consent was waived. Between January 2010 and December 2011, 508 HCC patients treated with percutaneous RFA were retrospectively identified through a review of the database of our institution. The inclusion criteria were as follows: patients with single or multiple (n≤3) HCC lesions smaller than 3 cm in diameter; positive HBsAg; abdominal contrast-enhanced MR examinations within one month before RFA and regular follow-up (including examinations within 24 hours and at 1 month after RFA) for at least 6 months unless the patient died or IDR occurred; and no previous treatment for HCC or a minimum of one-year disease-free survival after the previous treatment. The exclusion criteria were incomplete ablation at the immediate follow-up within 24 hours after RFA and the presence of extrahepatic metastasis or vascular invasion (Fig. 1).
The diagnosis of HCC was established before RFA by fine-needle aspiration cytology for 9 lesions in 9 patients and by diagnostic imaging criteria based on the latest AASLD practice guidelines for the remaining patients.[13]Thirty-five patients with 40 small HCCs were included in our study; 5 patients harbored 2 lesions. The baseline patient characteristics are summarized in Table 1. The patients were predominantly elderly (mean age 60.7 years) and male (82.9%). Fifteen patients were treated with surgical resection (n=8), RFA (n=6) or transcatheter arterial chemoembolization (TACE;n=1); all tumors in these 15 patients were newly developed lesions, and there was no evidence of tumor viability after previous treatment.
Radiofrequency ablation (RFA)
The patients were treated with two different types of RF systems: (i) an internally cooled single electrode (Cool-Tip; Radionics, Burlington, MA, USA) and (ii) multi-tined expandable StarBurst and StarBurst XL electrodes (RITA Medical System, Mountain View, CA, USA). Power settings and exposure times were selected according to the recommendations provided by each manufacturer. The procedures were performed percutaneously in real-time ultrasonic guidance under local anesthetics and intramuscular sedation. Before performing the RFA, intravenous antibiotics were administered. Hot withdrawal was performed to prevent oozing and tumor seeding, and the target temperature at the end of ablation was>60 ℃. Our procedure was aimed to ablate the tumor assection thickness, 5 mm; no intersection gap; matrix, 270×360) after the intravenous administration of gadopentetate dimeglumine (Magnevist; Bayer HealthCare, Berlin, Germany). Gadopentetate dimeglumine was administered at a dose of 0.1 mmol/kg at a rate of 2 mL/sec, followed by a 20 mL saline flush using a power injector (Spectris; Medrad, Pittsburgh, PA, USA). The acquisitions were performed at 25, 60, and 180 seconds after contrast administration during the hepatic arterial, portal, and delayed phase, respectively. The field of view was optimized to the patients' body habitus at 285×214-308×380 mm. well as a 5-10 mm peripheral margin of adjacent normal liver parenchyma. Patients with multiple nodules were treated with the same RF procedure.
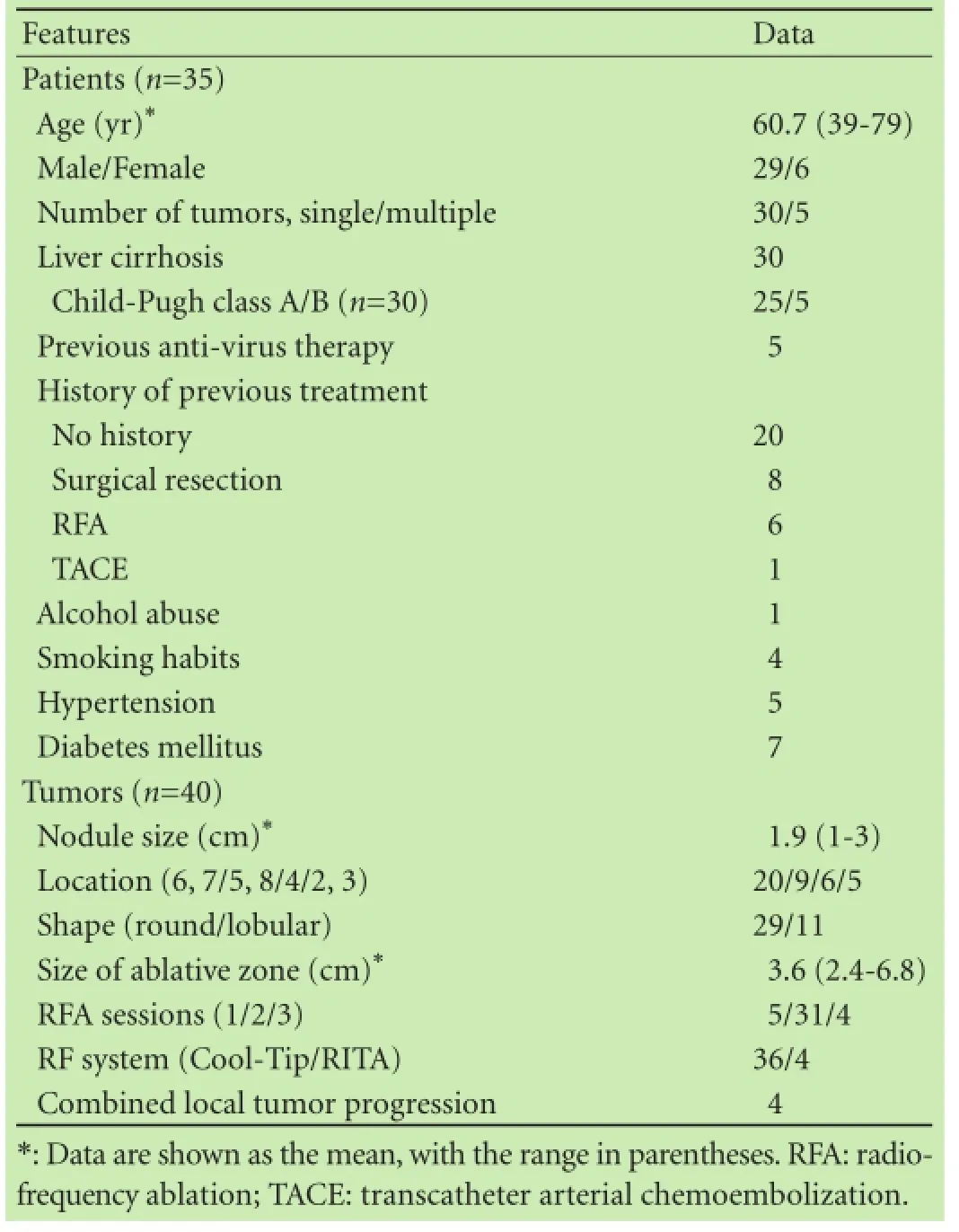
Table 1. Baseline features of the patients and tumors
Imaging protocol
MRI was performed using a 1.5-Tesla (T) scanner (Avanto; Siemens, Erlangen, Germany) with a peak gradient amplitude of 45 mT/m. An eight-channel torso phasedarray coil was centered over the liver. The conventional MR protocol used in this study included transverse respiratory-navigated T2-weighted fat-suppressed turbo spin echo sequence (TR/TE=3500/84 msec; section thickness, 5 mm; and intersection gap, 1 mm; matrix, 168×320); transverse T1-weighted in-phase and opposed-phase gradient echo [TR/TE=6.8/2.35 (in-phase), 4.75 (opposedphase) msec; section thickness, 5 mm; intersection gap, 1 mm; matrix, 180×320]. Diffusion-weighted imaging (DWI) was required with a transverse single-shot spinecho echo-planar sequence (TR/TE=2400/66 msec; section thickness, 5 mm; intersection gap, 1 mm; matrix, 168×320) with twobvalues (0 and 500 sec/mm2). Dynamic imaging was performed with a transverse breathhold T1-weighted 3-dimensional volumetric interpolated body examination sequence (TR/TE=5.0/2.3 msec;
Post-RFA follow-up
The follow-up period was determined as the interval from the date of ablation to the diagnosis of IDR, date of death, or September 30, 2013. For the early evaluation of the therapeutic response or potential complications, contrast-enhanced MRI was performed within 24 hours, and the subsequent follow-up MRI study was carried out one month later. Subsequent follow-ups were repeated every 3 months with contrast-enhanced CT, MRI or ultrasound examination until one year after RFA; followups were then conducted every 4 to 6 months according to the risks for recurrences. Chest X-ray examination and biochemical [liver function and alpha-fetoprotein (AFP)] analysis were also conducted at the follow-up visit.
