脑干胶质瘤磁共振成像影像与病理分级关系的临床研究
2015-12-05郝健
郝 健
脑干胶质瘤磁共振成像影像与病理分级关系的临床研究
郝 健①
目的:探讨脑干胶质瘤(BSG)病理分级与磁共振成像(MRI)影像的关系。方法:对98例BSG患者的临床资料进行回顾性分析,按病理级别将其分为两组,其中66例为低级别组BSG,32例为高级别组BSG,并分析不同病理分级BSG的MRI影像表现。结果:对两组患者胶质瘤生长方式进行比较无差异,但高级别组基底动脉包绕、坏死及跨中线生长的比例显著高于低级别组,两组相比差异有统计学意义(x2=15.548,x2=22.970,x2=9.393;P<0.01)。而低级别组患者囊性病变的比例明显高于高级别组,差异有统计学意义(x2=7.625,P<0.01)。高级别组肿瘤直径>2 cm的患者比例高于低级别组,差异有统计学意义(x2=5.331,P<0.05)。高级别组强化形态主要以花环样、壁结节为主,强化程度明显强于低级别组,强化均匀性方面主要表现为不均匀性特征。两组MRI测量最小厚度比较无差异,但高级别组MRI测量最大厚度、最大厚度与最小厚度的比值及差值明显大于低级别组,差异有统计学意义(t=-22.689,P<0.001)。结论:BSG的MRI影像及MRI增强特征可预测和判断BSG的病理分级及恶性程度。
脑干胶质瘤;磁共振成像;影像;病理分级
[First-author’s address] Department of Medical Imaging, The 421thHospital of Chinese PLA, Guangzhou 510318, China.
脑干胶质瘤(brainstem glioma,BSG)为中枢神经系统肿瘤,好发于年龄较小人群,占儿童颅内肿瘤的10%以上[1-2]。不同病理级别的BSG其磁共振成像(MRI)影像表现不尽相同,具有各自特征[3-4]。本研究对98例BSG患者的临床资料进行回顾性研究,旨在探讨BSG不同病理分级与其MRI影像表现之间的关系,以期为临床诊断BSG提供一定的研究依据。
1 资料与方法
1.1 一般资料
选取2010年12月至2012年12月期间在解放军第421医院诊治的98例BSG患者的临床资料,年龄3~52岁,平均年龄为(24.87±5.08)岁,所有患者均符合WHO BSG的诊断标准,并按病理级别将其分为两组,其中66例为低级别组BSG,32例为高级别组BSG。
1.2 设备及扫描参数
MRI采用Siemens Essenza 1.5 T磁共振成像仪,头部线圈。注射Gd-DTPA 0.1 mmol/kg,T1加权像轴位矢状位冠状位扫描[5]。
