Profile and geographical distribution of reported cutaneous leishmaniasis cases in Northwestern Saudi Arabia, from 2010 to 2013
2015-12-08NajouaHaouasOmarAmerAsmaIshankytyAdnanAlazmiIbrahimIshankyty
Najoua Haouas, Omar Amer, Asma Ishankyty, Adnan Alazmi, Ibrahim Ishankyty
1College of Applied Medical Sciences, Clinical Laboratory Sciences Department, University of Hail, KSA
2Laboratoire de Parasitologie-Mycologie Médicale et Moléculaire (code LR12ES08), Département de Biologie Clinique B, Faculté de Pharmacie, Université de Monastir, Tunisia
Profile and geographical distribution of reported cutaneous leishmaniasis cases in Northwestern Saudi Arabia, from 2010 to 2013
Najoua Haouas1,2*, Omar Amer1, Asma Ishankyty1, Adnan Alazmi1, Ibrahim Ishankyty1
1College of Applied Medical Sciences, Clinical Laboratory Sciences Department, University of Hail, KSA
2Laboratoire de Parasitologie-Mycologie Médicale et Moléculaire (code LR12ES08), Département de Biologie Clinique B, Faculté de Pharmacie, Université de Monastir, Tunisia
ARTICLE INFO
Article history:
Received 15 January 2015
Received in revised form 20 February 2015
Accepted 15 March 2015
Available online 20 April 2015
Cutaneous leishmaniais
Objective: To describe the profile and geographical distribution of reported cases of cutaneous leishmaniasis (CL) in the province of Hail, Saudi Arabia from 2010 to 2013. Methods: Human data were collected from the dermatology service of both King Khaled and General Hail hospitals. Results: A total of 483 confirmed CL cases were investigated. Cutaneous leishmaniasis follows a seasonal distribution related to the activity of the phlebotomine sand fly fauna. Both saudi and non saudi patients were almost equally infected. The number of reported cases of CL in men was higher than that in females. The frequency of CL was asoociated with age and increased in teenager and adult group. By analyzing the geographical distribution, the majority of Hail districts were affected with this disease. However it is more prevalent in Hail city. Conclusions: The lack of data concerning the parasite, the sand fly fauna and the existing transmission cycles in Hail province make difficult to interpret the reported results and to follow up the spatio-temporal evolution of the disease.
1. Introduction
Cutaneous leishmaniasis (CL) is a protozoan disease transmitted through the bites of infected phlebotomine sandflies and caused by members of Leishmania species. It is the most prevalent clinical form worldwide with an approximative global incidence of about 1.2 million cases per year. About one-third of these cases occurrs in each of three epidemiological regions, the Americas, the Mediterranean basin, and western Asia. Kingdom of Saudi Arabia (KSA) is classified as the fourth most endemic focus of CL in the middle East to Central Asia region with an estimated annual incidence ranging from 9 600 to 15.8 cases/year[1].
The first CL case in KSA was reported by Morsy and Shoura in 1973[2]. Since this date the disease has been reported in different parts of the country and many regions were endemic such as Al Qaseem, Al Madinah Al Munawarrah, Riyadh, Al Hassa and Aseer[3-7]. According to the Ministry Of Heath statistical reports, Hail province is reported as the fifth most infected region among other Saudi provinces and cities. Indeed, the average reported incidence of CL in Hail is 183 case/year[8]. Despite the endemicity of Hail province to CL, no published research is available until now describing the epidemiological profile of this disease and its geographical distribution.
Thereby, our present retrospective investigation aims to describe the epidemiology profile of CL in Hail province. Thus, in this first study, epidemiology of the disease is discussed in Hail over a fouryear period (2010-2013).
2. Material and methods
2.1. Study area
This is an epidemiological investigation of CL in the province of Hail. It is one of the 20 Saudi provinces. It is located in northwestern KSA. It has a continental desert climate with hot summers (average high temperature 29.2 ℃) and cool winters (average low temperature 13.3 ℃). Hail is located in a higher altitude with an annual precipitation of 100.6 mm. According to the Ministry of the Interior (2013), Hail has a population of 527 000 persons.
2.2. Study design and data collection
Human CL data collection was based on available records in the dermatology services of both King Khaled and General Hail hospitals over a period of four years, from 2010 to 2013.
First-line CL diagnosis was based on the clinical aspect of the lesion. Physician investigates the lesion appearance (mostly a nonhealing nodulo-ulcerative lesion with “volcanic crater”), its evolution period (slowly enlarging lesion) and the geographical origin of the patient. Diagnosis is confirmed by the microscopic demonstration of Leishmania amastigotes on Giemsa-stained scraping tissue smears.
