股骨粗隆间骨折手术并发股深动脉动静脉瘘一例报告
2015-10-14宋迪煜张树明乔林王奎友
宋迪煜 张树明 乔林 王奎友
. 病例报告 Case report .
股骨粗隆间骨折手术并发股深动脉动静脉瘘一例报告
宋迪煜 张树明 乔林 王奎友
股骨;骨折;血管系统损伤;手术后并发症;病例报告
股骨粗隆间骨折并发的医源性血管损伤是一种非常少见的并发症,其发生率约为 0.21%[1]。最早由 Dameron[2]于 1964 年报道 1 例,此后相继有部分病例报道,其损伤形式主要表现为假性动脉瘤或血肿[3]。笔者经治 1 例股骨粗隆间骨折防旋股骨近端髓内钉 ( proximal femoral nail antirotation,PFNA ) 固定术后第 8 天并发股深动脉动静脉瘘,经积极诊断、治疗,获得满意效果。此病例的特别之处在于其血管损伤类型为动静脉瘘,目前还未见有此类病例报道。
资料与方法
1. 一般资料:患者,女,77 岁,主因“摔伤致左髋部疼痛伴活动受限 8 小时”入院,既往有甲状腺功能减退症病史 10 余年,糖尿病病史 8 年,高血压病病史 5 年,伤前生活能自理。根据 X 线结果,明确诊断为左股骨粗隆间骨折 ( 31-A2.1 )。入院时查体可以发现:双下肢无明显肿胀,双侧足背动脉搏动正常,足趾毛细血管充盈实验正常。血常规提示血红蛋白 133 g / L。入院后完善术前准备,常规给予低分子肝素钙预防血栓治疗至术前 1 天。
2. 治疗方法:入院后第 8 天行手术治疗,手术常规在牵引床上进行,患肢适当牵引,并轻度内收内旋,骨折复位顺利,对线对位满意。按常规行 PFNA 内固定手术,术中插入导针顺利,并未穿透骨折端进入周围软组织,远端2 枚锁钉固定。术中输红细胞 400 ml、血浆 200 ml。术后常规给予预防感染、预防血栓、控制血糖及血压等治疗,术后第 1 天复查血常规提示:血红蛋白 109 g / L,红细胞比积 33.6%。
术后第 8 天,患者出现患肢大腿内侧明显疼痛、肿胀、青紫,患肢足背动脉仍搏动正常,末梢血运正常,体温正常,行下肢 B 超提示:未见明显异常,暂给予止痛、消肿等对症治疗,效果欠佳,此后患侧大腿疼痛、肿胀逐渐加重,以夜间明显。术后第 10 天,复查血常规提示:血红蛋白 70 g / L,红细胞比积降至 22.2%,给予输血 800 ml;术后第 12 天,再次复查血常规:血红蛋白 69 g / L,红细胞比积降至 21.5%。以上情况提示存在持续性失血,患肢血管损伤可能性大。急诊行左下肢血管造影术,术中发现股深动脉第一穿支的 4 级分支于小转子下方血管漏血,存在动静脉瘘 ( 图 1,2 ),给予第一穿支动脉弹簧圈栓塞,栓塞后见造影剂渗出停止 ( 图 3 ),栓塞效果好。栓塞术后给予输红细胞 800 ml,复查血常规提示:血红蛋白 88 g / L,红细胞比积 27.7%。术后患侧大腿疼痛明显减轻,肿胀逐渐消退,顺利出院。随访 6 个月,患者患肢已无疼痛,肿胀消退,患肢功能恢复良好。
讨 论
股骨粗隆间骨折手术并发损伤的血管主要包括股总动脉、股浅动脉、股深动脉及其分支。Bartonicek[4]认为,相比较而言,股深动脉更容易受到损害。Chan 等[5]认为,内旋下肢可使股深动脉更加贴近股骨皮质,而过度钻孔容易损伤股深动脉及第一、二穿支,其位置相当于 DHS的第 3、4 板孔。血管损伤可有不同的受伤机制,锋利的骨折块、突出皮质的螺钉尖、远端锁钉可刺伤或挤压损伤血管[3];电钻过度钻孔或不恰当放置的牵开器也可损伤血管[6];此外,当突出的螺钉长时间的刺激或腐蚀血管时也能造成血管损伤[7]。目前文献报道的动脉损伤类型包括假性动脉瘤[6,8]、动脉撕裂[9]、动脉堵塞[10]、小分支血管断裂[3]等,其中最主要损伤类型是假性动脉瘤[11]。