1.3 影像学处理
根据BSG的MRI影像上最大直径(>2 cm与≤2 cm)、内生型肿瘤是否跨脑干轴位中线生长(如图1a所示)、T1WI信号改变是否均匀低信号或混杂信号、T2WI信号改变是否均匀高信号或混杂高信号、增强效应有无强化、肿瘤有无囊变(如图1b所示)、肿瘤中心有无坏死(如图1c所示)以及肿瘤对基底动脉有无包绕及MRI增强特征(如图1d所示)等结果为变量分析和病理分级的关系[6]。
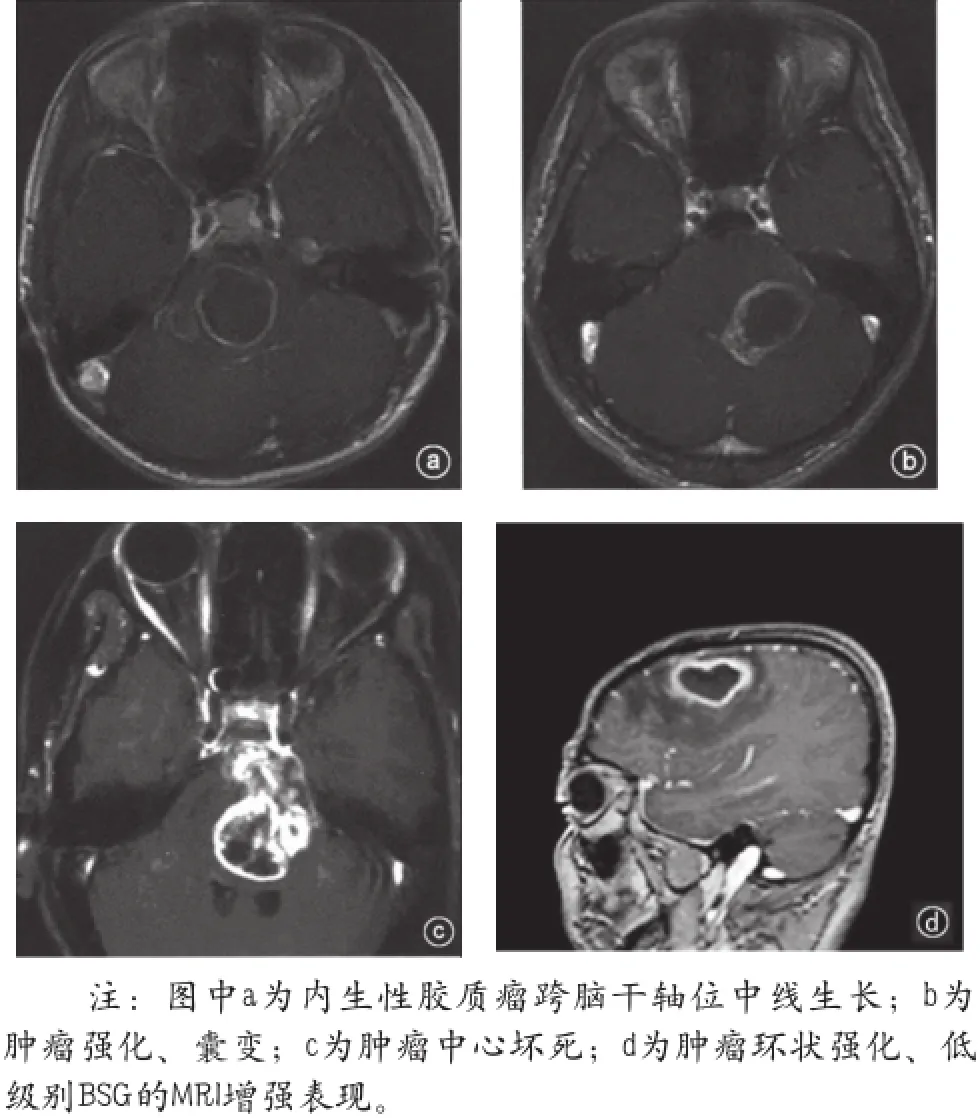
图1 BSG的MRI影像图
1.4 观察指标
对不同病理级别的两组患者的临床资料、MRI影像表现与病理级别的关系、MRI影像增强特征与病理级别以及MRI测量结果与病理级别等指标进行比较分析。
1.5 统计学方法
使用SPSS 18.0统计软件进行数据统计,计数资料使用%或以均值±标准差(x-±s)表示,应用卡方进行计数资料的检验,计量资料采用t检验,对MRI增强结果采取独立样本t检验,以P<0.05为差异有统计学意义。
2 结果
2.1 两组临床资料分析
两组患者基本资料比较结果显示,低级别组患者病理分级皆为I级、II级,高级别组病理分级皆为III级、IV级。两组年龄、性别、民族、病程、学历以及肿瘤部位等资料比较差异不显著,见表1。
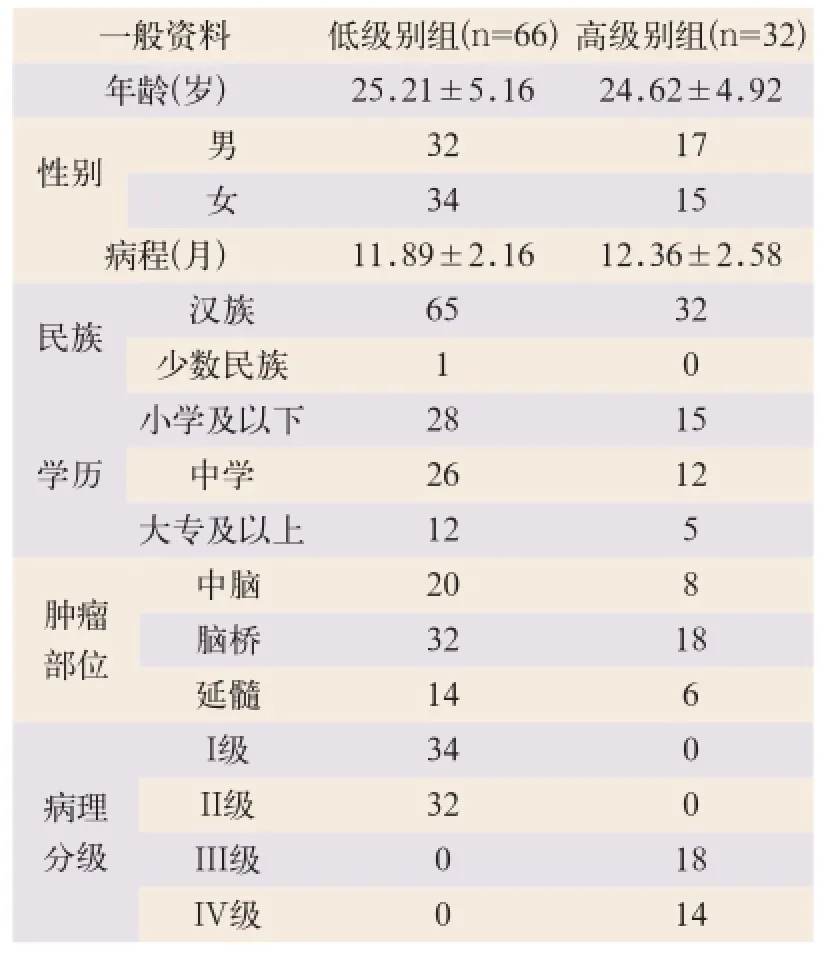
表1 不同病理分级患者的一般资料比较(例,x-±s)
2.2 MRI影像表现与病理级别的关系
两组患者MRI表现比较结果显示:两组胶质瘤生长方式比较无差异,但高级别组基底动脉包绕、坏死及跨中线生长的比例显著高于低级别组,两组相比差异有统计学意义(x2=15.548,x2=22.970,x2=9.393;P<0.01)。而低级别组患者囊性病变的比例明显高于高级别组,两组相比差异有统计学意义(x2=7.625,P<0.01)。高级别组肿瘤直径>2 cm的患者比例高于低级别组,差异有统计学意义(x2=5.331,P<0.05),见表2。

表2 BSG的MRI影像表现与病理级别的关系比较(例)
2.3 BSG的MRI影像增强特征与病理级别
两组患者MRI增强特征比较结果显示,高级别组强化形态主要以花环样、壁结节为主,强化程度明显强于低级别组,强化均匀性方面主要表现为不均匀性特征,两组相比较其差异有统计学意义(x2=12.873,P<0.01),见表3。
2.4 BSG的MRI测量结果与病理级别
两组患者MRI测量结果显示,两组MRI测量最小厚度比较差异无统计学意义(t=-0.860,P=0.391)。但高级别组MRI测量最大厚度,最大厚度与最小厚度的比值及差值明显大于低级别组,差异有显著统计学意义(t=-22.689,P<0.001),见表4。