The ablation was considered effective when the index tumor was treated according to the protocol and completely covered by the ablative zone without contrast enhancement at the immediate follow-up within 24 hours after RFA. Technique efficacy was confirmed in all of our recruited patients. IDR was defined as a new tumor with typical enhancement characteristics for HCC within different liver sub-segments from the original ablative zone. As the distinction between residual and recurrent disease is controversial, it may be impossible to differentiate microscopic remaining viable tumor from a new tumor focus at the ablative margin, the term local tumor progression (LTP) was used.[14]LTP was defined as the interval development of the tumor in continuity with the border of the ablative zone after RFA, where the RFA had been considered to be technically effective. If recurrence was observed during subsequent follow-up visits, additional treatment was performed.
Assessment of pre- and post-RFA imaging
All images were evaluated using a picture archiving and communication system (PACS; Pathspeed, GE Medical Systems Integrated Imaging Solutions, Prospect, IL, USA). MR findings were analyzed by two abdominal radiologists independently in a blinded manner. When discrepancies occurred, consensus was achieved during anadditional reading session. The reviewers were aware that the patients had RFA for HCC, but they were unaware of other information about the patients' histories and laboratory data. The MR images of HCC were randomly presented to avoid bias by creating a clinical practice setting. In the patients with multiple HCC lesions, the largest lesion was selected for assessment.
Regarding the measurement of the apparent diffusion coefficient (ADC), region of interest (ROI) was manually drawn on the diffusion-weighted images, including the whole ablation zone; these ROIs were then copied onto the ADC maps, and the ADC values were assessed.
Risk factors for IDR
The following host, tumoral and therapeutic variables were analyzed as potential risk factors for IDR: gender, age, whether RFA was the initial treatment, presence or absence of liver cirrhosis and portal hypertension, Child-Pugh classification, previous history of anti-virus therapy, alcohol abuse, smoking habits, hypertension, diabetes mellitus, levels of pretreatment laboratory markers (HBV-DNA, AFP, albumin, total bilirubin, alanine aminotransferase, aspartate aminotransferase, lactate dehydrogenase, alkaline phosphatase, γ-glutamyl transpeptidase, red blood cells, white blood cells, platelet count, and prothrombin time), tumor number, size (maximum diameter), shape (round/lobular), contact of tumor to liver capsule or major hepatic vessels, presence of pre-RFA biopsy or combined percutaneous ethanol injection therapy, ablative margin (the minimum margin, sufficient at 3 mm) and diminution of ablative region (a comparison of the maximum diameter of the ablative region within 24 hours and at one month after RFA). The ablative margin was defined as ablated normal parenchyma surrounding the tumor, lying beyond the previously estimated tumor borders. Visibility of the ablation margin was assessed on unenhanced T1, T2-weighted images, and enhanced T1-weighted images within 24 hours after RFA. The MR sequence that best showed the ablation margin was used for margin measurements, and the thinnest margin at any point along the circumference was reported as the minimum margin.[15]Furthermore, MR features were also analyzed, including the degree of arterial tumor enhancement (strong/poor) and existence of an enhanced tumor capsule before RFA; signal of the central ablative zone on T1-weighted images (T1WI; hyper or iso-hypointense compared with liver parenchyma), signal on T2-weighted images (T2WI; hyper or iso-hypointense) and degree of benign periablational enhancement (continuous or non-/disrupted enhancement) within 24 hours and at one month after RFA, and signal in DWI within 24 hours (hyper-/iso-/hypointense) and at one month (hyper-/iso-/hypo-/peripherally hyperintense) after RFA. We categorized the degree of arterial tumor enhancement into strong if it was greater than the surrounding liver parenchyma, and poor if it was not.Statistical analysis
The survival and cumulative IDR rates were analyzed using the Kaplan-Meier method. The variables that were considered as risk factors for IDR were analyzed using the log-rank test. A multivariate analysis of independent risk factors was conducted with a stepwise Cox-proportional hazards regression model. Additionally, receiver operating characteristic (ROC) analysis and corresponding area under the curve (AUC) statistics were used to determine the discriminatory accuracy of ADC values regarding IDR prediction. Statistical analyses were done using the SPSS software package (version 19.0, Chicago, IL, USA). All tests were two-sided andP<0.05 was considered statistically significant.
Results
Intrahepatic distant recurrence (IDR)
The patients had neither procedure-related mortality nor major complications that required treatments. The median follow-up period was 25 months (range 4-45 months). One patient died of the tumor before the development of IDR at 25 months after RFA.