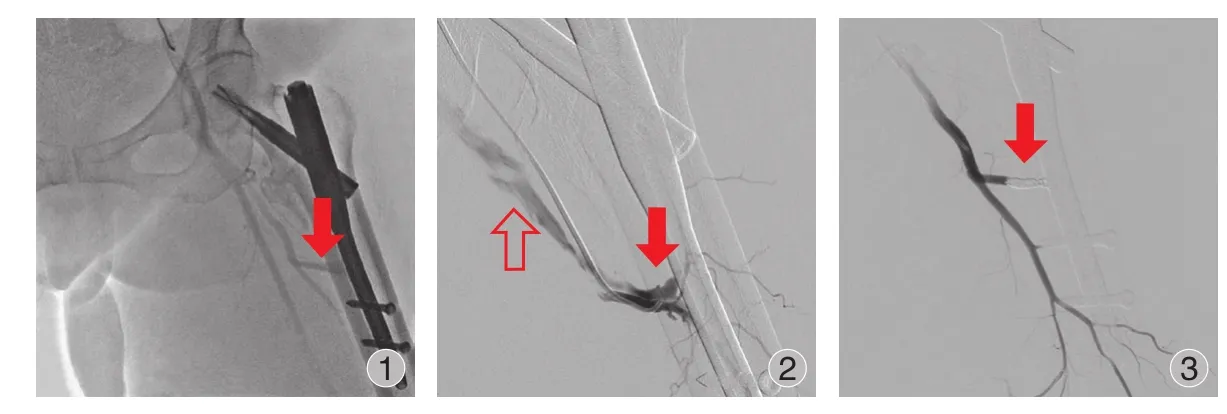
图 1 股深动脉第一穿支造影剂显示异常 ()图 2 血管损伤部位在第一穿支 (),静脉提前显影 () 说明存在动静脉瘘图 3 成功用弹簧圈栓塞股深动脉第一穿支 ()Fig.1 Contrast agent of the frst perforating artery of the profunda femoris artery was abnormal ()Fig.2 The site of injured artery located in the first perforating artery (), and the contrast agent developed ahead of time in the vein (), which implied the presence of arteriovenous fstulaFig.3 Successful coil embolisation of the frst perforating artery ()
本例血管损伤表现为股深动脉第一穿支动静脉瘘,位于粗隆间骨折部位与远端第一个锁钉之间;考虑到术中骨折复位顺利,亦未发现导针穿出骨折部位,因此被骨折块、或螺钉、或电钻、或导针损伤血管的可能性不大。Ryzewicz[3]曾报道 1 例股骨粗隆间骨折手术并发股深动脉分支损伤的病例,其损伤部位位于内固定远端,其考虑可能是牵拉损伤血管。本例患者为老年女性,血管弹性、质量下降,损伤血管紧贴股骨,因此也不能排除牵拉所致血管损伤可能。
有文献报道,血管损伤所致动静脉瘘的发生率约2%~4%[12]。在髋部骨折手术相关的文献中还未有此类损伤形式的记载。创伤性动静脉瘘最常见的临床表现是肢体出血、血肿、肿胀,触诊有震颤,听诊有血管杂音,甚至出现心衰症状[13]。本例主要表现为肢体剧烈疼痛、肿胀、血色素进行性下降,未发现局部震颤性包块、血管杂音,肢体末梢血运也是正常的,其原因可能是损伤部位深,且是 4 级分支小血管损伤。
血管损伤的最后确诊依赖于影像学检查,常用的无创性成像检查有超声多普勒、CT 血管成像。目前血管造影仍是金标准,它不仅能够明确动脉损伤性质,而且能同时进行治疗[6]。动脉损伤的治疗应根据损伤的解剖学部位及损伤大小决定,不重要的分支或可牺牲的血管可采用微创方法栓塞,而重要的血管需进行重建术[3]。已有的文献报道中多采用经皮经导管弹簧圈栓塞,其疗效确切,被认为是最有效的方法[6,8]。
综上所述,股骨粗隆间骨折手术并发动脉损伤虽然少见,但也应该引起足够的重视。股骨粗隆间骨折牵引复位时不宜反复使用暴力,尤其是存在小粗隆移位的病例;手术操作需仔细,避免过度牵拉,钻头穿透内侧皮质后应避免过度往里钻,以免损伤内侧软组织,螺钉长度要适宜等等。如术后如出现不明原因的患侧大腿疼痛、肿胀、血色素进行性下降等,应警惕动脉损伤的发生;一旦怀疑存在动脉损伤,尽可能行动脉造影;当明确诊断为次要血管损伤时,经导管动脉弹簧圈栓塞是一个有效的治疗方法。
[1] Karanikas I, Lazarides M, Arvanitis D, et al. Iatrogenic arterial trauma associated with hip fracture surgery. Acta Chir Belg,1993, 93(6):284-286.