表3 BSG的MRI增强特征与病理级别的关系比较(例)
表4 BSG的MRI测量结果与病理级别的关系比较

表4 BSG的MRI测量结果与病理级别的关系比较
病理级别例数最大厚度(mm)最小厚度(mm)最大和(或)最小(mm)最大和(或)最小(mm)低级别组662.85±1.02a1.09±0.612.21±1.66a1.58±0.62a高级别组328.26±1.271.21±0.727.32±3.826.91±1.78 t值-22.6890-0.8603-9.2493-21.8414 P值0.00000.39180.00000.0000
3 讨论
BSG好发于脑桥,也可累及多个部位[7-8]。其生长方式(局灶内生型、外生型)与病理分级的关系目前尚无定论,但多数学者认为胶质瘤生长方式和病理级别无明显相关性[9-14]。本研究中两组胶质瘤生长方式比较差异无统计学意义,与相关文献报道一致,提示胶质瘤生长方式与其病理级别关联度较小。不同病理级别BSG的MRI影像表现存在一定的差异。Dellaretti等[1]报道病理级别、恶性程度较高患者的MRI影像表现和级别、恶性度较低患者的MRI影像表现差异明显,高级别BSG发生基底动脉包绕、坏死及跨中线生长的几率要远高于低级别胶质瘤患者。Yamasaki等[5]的多中心研究显示,低级别BSG出现囊性病变的比例远高于高级别胶质瘤。Dellaretti等[9]报道BSG的MRI影像表现和胶质瘤病理分级密切相关,可以利用MRI影像结果对BSG组织学诊断、恶性程度及患者预后、生存时间进行预测。本研究对两组患者MRI表现进行比较,结果显示,高级别组基底动脉包绕、坏死及跨中线生长的比例显著高于对照组,两组差异有显著统计学意义。而低级别组患者囊性病变的比例明显高于高级别组,差异有显著统计学意义,和相关文献报道一致。提示BSG的MRI影像表现和胶质瘤病理分级关系密切,可以用于胶质瘤恶性程度高低及患者预后的预测。
Yamasaki等[5]报道肿瘤MRI影像显示直径越大,其恶性程度往往较高,直径>2 cm的胶质瘤病理级别及恶性程度往往较高,患者预后较差。本研究显示,高级别组肿瘤直径>2 cm的患者比例高于低级别组,和Fumiyuki等的观点相符。提示胶质瘤大小和恶性程度及患者预后同样相关,也可作为预测因子之一。