IDR was identified in 20 patients (57.1%) during the follow-up period; these patients were identified in 4-44 months after RFA, with a median of 18 months [95% confidence interval (95% CI), 13-23 months]. The 12- and 24-month cumulative IDR-free survival rates were 76.7% (95% CI, 58.7%-87.6%) and 61.3% (95% CI, 42.8%-75.5%), respectively (Fig. 2). Of the 20 patients with IDR, 9 were treated with repeated RFA, 7 with TACE and, 4 with palliative methods including chemotherapy (2), radiotherapy (1) and traditional Chinese medicine (1). LTP was observed in 4 tumors, including one prior to IDR and two that coincided with IDR; complete local control with subsequent RFA treatment was obtained in these patients.
Risk factors for IDR
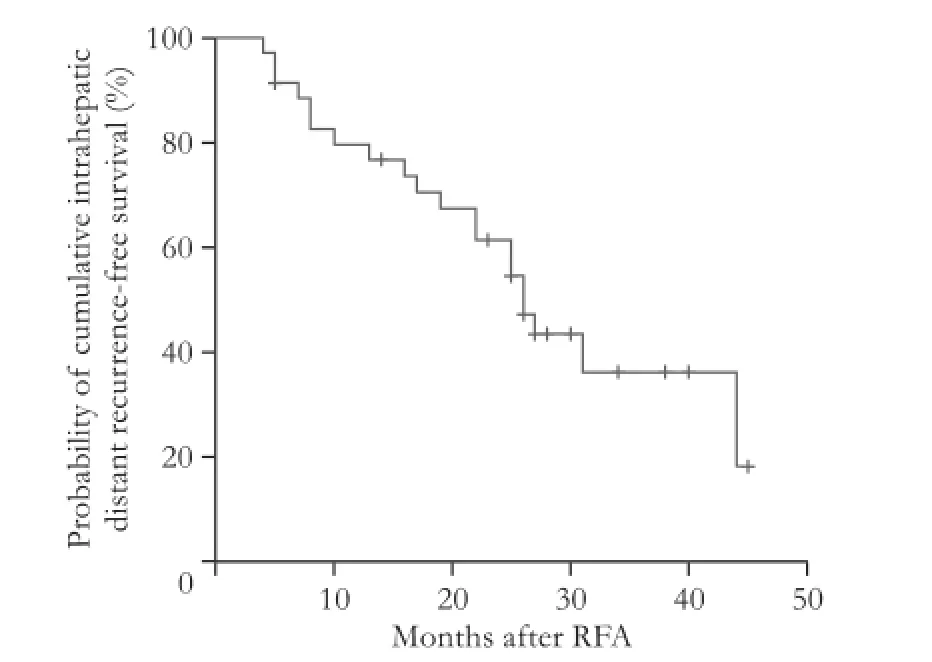
Fig. 2. Kaplan-Meier survival curve for intrahepatic distant recurrence (n=35) following percutaneous radiofrequency ablation of hepatocellular carcinoma. Cross marks (+) in the curve represent censored data.
Table 2 summarizes the risk factors for IDR determined according to the Kaplan-Meier method and logrank test. Pretreatment albumin level <3.5 g/dL (P=0.026), multinodular tumor (P=0.032), ablative margin <3 mm (P=0.007), no or disrupted periablational enhancement within 24 hours (P=0.001) and at one month (P=0.043) after RFA, and hyperintensity in the central ablative zone on T1WI at one month after RFA (P=0.004) were significantly related to IDR. A multivariate analysis using a stepwise Cox hazard model revealed that pretreatment albumin level <3.5 g/dL [hazard ratio (HR)=14.19; 95% CI, 1.252-160.779;P=0.032], multinodular tumor (HR=0.03; 95% CI, 0.002-0.457;P=0.012), no or disrupted periablational enhancement within 24 hours of RFA (HR=0.024; 95% CI, 0.002-0.237;P=0.001) and hyperintensity in the central ablative zone on T1WI at one month after RFA (HR=64.88; 95% CI, 4.327-972.774;P=0.003) were independent risk factors for IDR (Table 3). No significant differences were observed in the IDR rate between the patients with elevated and normal AFP levels (P=0.568).
The IDR rate was higher in patients with decreased albumin levels (<3.5 g/dL) than that in those with normal albumin levels (P=0.026). The 12- and 24-month IDR-free survival rates estimated by the Kaplan-Meier method after RFA were 62.5% (95% CI, 22.9%-86.1%) and 25.0% (95% CI, 3.7%-55.8%) respectively for patients with decreased albumin levels and 81.0% (95% CI, 60.2%-91.6%) and 68.9% (95% CI, 47.2%-83.1%) respectively for those with normal albumin levels (Fig. 3A).
Multinodular HCC was associated with a higher IDR rate (P=0.032). The 12- and 24-month IDR-free survival rates after RFA were 40.0% (95% CI, 5.2%-75.3%) and 20.0% (95% CI, 0.8%-85.2%) respectively for multinodular HCC and 82.9% (95% CI, 63.6%-92.5%) and 68.5% (95% CI, 48.1%-82.2%) respectively for uninodular HCC (Fig. 3B).
During the immediate follow-up within 24 hours after RFA, the lesions demonstrated marked hyperintensity with a surrounding hypointense band, including 17 (48.6%) lesions that displayed an iso-hypointense central zone on non-enhanced T1WI; at the one-month follow-up, most lesions (32, 91.4%) demonstrated a tar-get appearance with an enlarged iso-hypointense central zone, but the size of the entire ablative zone decreased by 17.9% on average, which was consistent with the result described in previous studies.[16]In patients with an iso-hypointense central zone at one month (Fig. 4A and B), the cumulative IDR-free survival rate was 80.7% (95% CI, 62.0%-90.9%) at 12 months and 63.9% (95% CI, 44.3%-78.2%) at 24 months, whereas the cumulative IDR-free survival rate was 33.3% (95% CI, 0.9%-77.4%) at 12 months and approached 0 at 24 months in patients with a persistent hyperintense central zone (P=0.004; Figs. 3C and 4C). On the T2WI, the tumors were typically iso-hypointense with a surrounding hyperintense band within 24 hours of RFA (33, 94.3%); after one month, 8 (22.9%) lesions exhibited relative hyperintensity. In the contrast-enhanced images, the ablative area did not exhibit enhancement, and the periablative area displayed continuous or discontinuous rim enhancement in most patients during the one-month follow-up. The cumulative IDR-free survival rate for patients with continuous benign periablational enhancement within 24 hours of RFA (Fig. 5A) was 85.9% (95% CI, 66.7%-94.5%) at 12 months and 71.0% (95% CI, 50.2%-84.3%) at 24 months. This rate decreased to 40.0% (95% CI, 5.2%-75.3%) at 12 months and approached 0 at 24 months in patients with no or disrupted periablational enhancement (P=0.001; Figs. 3D and 5B).