Basic data including the age, the gender and the nationality (Saudi or Non Saudi) of the patient, the precise date of consultation and the patient's residence (at the level of the first administrative unit) were collected for all the patients. More detailed information regarding the number of sores and time between onset of the lesions and initial consultation were analyzed only for a subset of patients for whom those data were available.
3. Results
3.1. Number of cases
Four hundred eighty three patients, 70.6% male and 29.4% female, who attented King Khaled and General Hail hospitals of Hail province KSA between 2010 and 2013, were diagnosed with CL. The yearly number of reported CL cases ranged from 94 to 172, with a mean of reported cases per-year of about 121 patients. Nevertheless, this number was markedly decreased from 172 cases in 2010 to about 96 in 2011 and 2012 and a re-increasing to 119 cases in 2013.
3.2. Seasonality
The monthly distribution of cases referred to the date of medical consultation and CL diagnosis. Cases of CL were recorded in all months of the year with a minimum in june (13 cumulative cases) and a maximum in February (64 cases). The number of reported cases increased in August, remained high in the following months, and reached its peak in February and March. The main cluster was in the period from December to March of the next year (236 cases, 48.86%). Then, the number of patients began to decline in April and reached its lowest number between June and July (Figure 1).
Among the infected cases, 179 are Saudi and 104 are non Saudi. In each month of the year both Saudi and non Saudi CL cases were reported.
By supperposing the reported number of CL cases and the mean rainful precipitation per month of the same period (2010-2013), we noted that human leishmaniasis cases appeared one to three months after a peak of precipitation (Figure 1).
3.3. Age distribution
The age of patients ranged from less than one year to more than 45 years. The majority (68.32%) of cases occurred in the teenager and adult group aged from 15 to more than 45 years. Number of cutaneous leishmaniasis cases markedly decline for the other groups of age. The lowest rate was found in patients less than one year (4.55%). 9.93% were in 1-4 yrs, 7.86% in 5-9 yrs and 9.31% in 10-14 yrs age groups, respectively. Till fourteen years both genders were almost equally infected. However, for the teenager and adults group, males were more infected than females (Figure 2). 70.6% were males and 29.4% were females.
By comparison of the infection rate between Saudi and non Saudi patient we have noticed differences inside the age groups. Indeed, at the children group (from 0 to 14 years) 94.8% of the infected cases were Saudi and only 5.2% were non Saudi. However, in the teenager and adult group (more the 15 years) the infection rates in the two nationalities are mostly equal. In fact, 44.8% were Saudi and 55.2% were non Saudi (Figure 3).
3.4. Residence and geographical distribution of cases
All districts of Hail province were involved, with large variation in the distribution of cases. According to the type of residence in which the cases lived, 74.3% (n=359 cases) of them lived in urbanized areas in Hail city. Whereas 25.7% (n=124 cases) were from rural settlements, mainly form Shenan (19.4%; n=24 cases), Jubbah (18.5%; n=23 cases) and Baqaa village (8%, n=10 cases) (Table 1, Figure 4). For the other villages, only few sporadic cases were reported. A map showing the distribution of cumulative CL cases by districts, number of cases and nationality proportions is shown in Figure 5.

Table 1 Distribution of the reported CL cases between 2010 and 2013 according to the geographical origin and the nationality.
Among the 359 CL cases of Hail city, 23.7% were from Al Azizya neighborhood followed by El Khuzama with 11.7%, Eastern Park with 11.4%, Ennagra with 7% and Eljamiin, El Matar and Al Wassita neighborhoods with 6.4% for each. The other neighborhoods present together approximately 27% of the reported CL cases in Hail city. Figure 5 summarize the distribution of CL cases in the neighborhoods of Hail city according to the number of cumulative cases and the nationality proportion.
3.5. Clinical features
Clinical data including number of lesion and duration prior diagnosis were available for only 146 CL cases. Among this group, 61 patients (41.8%) present a single lesion, 25 patients (17.1%)
with two lesions and 60 patients (41.1%) have between 3 to 13. By analyzing the number of lesion in each age group, no significant difference was noted.
Of the 146 patients for whom an accurate time of onset of lesion was recorded, 117 (80.13%) presented one to two months after the onset of their skin lesions (Table 2).
