脑梗死49例的临床特点、治疗方案及CT影像表现分析
2015-07-22首都医科大学附属北京康复医院北京100144
首都医科大学附属北京康复医院(北京 100144)
关利利 郭龙军
脑梗死49例的临床特点、治疗方案及CT影像表现分析
首都医科大学附属北京康复医院(北京 100144)
关利利 郭龙军
目的 研究49例脑梗死患者临床特点、治疗方案及CT影像表现分析。方法选取我院2014年12月至2015年7月49例脑梗死患者为研究对象,≥65岁以上设为老年组(29例),<65岁设为中年组(20例),比较两组临床表现及CISS分型差异,并给予静脉溶栓治疗,随访1月观察治疗方案疗效,最后通过分析头颅CT平扫结果,观察脑梗死患者CT影像表现特征。结果 老年组CISS分型中UE 10例与中年组比较显著较高(P<0.05),49例患者以LAA、UE型较为多见。老年组偏瘫、意识障碍、大小便失禁者较中年组明显较多,而中年组头痛人数较老年组明显较高,组间比较差异有统计学意义(P<0.05),49例患者以意识障碍、偏瘫、头痛为主要临床表现;溶栓治疗1月后进行结果观察,49例患者1例死亡,1例植物生存,GOS评分5分16例,4分22分,3分9例,GOS评分(3.24±0.59)分,较治疗前差异显著(P<0.05);49例患者中,CT扫描可见病灶数215个,其中腔隙性脑梗死38例,多发性脑梗死11例,病变分布:小脑梗死15例、皮质梗死17例、脑干梗死10例、基底节区梗死7例。结论 不同脑梗死患者临床特点存在明显差异,老年患者以UE分型多见,且偏瘫、大小便失禁、意识障碍发生率高,而中年患者则表现为头痛,静脉溶栓治疗脑梗死预后较良好,CT诊断可有利于临床的病情评估,可为临床治疗及临床特点分析提供可靠依据,
脑梗死;CT影像表现;治疗
脑梗死指局部脑组织因血液循环障碍出现缺氧、缺血而导致的软化坏死,主要因脑血液动脉发生动脉粥样硬化及血栓,管腔有不同程度的狭窄或闭塞,进而引发局灶性急性脑供血不足发病,患者症状根据病情进展程度存在明显差异[1]。脑梗死占所有脑血管疾病的50%~60%,且病死率达10%~15%,预后较差[2-3]。早期有效诊断对脑梗死临床特点、治疗方案的选择有重要的指导价值。本次研究对49例脑梗死患者临床特点、治疗方案及CT影像特征进行分析,旨在为脑梗死今后诊治提供参考依据。
1 资料与方法
1.1 一般资料选取我院2014年12月至2015年7月49例脑梗死患者为研究对象,其中男27例,女22例,年龄51~79岁,平均(62.36±5.14)岁,合并症:高血压27例,高脂血症12例,糖尿病史17例。临床表现:偏瘫19例,头痛18例,失语13例,意识障碍21例,大小便失禁10例。
1.2 治疗方式均采取静脉溶栓治疗,根据患者体质量给予重组组织型纤溶酶原激活剂(rt-PA),0.9mg/kg,总剂量90mg,10%静脉推注给药,剩余总剂量1h内缓慢泵入。
1.3 诊断方式采用日本岛津 TSCT—7000TX/TE 扫描仪进行头颅CT扫描,患者取仰卧位,横断面(轴位)平扫,横断扫描为听眦线为基线,层厚10mm、层距10mm进行全脑扫描,如扫描区发生异常,加5mm薄层扫描,参数:120kV,210mAs,FOV250mm,矩阵512×512。
1.4 观察指标①≥65岁设为老年患者,<65岁为中年组,比较两组临床表现及CISS分型[4]的分布情况;②随访3月对治疗效果进行观察,与入院时格拉斯哥预后评分(GOS)评分进行比较以评价治疗方案的临床效果,GOS共1-5分,分数越高表示预后越好;③分析患者头颅CT影像学特征。
1.5 统计学方法选用统计学软件SPSS19.0对研究数据进行分析和处理,计数资料采取率(%)表示,组间对比进行χ2检验,以P<0.05为有显著性差异和统计学意义。
2 结 果