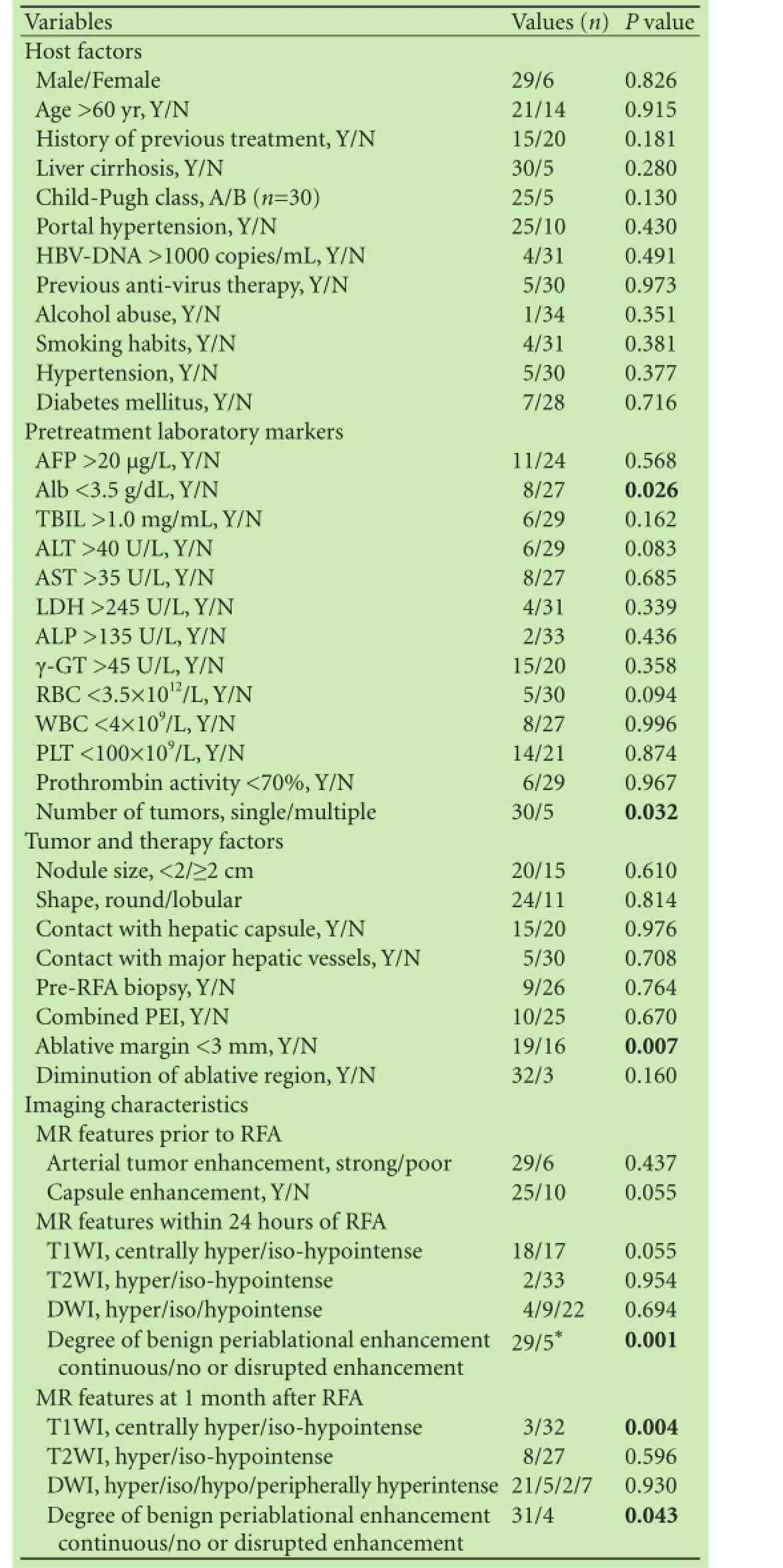
Table 2. Univariate analysis showing risk factors related to HCCIDR (n=35)

Table 3. Multivariate analysis showing independent risk factors related to HCC-IDR
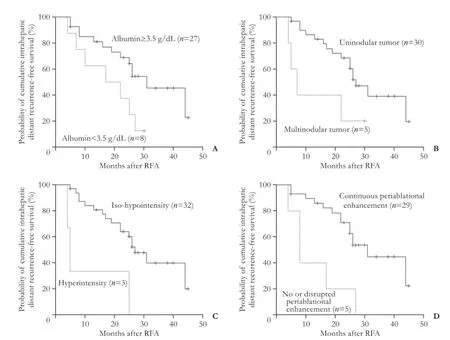
Fig. 3. Independent risk factors for intrahepatic distant recurrence following percutaneous radiofrequency ablation (RFA) of hepatocellular carcinoma. (A) pretreatment albumin <3.5 g/dL (P=0.026), (B) multinodular tumor (P=0.032), (C) hyperintensity of the central ablative zone on T1WI at 1 month after RFA (P=0.004), and (D) no or disrupted periablational enhancement within 24 hours of RFA (P=0.001) were significant factors identified by the Kaplan-Meier method and log-rank test. Cross marks (+) in the curve represent censored data.
In DWI, most ablated lesions were hypo- (22, 62.9%)or isointense (9, 25.7%) with a surrounding hyperintense band within 24 hours of RFA (P=0.694); after one month, a large proportion of tumors became globally (21, 60.0%) or peripherally (7, 20.0%) hyperintense (P=0.930). The ADC values exhibited an up-and-down evolution as a whole within the one-month follow-up, but the efficacy in predicting IDR outcome based on the ADC values (expressed as the area under the ROC curve) was 0.627, 0.572, and 0.530 before RFA, within 24 hours and at one month after RFA, respectively, which were not significant (P=0.224, 0.519, and 0.771, respectively) (Table 4).