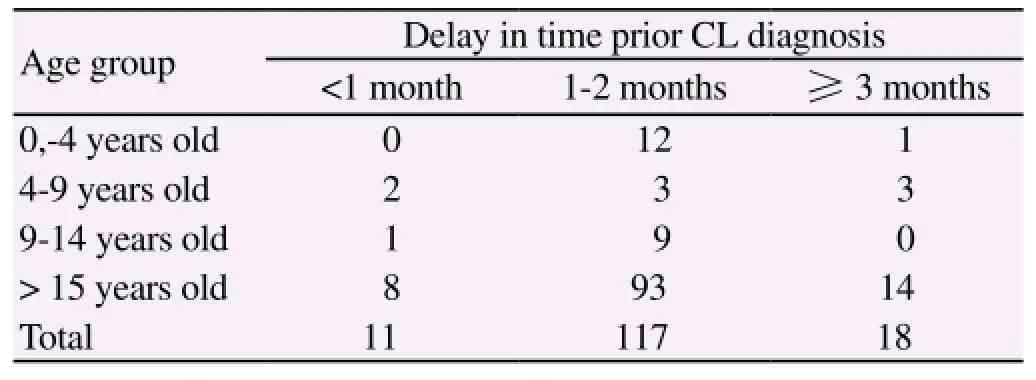
Table 2 Duration of skin lesion prior diagnosis
4. Discussion
Cutaneous leishmaniasis has been reported in the Arabian Peninsula since 1973[9]. A large set of date is available concerning the epidemiological feature of this disease in some foci of the country such as Al Madinah Al Munawarah, Al Baha, Al Hassa and Al Qassim provinces. These data concern the identification of the causative Leishmania species, the clinical feature as well as the analysis of the phlebotomine sand flies fauna in these regions[4,5,7,10-12]. Despite all these studies, some Saudi foci are still not investigated and no reports about the epidemiological feature of CL are available until now. Among these foci is the Hail Province in Northwestern Saudi Arabia.
To the best of our knowledge, this is the first reported epidemiological study of CL in Hail province KSA. This four years retrospective study allows us to get epidemiological data from 483 patients with confirmed CL. A definite fluctuation of the mean number of case per month is evident in our study. Indeed, the number of cases is high between September and March of the next year. Its high level is reported between January and March of each year. The lowest number is noticed in summer between June and July. The most likely factor that could explain this variation is the fluctuation of the sand flies population (Vector of the disease) during the year. Indeed, during a study of the sand fly population in Al-Baha Province, the analysis of Phlebotomus papatasi population (Vector of Zoonotic CL) has demonstrated the presence of two pullulation peaks: one in May-June and another in august[11]. Accordingly, clinical cutaneous lesions appear after three to four months post the infected bite.
Also, we must emphasize that the lag time from the development of skin lesions to the visit of patients to physicians results in a difference in timing between the peak activity of the sand fly and the peak of human CL cases[13].
The analysis of the CL distribution among the age group has demonstrated that all group of age are susceptible to infection with Leishmania. Nevertheless, the disease is most prevalent in the teenager and adult group. This finding could be explained by the difference in the activity rate between the different ages. Indeed, Teenager and adult must be more active in sundown and the night (activity time of the female sand fly) and accordingly the risk to be bite by the sand fly is bigger by comparison to the other ages. Our finding is different to those of Al-Tawfiq and Abukhamsin (2004) who noted that age between one and four years are affected more frequently than other age groups[3]. Though, our results agree with those of Al-Taqi and Behbehani (1980) who reported that CL occurs in patients between the ages of 21 and 30 years more often than in other ages[14].
Moreover, by comparison of CL in both genders we have noticed that teenager and adult men are significantly more infected than women. This result could be explained by the difference in the sartorial habits between the two genders. Indeed, the total veiling of teenager and adult women in Hail province results in a decrease of the risk of sand fly biting and therefore a decrease of the CL prevalence in this gender. Nevertheless, for patients aged less than 15 years, both genders are equally infected. This last finding was already reported by Al-Tawfiq and Abukhamsin and Al-Gindan et al[3,13].
Concerning the nationality of the patients, both Saudi and non-Saudi are affected with CL equally. This is an expected result since sand fly has no preference for the human blood meals. However, it is important to highlight that 95.8% of the non Saudi patients are teenagers and adults (more than 15 years old). This must be the direct consequence of the composition of this population since foreign workers are mainly composed by adults.
Geographical distribution of CL cases in Hail province has shown that the biggest number is located in center of Hail and only few cases were reported in the other villages. This result could not reflect the endemicity level of CL among Hail villages. Indeed, a number of issues might have affected this finding. First, during this retrospective study data were recorded from two public hospitals in Hail. These are never the only sources of information about CL and the number of reported cases reflects only patients visiting these two public clinics. Second, the existance of limited care centers and limited awareness in rural areas may have contributed to the possibly false impression that the disease burden in some villages is low. The consequence of this is the potential under-estimation of the disease. According to Jaber et al, 2013, the enhancing of a national reporting system through the incorporation of data that are geocoded based on
patients addresses and using Geographic Information Systems-based multiuser geodatabases could be the appropriate way to overcome this under-estimation limit[6].
Among Hail city neighborhoods, Al Azizya city was the most endemic region with the biggest number of CL cases. This result must be the consequence of the existence of a stable transmission cycle including the parasite species, the sand fly vector and the reservoir host.