2.1 脑梗死临床特点CISS分型老年组LAA 11例、CS 3例、PAD 3例、OE 2例,中年组LAA 9例、CS 4例、PAD 4例、OE 2例,比较无统计学意义(P>0.05),老年组UE 10例与中年组1例比较显著较高(χ2=5.910,P<0.05),48例患者以LAA、UE型较为多见。老年组偏瘫、意识障碍、大小便失禁者较中年组明显较多,而中年组头痛人数较老年组明显较高,组间比较差异有统计学意义(P<0.05),49例患者以意识障碍、偏瘫、头痛为主要临床表现。见表1。
2.3 CT诊断结果49例患者中,CT扫描可见病灶数215个,其中腔隙性脑梗死38例,多发性脑梗死11例,病变分布:小脑梗死15例、皮质梗死17例、脑干梗死10例、基底节区梗死7例。
2.4 头颅CT平扫图像两侧基底节区、侧脑室旁及半卵圆中心可见斑点、斑片状低密度灶,较大者0.5*0.5cm,CT值约13hu;两侧侧脑室前后角低密度区,边缘模糊;脑干、小脑大脑实质内未见明显异常密度影;脑室系统大小稍扩大;脑沟、裂、池增宽;中线结构居中。考虑为脑内腔隙性脑梗死,脑白质变性,老年颅脑改变。见图1。左
2.2 治疗结果溶栓治疗1月后进行结果观察,49例患者1例死亡,1例植物生存,GOS评分5分16例,4分22分,3分9例。侧基底节区片状低密度灶,大小1.6*0.85cm,CT值13hu,右侧基底节区斑点状低密度灶;两侧侧脑室前后角低密度区,边缘模糊;脑干、小脑大脑实质内未见明显异常密度影;侧脑室扩大,左右侧脑室不对称;脑沟、裂、池增宽;中线结构居中。考虑脑软化灶、脑内腔隙性脑梗死,脑白质变性,老年颅脑改变。见图2。

表1 中、老年患者脑梗死临床特点[例数(%)]
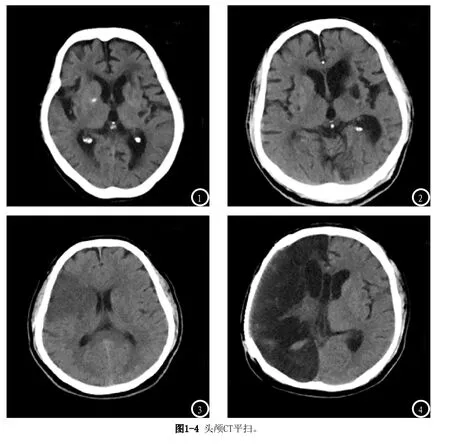
两侧基底节区、放射冠及半卵圆中心多发斑点及大片状低密度影,脑室系统形态如常,脑沟、裂、增宽;中线结构居中。考虑为脑内多发脑梗死,老年颅脑改变。见图3。右侧大脑半球大面积低密度灶,CT值14hu;左侧基底节区斑片状低密度灶;脑干、小脑实质内未见明显异常密度影;右侧侧脑室扩大;左侧脑沟、裂未见明显增宽;中线结构居中。右侧颅骨部分缺如,可见金属影覆盖。考虑右侧大脑半球脑软化灶,腔隙性脑梗死,去骨瓣减压术后改变。见图4。
3 讨 论
近年脑梗死的临床研究较多,诊断技术也逐渐成熟,如DSA、MRI均已成为脑梗死诊断的常用方式,但操作难度高,对设备要求高,因此在部分医院内难以开展,CT影像学因经济、便捷,目前仍为诊断脑梗死的最主要方式[5]。CT诊断脑根死主要机制在于可显示梗死部位及病灶范围,可用于鉴别梗死和出血,并可以此判断出血性梗死、多发性梗死、分水岭梗死等,而诊断不明确者通过造影增强CT扫描可获得较为准确的图像信息[6]。CT诊断可在早期排除脑出血,同时有研究认为,早期CT影像学显示局部脑实质轻微降低,脑动脉高密度中征,且有局部脑肿胀,可为临床确诊提供依据[7-8]。
通过对49例患者临床特点的分析可见,老年患者更易发生偏瘫、意识障碍、大小便失禁,而中年患者临床特点则以头痛居多,同时中年组UE型例数显著低于老年组,考虑与基因、血管发育有关[9]。同时研究显示脑梗死患者采取静脉溶栓治疗预后良好。本次研究可见,通过头颅CT平扫可清晰显示两侧基底节区、侧脑室旁及半卵圆中心,对脑干、小脑及大脑实质等部位密度影进行观察,从而分析脑内多发脑梗死、老年颅脑改变、脑白质变性、腔隙性脑梗死等病理改变[10],本次研究中腔隙性脑梗死38例,多发性脑梗死11例,且病灶部位显像清晰。因此当患者出现语言障碍、头痛等临床表现后,应及时采取头颅CT扫描,从而实现病情的准确评估[11]。但也有研究显示,CT诊断<2mm直径的梗死灶效果较差,且容易受颅底骨质伪影的干扰,且检测脑干及小脑梗死的准确率较低,在发病早期(24h内)时检出率低,需引起临床重视[12]。
综上,脑梗死临床特征明显,静脉溶栓治疗效果显著,通过早期CT诊断可对病情进行准确评估,也可为治疗方案的选择及临床特点的分析提供依据。
[1]王春生.4 5例早期脑梗死C T影像诊断分析[J].河北医学,2013,19(1):134-137.