Davison等[7]报道不同病理级别的BSG的MRI增强结果差异较大。Janssens等[8]对儿童的一项尝试性研究显示,高级别BSG的MRI强化形态、强化程度和均匀性与低级别胶质瘤的MRI强化结果差异极大,Rachinger等[14]的回顾性研究同样证实了这一点。Rachinger等的研究显示,高级别与低级别胶质瘤之间MRI的测量结果同样存在很大差异。本研究对两组患者MRI增强特征进行比较结果显示,高级别组强化形态主要以花环样、壁结节为主,强化程度明显强于低级别组;强化均匀性方面主要表现为不均匀性特征。对两组患者MRI测量结果进行比较结果显示,两组MRI测量最小厚度比较差异无统计学意义,但高级别组MRI测量最大厚度,最大厚度与最小厚度的比值及差值明显大于低级别组,这与文献报道相接近。由于BSG的浸润性生长可以破坏正常血管的分布及生长,引发异常血管的出现,恶性程度越高的胶质瘤,其异常血管生成比例越高,且分布表现不均,因此MRI增强强化的结果可表现出异常血管的强化影像很明显,而高级别BSG伴有异常血管分布不均,因此可表现为强化不均匀性的特征,同时也表现为花环样图像。由于异常血管生长及恶性胶质瘤本身肿瘤细胞的异常繁殖,因此其测量厚度明显较高,提示BSG的MRI增强特征同样可以预测胶质瘤病理级别及恶性程度。
本研究的不足之处是高级别BSG样本量相对较小,因此可能会影响结果的精确性,因此仍然需要更大规模的样本进行深入研究。
[1]Dellaretti M,Touzet G,Reyns N,et al. Correlation between magnetic resonance imaging findings and histological diagnosis of intrinsic brainstem lesions in adults[J].Neuro Oncol,2012,14(3):381-385.
[2]Ogiwara H,Morota N.The efficacy of a biopsy of intrinsic brainstem lesions for decision making of the treatments[J].Childs Nerv Syst,2013,29(5):833-837.
[3]Tsutsumi M,Akimoto J,Nakajima N,et al.Two cases of posterior reversible encephalopathy syndrome resembling brainstem glioma[J].Clin Neurosurg,2012,114(7):1062-1065.
[4]Reyes-Botero G,Mokhtari K,Martin-Duverneuil N,et al.Adult brainstem gliomas[J].The oncologist,2012,17(3):388-397.