[2] Dameron TBJ. False aneurysm of femoral profundus artery resulting from internal-fixation device (screw). J Bone Joint Surg (Am), 1964, 46:577-580.
[3] Ryzewicz M, Robinson M, McConnell J, et al. Vascular injury during fxation of an intertrochanteric hip fracture in a patient with severe atherosclerosis. A case report. J Bone Joint Surg(Am), 2006, 88(11):2483-2486.
[4] Bartonicek J. Injuries to femoral vessels in fractures of the hip. Rozhl Chir, 2009, 88(4):203-205.
[5] Chan WSW, Kong SW, Sun KW, et al. Pseudoaneurysm and intramuscular haematoma after dynamic hip screw fxation for intertrochanteric femoral fracture: a case report. J Orthop Surg(Hong Kong), 2010, 18(2):244-247.
[6] Singh S, Arora S, Thora A, et al. Pseudoaneurysm of profunda femoris artery following dynamic hip screw fixation for intertrochanteric femoral fracture. Chin J Traumatol, 2013,16(4):233-236.
[7] Ritchie ED, Haverkamp D, Schiphorst TJMJ, et al. False aneurysm of the profunda femoris artery, a rare complication of a proximal femoral fracture. Acta Orthop Belg, 2007,73(4):530-532.
[8] Patelis N, Koutsoumpelis A, Papoutsis K, et al. Iatrogenic injury of profunda femoris artery branches after intertrochanteric hip screw fixation for intertrochanteric femoral fracture: a case report and literature review. Case Rep Vasc Med, 2014,2014:694235.
[9] Tomcovcík L, Kovác P, Dano J, et al. Late laceration of the superficial femoral artery by an intertrochanteric fracture fragment. Hip Int, 2011, 21(2):273-277.
[10] Bansal R, Laing PW. Iatrogenic blunt arterial injury during a hip fracture surgery. Acta Orthop Belg, 2006, 72(1):96-99.
[11] Li X, Luckeroth PD, Curry EJ, et al. Pseudoaneurysm of the profunda femoris artery following a long anterograde intramedullary nail for an unstable intertrochanteric hip fracture: A case report and review of the literature. Eur J Orthop Surg Traumatol, 2010, 21(4):293-299.
[12] Toit du DF, Leith JG, Strauss DC, et al. Endovascular management of traumatic cervicothoracic arteriovenous fstula. Br J Surg, 2003, 90(12):1516-1521.
[13] Yildirim S, Oguzkurt L, Tarim A, et al. Endovascular treatment of traumatic femoral arteriovenous fstula. Euro J Radiol Extra,2005, 55(1):33-35.
( 本文编辑:王永刚 )
Arteriovenous fistula of profunda femoris artery following fixation of intertrochanteric hip fracture: 1 case report
SONG Di-yu, ZHANG Shu-ming, QIAO Lin, WANG Kui-you. Department of Orthopedics, the second Artillery General Hospital PLA, Beijing, 100088, PRC
Vascular injury is a rare complication following the fxation of intertrochanteric femoral fracture. A case of profunda femoris artery injury after intertrochanteric hip fracture fixation with PFNA will be reported. Arterial injury's manifestation is arteriovenous fstula, which has not been reported before. This patient presented with excessive thigh swelling, substantial pain and progressive drop of haemoglobin 8 days postoperatively. Diagnosis was confrmed by angiographic study and it was successfully treated by coil embolization.
Femur; Fractures, bone; Vascular system injuries; Postoperative complications; Case reports
10.3969/j.issn.2095-252X.2015.12.019
R683, R619
100088 北京,第二炮兵总医院骨科
2015-05-06 )