Table 4. Thresholds of the ADC values according to the ROC curves and their efficacies
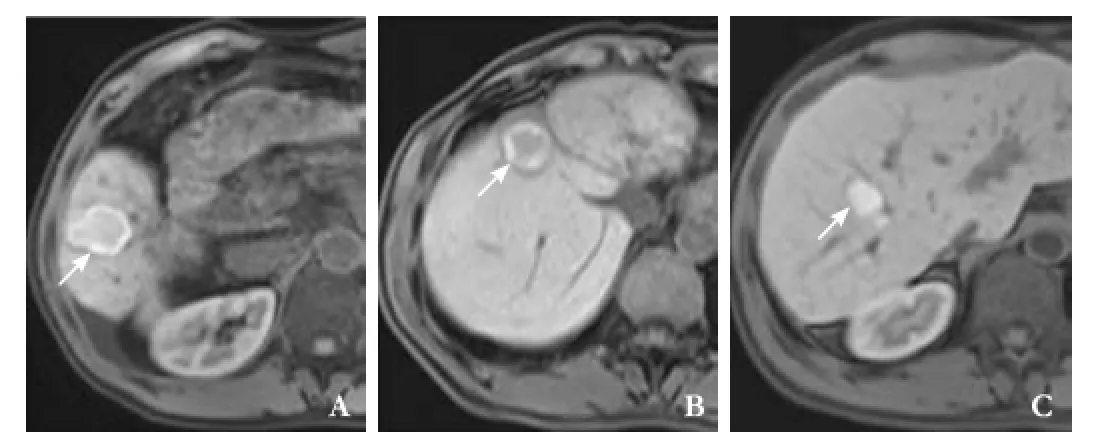
Fig. 4. Tumors with (A) isointensity (66-year-old man), (B) hypointensity (65-year-old man) and (C) hyperintensity (45-year-old man) in the central ablative zone on non-enhanced T1-weighted images at 1 month after percutaneous radiofrequency ablation.
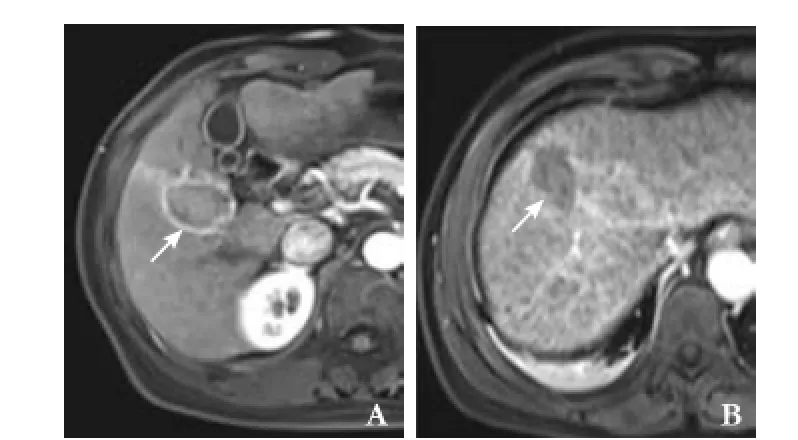
Fig. 5. Tumors with (A) continuous (a 51-year-old woman) and (B) disrupted periablational enhancement (a 55-year-old man) within 24 hours of percutaneous radiofrequency ablation.
Discussion
RFA has been increasingly and widely used. The heat RFA produced leads to irreversible cellular changes, which cause coagulative necrosis and consequently, cell death.[17]However, as demonstrated by many studies, RFA is associated with a high IDR rate (57.1% in this study), which negatively affects the long-term prognosis.[5-7]Therefore, analyzing the potential risk factors for IDR is especially important. Several studies[4,11,12,18-22]have reported the incidence and risk factors of IDR after RFA for HCC (Table 5), but most of them focused on clinical characteristics. Hence we investigated both clinical and imaging factors.
Two mechanisms of IDR have been assumed: intrahepatic dissemination and metachronous multicentric carcinogenesis.[11,23]A study[24]demonstrated that the state of the underlying liver is associated with IDR based on multicentric carcinogenesis. Our results supported this view and suggested that pretreatment albumin level <3.5 g/dL was an independent risk factor for IDR. Because impaired liver function may simultaneously increase the treatment risk,[6]special caution should be taken to select appropriate candidates for RFA. However, no significant correlation was observed between the AFP level and the occurrence of IDR. In contrast with several previous reports,[4,11,18,21,22]this discrepancy may be related to the relatively low positive AFP (>20 μg/L) rate (31.4%) in our cohort.
Chandarana et al[25]reported that tumor multifocality on MRI was significantly correlated with microvascular invasion, which may be closely related to intrahepatic dissemination. In our study, we found that multiplicity was an independent risk factor for IDR. This finding was also noted in previous studies.[12,18,19]
To date, the potential correlations between relevant imaging, especially MR features and IDR, have not been fully explored. In a recent study, Maruyama et al[12]examined pretreatment imaging findings using contrastenhanced ultrasound and found that patients with gradually enhanced tumors in the early arterial time were at higher risk for IDR. During the short-term follow-up after RFA, most lesions demonstrated peripheral rim enhancement surrounding the ablative zone. This finding is regarded as a reflection of reactive hyperemia due to an inflammatory reaction and granulation tissue formation and can last up to 6 months.[26,27]This benign periablational enhancement should be discriminated from residual tumor enhancement. The former is usually thin anduniform in thickness and envelops ablated lesions, which always present as hyperintense or isotense areas during the portal venous or delayed phase; whereas the latter shows nodular and irregular peripheral enhancement, which often presents as areas of hypointensity during the portal venous or delayed phase.[28,29]Some studies[4,20]investigated the relationship between the degree of benign periablational hyperemia and LTP, but no significant differences were observed. Our results indicated that patients with continuous periablational enhancement at 24-hour and one-month follow-ups after RFA had a lower IDR rate compared with those with no or disrupted rim enhancement. Thus, we speculated that continuous rim enhancement might indicate more thorough coagulation necrosis and less possibility of incomplete ablation with residual tumor cells in the marginal areas.
