500例患儿麻醉后躁动的多因素分析
2015-06-01李法印张先龙
李法印,徐 峰,张先龙
(江苏省淮安市第一人民医院麻醉科 223300)
论著·临床研究
500例患儿麻醉后躁动的多因素分析
李法印,徐 峰△,张先龙
(江苏省淮安市第一人民医院麻醉科 223300)
目的 分析该院2年500例患儿麻醉手术后躁动发生的影响因素。方法 该院ASA分级为Ⅰ~Ⅱ级的500例患儿,根据麻醉手术后苏醒的躁动情况分为躁动组和非躁动组。对患儿年龄、性别、体质量、术前焦虑分级、所患疾病种类、ASA分级、麻醉用药种类及剂量、插管、麻醉时间、停药后患儿苏醒时间、患儿苏醒后躁动情况做Logistic回归分析。结果 500例患儿,术后躁动153例,占总数的30.6%;Logistic回归分析得出患儿年龄较大、性别、应用氯胺酮等项目回归系数为负,患儿体质量、术前焦虑分级、七氟醚麻醉、插管等项目回归系数为正;ROC曲线下面积为0.850。结论 患儿体质量、术前焦虑分级、气管插管、七氟醚麻醉可以增加患儿麻醉手术后躁动发生率,而患儿年龄较大、女性患儿、应用氯胺酮可以减少麻醉手术后躁动发生率。
儿童;麻醉;躁动;Logistic回归
小儿术后躁动发生率可以高达80%[1]。一旦术后躁动,可引发诸多意外伤害,这要求临床医生严密监护,必要时采取相应的措施控制术后躁动。作者认真观察了本院2年500例手术麻醉后患儿的躁动发生情况,对术后躁动原因分析如下。
1 资料与方法
1.1 一般资料 收集本院2011年5月至2013年5月麻醉患儿,ASA分级为Ⅰ~Ⅱ级,排除严重心血管、神经系统疾病及手术当日感冒、咳嗽、发热患儿后共入选500例。根据麻醉后苏醒情况分为躁动组和非躁动组。分别记录患儿的年龄、性别、体质量、术前焦虑分级(共4级,1级:患儿熟睡;2级:能够轻易地与父母分开,进入手术室;3级:有些焦虑,但在劝说的情况下可以带进手术室;4级:哭闹,不情愿进入手术室)。手术类型:(1)疝气手术;(2)眼科手术;(3)腺样体肥大手术;(4)小儿烧伤手术;(5)阑尾炎手术;(6)包皮环切术。
1.2 麻醉方法 患儿进入手术室后,对于有严重焦虑情绪的患儿,先辅助吸入七氟醚,待患儿安静后,再开放背静脉;对于无焦虑症状患儿,直接开放静脉。按体质量使用不同静脉麻醉药物,氯胺酮(2 mg/kg)、异丙酚(2 mg/kg)、芬太尼(2~5 μg/kg)、仙林(0.1 mg/kg)等麻醉药物诱导后,做气管插管,异丙酚持续泵入(6~8 mg·kg-1·min-1)或吸入七氟醚(2%~3%)维持麻醉,术中根据手术刺激情况酌情加入芬太尼或者肌肉松弛药物,以增加麻醉深度。