[2]朱仁洋,王黎萍,孙新芳,等.ABCD2评分联合头颅CT影像在TIA预后评估中的价值[J].浙江临床医学,2015,21(6):1017-1018.
[3]杨春燕,梅友泉,苏俊红,等.超急性期大面积脑梗死的C T诊断与应用[J].中国全科医学,2012,15(3):344-347.
[4]Gao S,Wang YJ,Xu AD,et aI.Chinese ischemic stroke subclassification[J].Front Neurol,2011,10(2):6.
[5]石安斌,龙娟,杨秋云,等.16排CT全脑低采样灌注及血管成像在早期脑梗死中的应用价值[J].中国CT和MRI杂志,2013,11(4):29-31.
[6]曹洋,王春.老年静止性脑梗死的CT表现与影像分类及临床分析[J].中国老年学杂志,2013,33(9):2147-2148.
[7]袁明远,陈斌.青壮年非创伤急性脑梗死的病因与影像学特点[J].影像诊断与介入放射学,2012,21(1):18-20.
[8]路融,刘瑛,廖顺明,等.MRI与CT影像检查在老年多发性脑梗死诊断中的应用分析[J].医学影像学杂志,2014,14(4):611-613.
[9]陈小余,宋学文,肖红,等.128层螺旋CT三维成像技术在脑梗死及动脉瘤中的诊断作用[J].中国CT和MRI杂志,2015,17(7):7-10.
[10]徐延峰,康立清,冯俊杰,等.成人脑梗死及脑血肿近期低剂量CT复查的应用[J].临床放射学杂志,2012,31(11):1633-1636.
[11]方东光.老年与中年脑梗死患者CT和MRI对比[J].中国老年学杂志,2012,32(6):1279-1280.
[12]杜飞,郭艳霞.MRI与CT在老年多发性脑梗死病人诊断中的临床结果比较[J].中国老年学杂志,2012,32(3):487-489.
(本文编辑:谢婷婷)
Analysis of the Clinical Features, Treatment Plan and CT Imaging Findings of 49 Cases of Cerebral Infarction
GUAN Li-li, GUO Long-jun. BeiJing Rehabilitation Hospital Of Capital Medical University 100144
Objective To study the clinical features, treatment plan and CT imaging findings of 49 cases of patients with cerebral infarction.Methods 49 cases of patients with cerebral infarction who were admitted into the hospital during December 2014 to July 2015 were selected as the research objects. Patients who were older than or equal to 65 years old were treated as the elderly group (29 cases) while younger than 65 years old as the middle-aged group (20 cases). The clinical manifestations and CISS typing were compared between the two groups. Meanwhile, the intravenous thrombolytic therapy was implemented. With a month of follow-up, the efficacy of treatment plan was observed. Finally, through analyzing the results of head CT scan, the CT findings of patients with cerebral infarction were observed.Results In the elderly group, there were 10 cases of UE in CISS typing which were significantly higher than those in the middle-aged group (P<0.05). Most of the 49 patients were of LAA and UE type. In the elderly group, patients with hemiplegia, consciousness disorders and gatism were significantly more than those in the middle-aged group while patients with headaches in the middle-aged group were more than those in the elderly group. The comparison between groups was statistically significant (P<0.05). The main clinical manifestations of the 49 patients were consciousness disorders, hemiplegia and headaches. After a month of thrombolytic therapy, the results were observed. Among the 49 patients, there was a case of death and a case in persistent vegetative state. There were 16 cases of 5 points of GOS, 22 cases of 4 points and 9 cases of 3 points. GOS were (3.24±0.59) points. Compared with those before the treatment, the difference was significant (P<0.05). Among the 49 patients, there were 215 visible lesions scaned by CT, including 38 cases with lacunae brain infarction and 11 cases with multiple cerebral infarction. The distribution of lesions showed that there was cerebellar infarction in 15 cases, cortex infarction in 17 cases, brain stem infarction in 10 cases and basal ganglia infarction in 7 cases.Conclusion There is significant difference in the clinical characteristics of patients with different cerebral infarction. Most of the elderly patients are UE type and the incidence rates of hemiplegia and gatism in them are high. However, the middle aged patients manifest as headaches. The prognosis of patients who receive thrombolytic therapy for treating cerebral infarction is relatively good. CT diagnosis is beneficial to clinical disease evaluation, which can provide reliable basis for clinical treatment and the analysis of clinical characteristics.
Cerebral Infarction; CT Imaging Findings; Treatment
R651.1
A
10.3969/j.issn.1672-5131.2015.11.003
关利利
2015-10-08