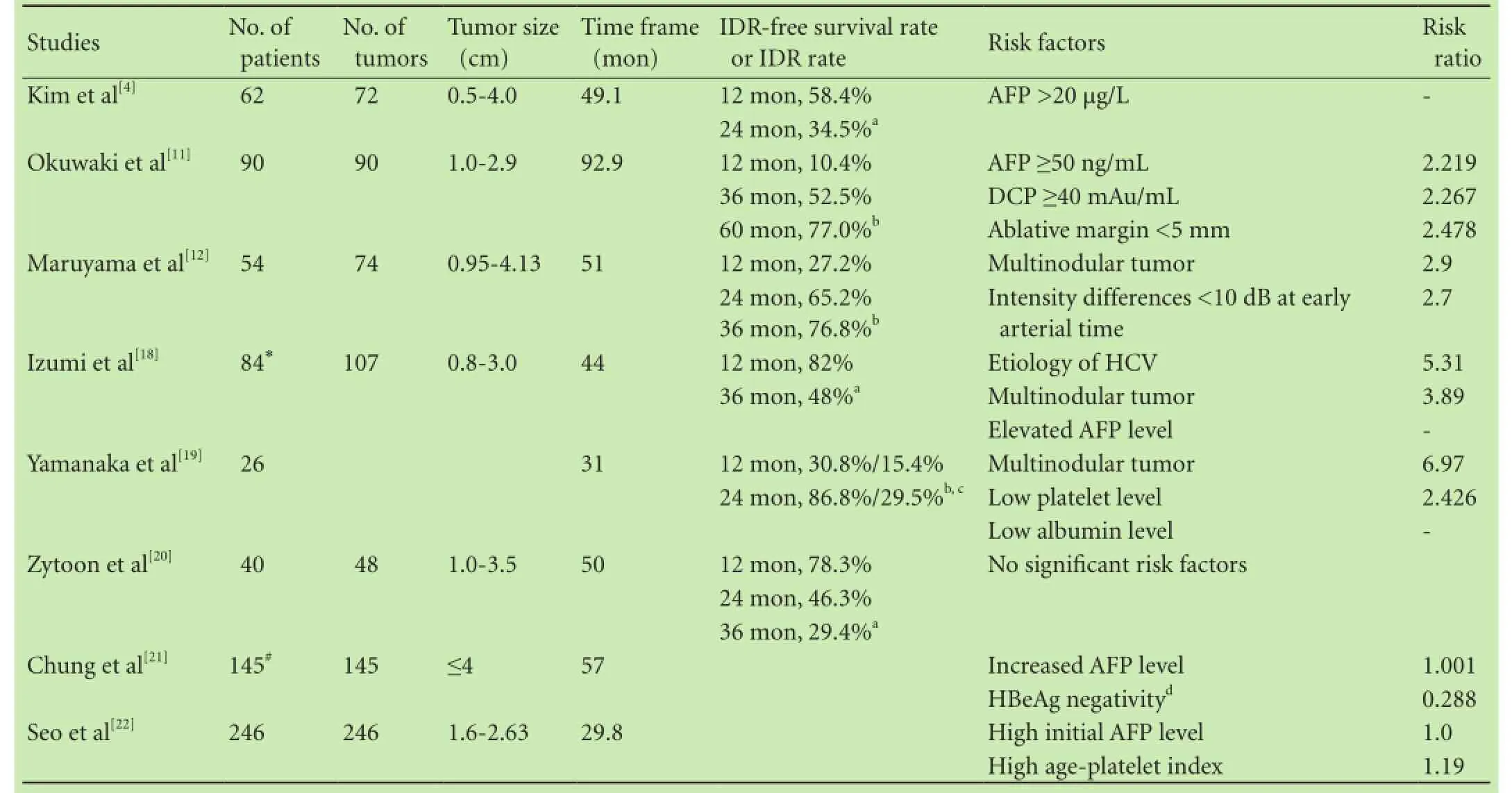
Table 5. Literature review of the risk factors for IDR in HCC after RFA
Lesions demonstrated marked hyperintensity on T1WI after ablation, and a target appearance of the ablative zone was commonly present within one month, which represents a central zone with iso-hypointensity, a broad hyperintense middle zone, and a surrounding hypointense band related to reactive hyperemia.[30,31]Studies[8,30,31]have demonstrated that the signal intensity changes on T1WI may be caused by the heterogeneity of tumor composition, the uneven evolution of coagulation necrosis, and the host response to thermal injury over time. At the short-term follow-up, the low signal intensity implies free water in enlarged sinusoids or tissue defect due to electrode needle, and the high intensity may be related to degenerated hepatocytes and red blood cells caused by hydration effect. With the extension of time, coagulated region degrades progressively, and the ablative areas may be gradually replaced by fibrous tissues with iso-hypointensity. In the current study, we demonstrated that a hyperintense central ablative zone on T1WI at one month after RFA was closely related to IDR; one potential explanation is that the persistent hyperintensity may be associated with a slower degraded evolution. Further studies, especially a radiologic-histologic comparative analysis, are needed to validate our data and achieve more convincing conclusions.
A gross tumor-free margin of one cm in all directions around the tumor in the resected specimen is generally accepted by most surgeons and pathologists. Reports[27,32,33]have also recommended an ablative margin of 5-10 mm to achieve therapeutic results similar to those of surgery. Kim et al[34]and Shyn et al[35]found that a margin of 3 mm or more was associated with a lower LTP rate, similarly we found that an ablative margin less than 3 mm was at higher risk for IDR. The marginal area wasmost likely to contain viable tumor cells and small satellite nodules, and portal vein invasion was occasionally detected in even small HCC, which necessitated an ablative margin of at least 3 mm. As reported by Kim et al,[34]however, the 3-mm margin may be used as a criterion for more attention and closer follow-up rather than a goal of ablation, because a larger ablative margin is more beneficial and related to a lower recurrence rate. Moreover, a follow-up immediately after RFA (within 24 hours) is necessary to guarantee adequate ablation and exclude the possibility of residual viable tissues by using imaging criteria beforehand.
DWI and ADC maps provide insights into the molecular water composition and the degree of tumor viability at the cellular level. Cellular necrosis causes increased membranous permeability, which enables free diffusion of water molecules and an increased ADC value.[36,37]Lu et al[37]noted that the ADC of completely ablated HCCs increased at one month, decreased at 3 months, and increased again at 6 months without clear evolutional patterns. In our study, however, the ADC of the whole lesion demonstrated an up-and-down trend within the onemonth follow-up. The decreased ADC may be related to some type of restrictive effect due to tissue dehydration, which results from cellular necrosis or cellular swelling. Schraml et al[38]reported a higher LTP rate in patients with lower ADC values in the peripheral ablative region. We also analyzed the value of ADC in the prediction of IDR after RFA, but no significant predictive value was identified. Our results may be limited by the relatively small sample size, thus, further large scale investigations are needed.