小手术如不需插管,则不用肌肉松弛药,保留自主呼吸,吸氧。手术过程中保持小儿心率、血压平稳,氧饱和度维持在95%以上。手术结束时,停止使用麻醉药物。不使用麻醉催醒药物,麻醉恢复室内观察患儿苏醒情况。
患儿在麻醉恢复室内躁动分级根据以下评分进行判断,0级:患儿安静,对耳垂刺激无反应;1级:患儿安静,对耳垂刺激有反应;2级:患儿清醒,对言语有主动反应;3级:患儿清醒,能够感觉到疼痛及各种不适;4级:患儿哭闹;5级:患儿哭闹得厉害,需要采取相应的安静措施。每隔10 min评定1次患儿躁动情况,在恢复室内有1次评分达到4级或5级时,可判断为患儿麻醉后躁动。记录患儿麻醉用药种类及剂量、插管情况、麻醉时间、停药后患儿苏醒时间、患儿苏醒后躁动情况。

2 结果
2.1 500例患儿麻醉手术后躁动情况 500例患儿中,术后发生躁动者153例,占总数的30.6%;非躁动者347例,占总数的69.4%,见表1。
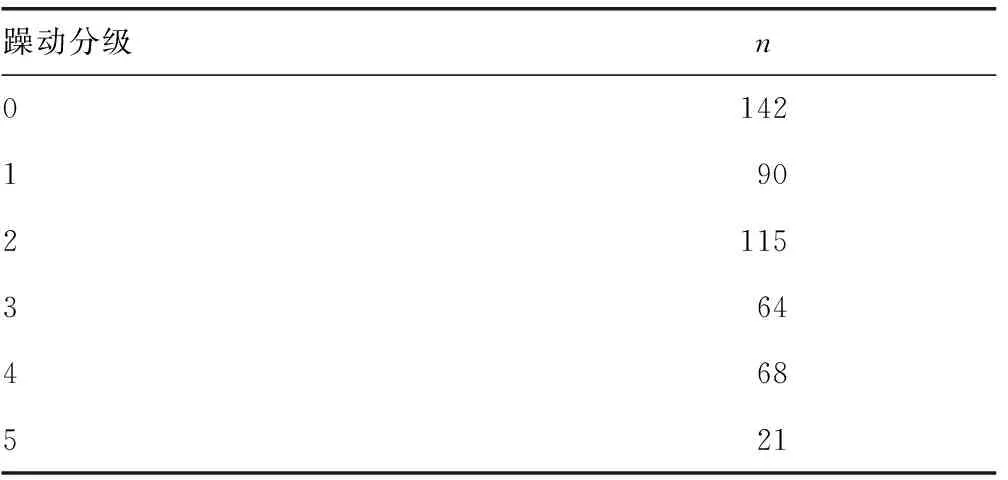
表1500 例患儿麻醉手术后躁动情况
2.2 两组患儿一般临床资料、麻醉药物及相关时间的比较 躁动组患儿年龄偏小,体质量较轻,与非躁动组比较差异有统计学意义(P<0.05)。两组患儿麻醉药物异丙酚、芬太尼使用量、麻醉时间、苏醒时间方面比较差异无统计学意义(P>0.05),见表2。

表2 两组患儿一般临床资料、麻醉药物及相关 时间的比较
2.3 两组患儿一般临床资料及麻醉相关资料的比较 躁动组男性患儿较女性患儿多(P<0.05);患儿术前焦虑分级高,术后躁动发生率也较高,差异有统计学意义(P<0.05);使用氯胺酮做麻醉诱导患儿术后躁动发生率较少,差异有统计学意义(P<0.05);患儿使用肌肉松弛药物、气管插管及用七氟醚做麻醉维持,其术后躁动发生率也较高,差异有统计学意义(P<0.05)。但疾病种类、患儿ASA分级、术前用药对患儿术后躁动的影响差异无统计学意义(P>0.05),见表3。
2.4 Logistic回归方程系数、标准误、OR值及95%可信区间 患儿年龄、性别、氯胺酮使用方面Logistic回归系数为负;体质量、术前焦虑分级、七氟醚使用、术前插管方面Logistic回归系数为正。OR值95%可信区间都不包括0,表明参数有显著统计学意义,见表4。