Unfortunately, the lack of data concerning all these transmission cycle actors in this focus make difficult to explain the observed discrepancy concerning the geographical distribution of the disease. Cutaneous leishmaniasis in Hail province is prevalent. It affects mainly teenagers and adults male. This disease has a seasonal pattern which correlates with the activity of the vector. Geographical distribution indicates that Hail city is endemic for the disease. More investigations concerning the identification of the causative species of Leishmania and the analysis of the phlebotomine sand fly fauna are crucial to follow up the spatio-temporal evolution of the disease and to establish an effective control strategy.
Conflict of interest statement
We declare that we have no conflict of interest.
[1] Alvar J, Vélez ID, Bern C, Herrero M, Desjeux P, Cano J, et al. Leishmaniasis worldwide and global estimates of its incidence. Plos One 2012; 7(5): 1-12.
[2] Morsy TA, Shoura MI. Some aspects of cutaneous leishmaniasis. Int Cong Trop Med Malar 1973; 1: 138.
[3] Al-Tawfiq JA, Abukhamsin A. Cutaneous leishmaniasis: a 46-year study of the epidemiology and clinical feature in Saudi Arabia (1956-2002). Int J Infect Dis 2004; 8: 244-250.
[4] El-Beshbishy HA, Al-li KH, El-Badry AA. Molecular characterization of cutaneous leishmaniasis in Al-Madinah Al-Munawarah province, western Saudi Arabia. Int J Infect Dis 2013a; 17(5): e334-e338.
[5] El-Beshbishy HA, Al-Ali KH, El-Badry AA. Molecular characterization of Leishmania infection in sand flies from Al-madinah. Al-munawarah province, western Saudi Arabia. Exp Parasitol 2013b; 134(2): 211-215.
[6] Jaber SM, Ibbini JH, Hijjawi NS, Amdar NM, Huwail MJ, Al-Aboud K. Exploring recent spatial patterns of cutaneous leishmaniasis and their associations with climate in some countries of the Middle East using geographical information systems. Geospatial Health 2013; 8(1): 143-158.
[7] Shalaby I, Gherbawy Y, Jamjoom M, Banaja AE. Genotypic characterization of cutaneous leishmaniasis at Al Baha and Al Qasim Provinces (Saudi Arabia). Vector Borne Zoonotic Dis 2011; 11(7): 807-813.
[8] MOHSA, 2006-2012. Statistical books for the years 2006-2012. Ministry of Health of Saudi Arabia. [Online] Available from: http://www.moh.gov. sa/en/Ministry/Statistics/book/Pages/defa ult.aspx [Accessed on March 2014].
[9] Aramco Medical Department. Epidemiological bulletin. 1-4 Jun-Jul, 1976.
[10] Al-Mohammed HI. Efficacy of two rodenticides against Leishmania reservoir host rat (Psammomys obesus) in the rural area of Al-Ahsa Oasis, Saudi Arabia. J Egypt Soc Parasitol 2010; 40(3): 609-616.
[11] Doha SA, Samy AM. Bionomics of phlebotomine sand flies (Diptera: Psychodidae) in the province of Al-Baha, Saudi Arabia. Mem Inst Oswaldo Cruz 2010; 105(7): 850-856.
[12] El-Badry A, Al-Juhani A, Ibrahim el-K, Al-Zubiany S. Distribution of sand flies in El-Nekheil province, in Al-Madinah Al-Munawwarah region, western of Saudi Arabia. Parasitol Res 2008; 103(1): 151-156.
[13] Al-Gindan Y, Abdul-Aziz O, Kubba R. Cutaneous leishmaniasis in Al-Hassa, Saudi Arabia. Int J Dermatol 1984; 23: 194-197.
[14] Al-Taqi M., Behbehani K. Cutaneous leishmaniasis in Kuwait. Ann Trop Med Parasitol 1980; 74: 495-501.
ment heading
10.1016/S1995-7645(14)60332-1
*Corresponding author: Najoua Haouas, College of Applied Medical Sciences, Clinical Laboratory Sciences Department, University of Hail, Kingdom of Saudi Arabia.
E-mail: najoua.h@laposte.net
Epidemiology
Hail Saudi Arabia
杂志排行
Asian Pacific Journal of Tropical Medicine的其它文章
- A brief review on biomarkers and proteomic approach for malaria research
- Trigonelline protects the cardiocyte from hydrogen peroxide induced apoptosis in H9c2 cells
- In vitro cholinesterase inhibitory and antioxidant effect of selected coniferous tree species
- Monascus pilosus-fermented black soybean inhibits lipid accumulation in adipocytes and in high-fat diet-induced obese mice
- Antiprotozoal assessment and phenolic acid profiling of five Fumaria (fumitory) species
- Change of MicroRNA-134, CREB and p-CREB expression in epileptic rat