[5]Yamasaki F,Kurisu K,Kajiwara Y,et al. Magnetic resonance spectroscopic detection of lactate is predictive of a poor prognosis in patients with diffuse intrinsic pontine glioma[J]. Neuro Oncol,2011,13(7):791-801.
[6]Agamanolis DP,Katsetos CD,Klonk CJ.et al.An unusual form of superficially disseminated glioma in children: Report of 3 cases[J].Journal of child neurology,2012,27(6):727-733.
[7]Davison JE,Davies NP,English MW,et al. Magnetic resonance spectroscopy in the diagnostic evaluation of brainstem lesions in Alexander disease[J].Journal of child neurology,2011,26(3):356-360.
[8]Janssens GO,Gidding CE,Van-Lindert EJ,et al.The role of hypofractionation radiotherapy for diffuse intrinsic brainstem glioma in children:a pilot study[J].Int J Radiat Oncol Biol Phys,2009,73(3):722-726.
[9]Dellaretti M,Touzet G,Reyns N,et al.Correlation among magnetic resonance imaging findings,prognostic factors for survival and histological diagnosis of intrinsic brainstem lesions in children[J].J Neurosurg Pediatr,2011,8(6):539-543.
[10]Hinnell C,Almekhlafi M,Joseph JT,et al. Concurrence of high-grade brainstem glioma and multiple sclerosis[J].Can J Neurol Sci,2010,37(4):512-514.
[11]李健,武永康,董伦,等.脑胶质瘤磁共振成像增强特征与病理分级相关性研究[J].医学综述,2011,17(11):1725-1727.
[12]Rosenschold P,Engelholm S,Ohlhues L,et al. Photon and proton therapy planning comparison for malignant glioma based on CT,FDG-PET,DTI-MRI and fiber tracking[J]. Acta Oncologica,2011,50(6):777-783.
[13]万贻绿,漆松涛,方陆雄,等.94例脑干胶质瘤MRI影像与病理分级的关系分析[J].中华神经外科杂志,2012,28(4):346-349.
[14]Rachinger W,Grau S,Holtmannspotter M,et al.Serial stereotactic biopsy of brainstem lesions in adults improves diagnostic accuracy compared with MRI only[J].J Neurol,Neurosurg Psychiatry,2009,80(10):1134-1139.
Clinical study on the corration of pathological classification of brainstem glioma with MRI imaging
HAO Jian// China Medical Equipment,2015,12(1):92-95.
Objective: To explore the corration of pathological classification of brainstem glioma with MRI imaging. Methods: The clinical data of 98 patients with BSG was retrospectively analyzed. of 98 patients, 66 cases were low level of brainstem gliomas, 32 cases were high level of brainstem gliomas. MRI images of different pathological grading of BSG were analyzed. Results: Glioma growth way was similar between the two groups and there was no statistical significance. But the proportion of basal artery circumvolutio, necrosis, growth across the midline of the high level group were significantly higher than the control group, there was a significant statistical significance (P<0.01). And the proportion of the cystic lesion in patients of low level group was obviously higher than that of high level group, with significant difference (P<0.01). of high level group patients with a ratio of tumor >2 cm in diameter was higher than the control group, and the difference was statistically significant (P<0.05). The improved forms of high level group were mainly wreath, wall nodules (P<0.01), and improved significantly stronger than the low level group (P<0.01). The main uniformity of high level group in show was characteristics with less uniformity (P<0.01). The MRI measuring minimum thickness was similar between the two groups and had no statistical significance. But MRI measuring thickness, the ratio and gap between maximum thickness and minimum thickness of high level group were bigger than the value of low level group, with statistically significant difference (P<0.001). Conclusion: MRI imaging and MRI enhanced characteristics of brainstem glioma may predict and judge the malignant degree and pathological grading of brainstem glioma.
Brainstem glioma; Magnetic resonance imaging; Imaging; Pathological grading
郝健,男,(1960- ),本科学历,副主任医师。解放军第421医院医学影像科主任,从事医学影像诊断工作。
1672-8270(2015)01-0092-04
R445.2
A
10.3969/J.ISSN.1672-8270.2015.01.029
2014-04-08
①解放军第421医院医学影像科 广东 广州 510318