The major limitations of our study are the relatively small study population and the retrospective nature. Firstly, the utility of the clinical or imaging characteristics as prognostic factors in practice should be evaluated in well-designed prospective studies on a large cohort of patients. Secondly, only a small portion of tumors were pathologically confirmed; thus, the radiologic-histologic correlation and the relationship between IDR and histopathological features were not examined. Thirdly, our analysis of IDR was independent of local tumor recurrence. In our study there were 3 patients with local recurrence occurred prior to or simultaneously with IDR and the local recurrence may affect the subsequent IDR. Fourthly, we didn't differentiate IDR caused by intrahepatic metastasis or multicentric carcinogenesis. Finally, the patients were treated with two different types of RF devices which might bring in some variations.
In conclusion, patients with hepatitis B-related small HCC with low serum albumin, multiple nodules, and lesions with no or disrupted periablational enhancement and persistent hyperintensity in the central ablative zone on T1WI within the one-month follow-up after RFA are at higher risk for IDR, and a close follow-up is recommended, even if RFA is complete. A sufficient ablative margin of at least 3 mm is required. Thus, we propose that noninvasive clinical and imaging measures should be used to provide early warning of IDR, and further studies are needed to confirm our data and establish a strategy to prevent IDR after RFA.
Contributors:ZMS proposed the study. SRF, ZMS and CCZ performed research and wrote the first draft. SRF, RZG, YSL and ZL collected and analyzed the data. All authors contributed to the design and interpretation of the study and to further drafts. ZMS is the guarantor.
Funding:None.
Ethical approval:This study was approved by the institutional review board (B2014-002).
Competing interest:The authors do not choose to declare any conflict of interest related directly or indirectly to the subject of this article.
1 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011;61:69-90.
2 Sherman M. Hepatocellular carcinoma: epidemiology, surveillance, and diagnosis. Semin Liver Dis 2010;30:3-16.
3 El-Serag HB. Hepatocellular carcinoma. N Engl J Med 2011;365: 1118-1127.
4 Kim YS, Rhim H, Cho OK, Koh BH, Kim Y. Intrahepatic recurrence after percutaneous radiofrequency ablation of hepatocellular carcinoma: analysis of the pattern and risk factors. Eur J Radiol 2006;59:432-441.
5 Tiong L, Maddern GJ. Systematic review and meta-analysis of survival and disease recurrence after radiofrequency ablation for hepatocellular carcinoma. Br J Surg 2011;98:1210-1224.
6 Brunello F, Cantamessa A, Gaia S, Carucci P, Rolle E, Castiglione A, et al. Radiofrequency ablation: technical and clinical long-term outcomes for single hepatocellular carcinoma up to 30 mm. Eur J Gastroenterol Hepatol 2013;25:842-849.
7 Pompili M, Saviano A, de Matthaeis N, Cucchetti A, Ardito F, Federico B, et al. Long-term effectiveness of resection and radiofrequency ablation for single hepatocellular carcinoma ≤3 cm. Results of a multicenter Italian survey. J Hepatol 2013;59:89-97.
8 Goldberg SN, Gazelle GS, Compton CC, Mueller PR, Tanabe KK. Treatment of intrahepatic malignancy with radiofrequency ablation: radiologic-pathologic correlation. Cancer 2000;88: 2452-2463.
9 Li WH, Ma KW, Cheng M, Chui KH, Chan PT, Chu WH, et al. Radiofrequency ablation for hepatocellular carcinoma: a survival analysis of 117 patients. ANZ J Surg 2010;80:714-721.
10 Forner A, Reig ME, de Lope CR, Bruix J. Current strategy for staging and treatment: the BCLC update and future prospects. Semin Liver Dis 2010;30:61-74.
11 Okuwaki Y, Nakazawa T, Shibuya A, Ono K, Hidaka H, Watanabe M, et al. Intrahepatic distant recurrence after radiofrequency ablation for a single small hepatocellular carcinoma:risk factors and patterns. J Gastroenterol 2008;43:71-78.
12 Maruyama H, Takahashi M, Shimada T, Sekimoto T, Kamesaki H, Kanai F, et al. Pretreatment microbubble-induced enhancement in hepatocellular carcinoma predicts intrahepatic distant recurrence after radiofrequency ablation. AJR Am J Roentgenol 2013;200:570-577.
13 Bruix J, Sherman M; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology 2011;53:1020-1022.
14 Ahmed M, Solbiati L, Brace CL, Breen DJ, Callstrom MR, Charboneau JW, et al. Image-guided tumor ablation: standardization of terminology and reporting criteria--a 10-year update. Radiology 2014;273:241-260.
15 Wang X, Sofocleous CT, Erinjeri JP, Petre EN, Gonen M, Do KG, et al. Margin size is an independent predictor of local tumor progression after ablation of colon cancer liver metastases. Cardiovasc Intervent Radiol 2013;36:166-175.
16 Kim YS, Rhim H, Lim HK, Choi D, Lee MW, Park MJ. Coagulation necrosis induced by radiofrequency ablation in the liver: histopathologic and radiologic review of usual to extremely rare changes. Radiographics 2011;31:377-390.
17 Lee CH, Braga L, de Campos RO, Semelka RC. Hepatic tumor response evaluation by MRI. NMR Biomed 2011;24:721-733.
18 Izumi N, Asahina Y, Noguchi O, Uchihara M, Kanazawa N, Itakura J, et al. Risk factors for distant recurrence of hepatocellular carcinoma in the liver after complete coagulation by microwave or radiofrequency ablation. Cancer 2001;91:949-956.
19 Yamanaka Y, Shiraki K, Miyashita K, Inoue T, Kawakita T, Yamaguchi Y, et al. Risk factors for the recurrence of hepatocellular carcinoma after radiofrequency ablation of hepatocellular carcinoma in patients with hepatitis C. World J Gastroenterol 2005;11:2174-2178.
20 Zytoon AA, Ishii H, Murakami K, El-Kholy MR, Furuse J, El-Dorry A, et al. Recurrence-free survival after radiofrequency ablation of hepatocellular carcinoma. A registry report of the impact of risk factors on outcome. Jpn J Clin Oncol 2007;37: 658-672.
21 Chung GE, Kim W, Lee JH, Kim YJ, Yoon JH, Lee JM, et al. Negative hepatitis B envelope antigen predicts intrahepatic recurrence in hepatitis B virus-related hepatocellular carcinoma after ablation therapy. J Gastroenterol Hepatol 2011;26:1638-1645.
22 Seo JY, Kim W, Kwon JH, Jin EH, Yu SJ, Kim HY, et al. Noninvasive fibrosis indices predict intrahepatic distant recurrence of hepatitis B-related hepatocellular carcinoma following radiofrequency ablation. Liver Int 2013;33:884-893.
23 Ng KK, Poon RT, Lo CM, Yuen J, Tso WK, Fan ST. Analysis of recurrence pattern and its influence on survival outcome after radiofrequency ablation of hepatocellular carcinoma. J Gastrointest Surg 2008;12:183-191.
24 Fuke H, Sugimoto K, Shiraki K, Tanaka J, Beppu T, Yoneda K, et al. Predictive factors for distant recurrence of HCV-related hepatocellular carcinoma after radiofrequency ablation combined with chemoembolization. Aliment Pharmacol Ther 2008;27:1253-1260.
25 Chandarana H, Robinson E, Hajdu CH, Drozhinin L, Babb JS, Taouli B. Microvascular invasion in hepatocellular carcinoma: is it predictable with pretransplant MRI? AJR Am J Roentgenol 2011;196:1083-1089.
26 Koda M, Tokunaga S, Miyoshi K, Kishina M, Fujise Y, Kato J, et al. Assessment of ablative margin by unenhanced magnetic resonance imaging after radiofrequency ablation for hepatocellular carcinoma. Eur J Radiol 2012;81:2730-2736.
27 Gervais DA, Kalva S, Thabet A. Percutaneous image-guided therapy of intra-abdominal malignancy: imaging evaluation of treatment response. Abdom Imaging 2009;34:593-609.
28 Watanabe H, Kanematsu M, Goshima S, Yoshida M, Kawada H, Kondo H, et al. Is gadoxetate disodium-enhanced MRI useful for detecting local recurrence of hepatocellular carcinoma after radiofrequency ablation therapy? AJR Am J Roentgenol 2012;198:589-595.
29 Liu CH, Arellano RS, Uppot RN, Samir AE, Gervais DA, Mueller PR. Radiofrequency ablation of hepatic tumours: effect of post-ablation margin on local tumour progression. Eur Radiol 2010;20:877-885.
30 Tsuda M, Rikimaru H, Majima K, Yamada T, Saito H, Ishibashi T, et al. Time-related changes of radiofrequency ablation lesion in the normal rabbit liver: findings of magnetic resonance imaging and histopathology. Invest Radiol 2003;38:525-531.
31 Khankan AA, Murakami T, Onishi H, Matsushita M, Iannaccone R, Aoki Y, et al. Hepatocellular carcinoma treated with radio frequency ablation: an early evaluation with magnetic resonance imaging. J Magn Reson Imaging 2008;27:546-551.
32 Woo S, Lee JM, Yoon JH, Joo I, Kim SH, Lee JY, et al. Smalland medium-sized hepatocellular carcinomas: monopolar radiofrequency ablation with a multiple-electrode switching system-mid-term results. Radiology 2013;268:589-600.
33 Nakazawa T, Kokubu S, Shibuya A, Ono K, Watanabe M, Hidaka H, et al. Radiofrequency ablation of hepatocellular carcinoma: correlation between local tumor progression after ablation and ablative margin. AJR Am J Roentgenol 2007;188:480-488.
34 Kim YS, Lee WJ, Rhim H, Lim HK, Choi D, Lee JY. The minimal ablative margin of radiofrequency ablation of hepatocellular carcinoma (> 2 and < 5 cm) needed to prevent local tumor progression: 3D quantitative assessment using CT image fusion. AJR Am J Roentgenol 2010;195:758-765.
35 Shyn PB, Mauri G, Alencar RO, Tatli S, Shah SH, Morrison PR, et al. Percutaneous imaging-guided cryoablation of liver tumors: predicting local progression on 24-hour MRI. AJR Am J Roentgenol 2014;203:W181-191.
36 Kamel IR, Liapi E, Reyes DK, Zahurak M, Bluemke DA, Geschwind JF. Unresectable hepatocellular carcinoma: serial early vascular and cellular changes after transarterial chemoembolization as detected with MR imaging. Radiology 2009;250:466-473.
37 Lu TL, Becce F, Bize P, Denys A, Meuli R, Schmidt S. Assessment of liver tumor response by high-field (3 T) MRI after radiofrequency ablation: short- and mid-term evolution of diffusion parameters within the ablation zone. Eur J Radiol 2012;81:e944-950.
38 Schraml C, Schwenzer NF, Clasen S, Rempp HJ, Martirosian P, Claussen CD, et al. Navigator respiratory-triggered diffusion-weighted imaging in the follow-up after hepatic radiofrequency ablation-initial results. J Magn Reson Imaging 2009;29:1308-1316.
Received September 12, 2014
Accepted after revision March 11, 2015
Author Affiliations:Department of Radiology, Zhongshan Hospital, Fudan University; Shanghai Institute of Medical Imaging; Department of Medical Imaging, Shanghai Medical College, Fudan University (Sheng RF, Zeng MS and Chen CZ); Liver Cancer Institute, Zhongshan Hospital, Fudan University; Key Laboratory of Carcinogenesis and Cancer Invasion, Ministry of Education (Ren ZG, Ye SL and Zhang L), Shanghai 200032, China
Meng-Su Zeng, MD, PhD, Department of Radiology, Zhongshan Hospital, Fudan University, No. 180 Fenglin Road, Xuhui District, Shanghai 200032, China (Tel: +86-21-64041990ext2130; Fax: +86-21-64439906; Email: zeng.mengsu@zs-hospital.sh.cn)
© 2015, Hepatobiliary Pancreat Dis Int. All rights reserved.
10.1016/S1499-3872(15)60390-3
Published online July 2, 2015.
杂志排行

Hepatobiliary & Pancreatic Diseases International的其它文章
- Gut microbiota and non-alcoholic fatty liver disease
- Risk factors of metabolic syndrome after liver transplantation
- Combined Hangzhou criteria with neutrophillymphocyte ratio is superior to other criteria in selecting liver transplantation candidates with HBV-related hepatocellular carcinoma
- Warm HTK donor pretreatment reduces liver injury during static cold storage in experimental rat liver transplantation
- Oncogenic role of microRNA-423-5p in hepatocellular carcinoma
- Ankaflavin ameliorates steatotic liver ischemiareperfusion injury in mice