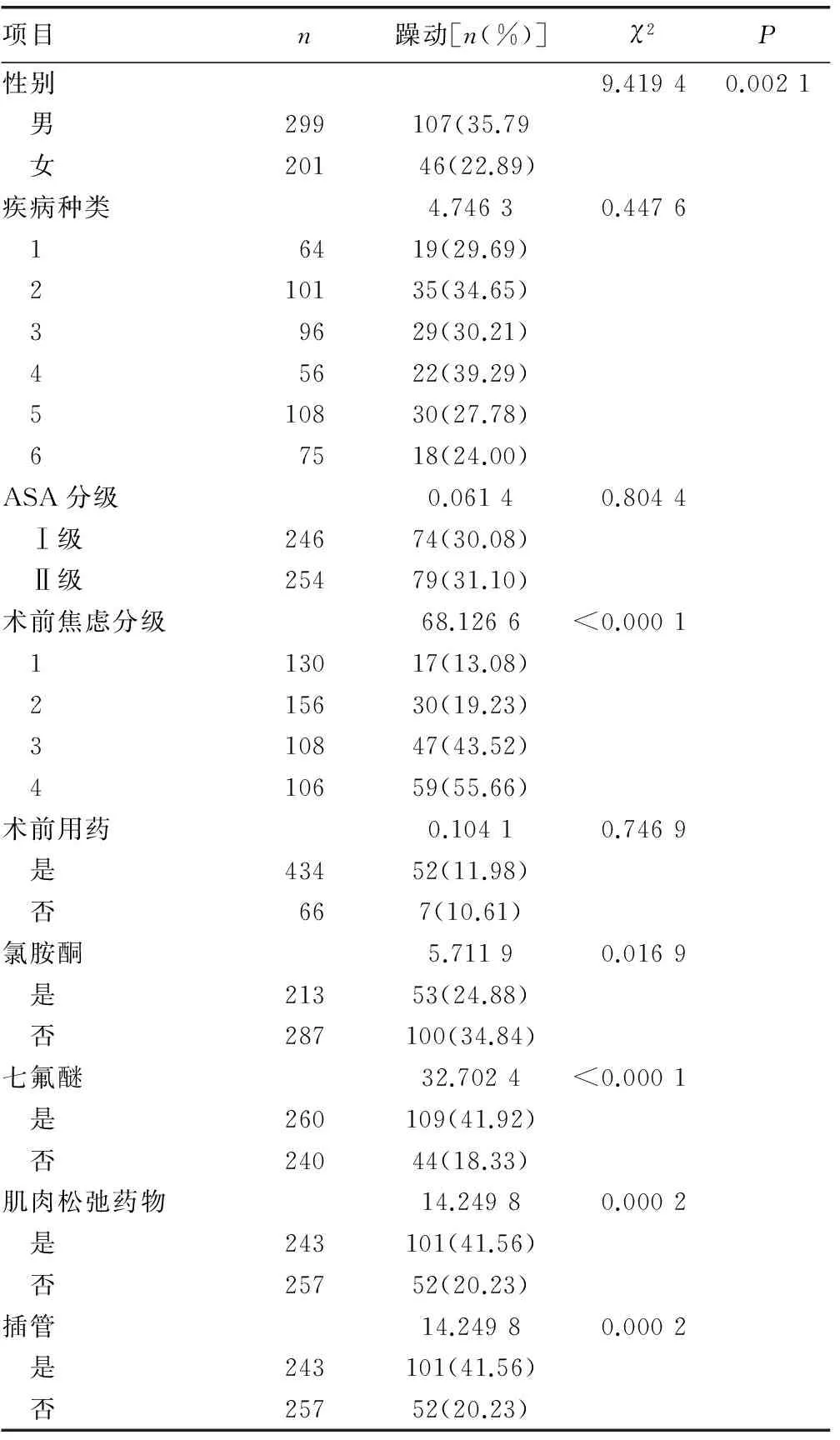
表3 两组患儿一般临床资料及麻醉相关资料的比较

表4 Logistic回归系数、标准误、OR值及95%可信区间及ROC值

续表4 Logistic回归系数、标准误、OR值及95%可信区间及ROC值
Logistic回归方程为log it(P)=-1.470 0-0.556 2y-0.780 9S+0.097 3kg+0.687 8An-0.445 5K+1.126 9Se+1.101 2I。
3 讨论
患儿术后躁动发生率较高,术后缺氧、伤口疼痛、心理恐惧、各种不适均可导致患儿在苏醒期躁动。可乐定于手术前使用可以明显减少术后躁动[2];静脉注射咪唑安定也可以减少术后躁动发生[3];咪唑安定经鼻滴入对术后躁动也有较好的抑制作用[4]。本研究表明在术前没有用这些药物和方法,患儿术后躁动发生率为30.6%,如果使用了这些药物和方法,有可能减少患儿术后躁动发生率。
七氟醚吸入麻醉有较高术后躁动发生率[5]。但七氟醚联合使用小剂量异丙酚1 mg/kg或芬太尼1 μg/kg可以减少术后躁动[6],麻醉前静脉注射安定或父母陪同安慰的方法对七氟醚麻醉引起术后苏醒期躁动有抑制作用[7]。本研究表明七氟醚麻醉后,其他研究因素保持不变的条件下,七氟醚吸入麻醉,躁动的发生率较非七氟醚麻醉组发生率提高3.086倍。
联合使用氯胺酮及异丙酚可以减少单独使用氯胺酮或者异丙酚的不良反应[8],小剂量氯胺酮加上异丙酚可以减少全凭异丙酚静脉麻醉患儿术后躁动[9],异丙酚静脉麻醉可减少七氟醚麻醉术后躁动发生率[10]。小剂量安定、异丙酚、小剂量芬太尼联合使用可减少术后躁动[11]。本研究也表明术前使用小剂量氯胺酮可有效抑制患儿麻醉后躁动发生率,其OR值为0.641。在其他影响因素不变时,本研究方法可以使麻醉手术后躁动发生率减少36%。
学前儿童较高术后躁动发生率(43.3%)是由于对父母依赖[12]。本研究还表明患儿性别、身高与患儿麻醉手术后躁动呈负相关性。这可能与年龄较大女性患儿较易交流,能较好适应麻醉手术后各种不适。本研究表明,排除其他影响因素下,容易焦虑儿童发生躁动概率是非焦虑儿童的1.989倍。另外,做气管插管患儿其OR值为3.008,这表明麻醉时气管插管患儿,更容易有不适感,特别是插管致喉头部位刺激,能增加躁动发生率。
ROC曲线下的面积反映诊断系统的准确性,理论上这一指标的取值范围为0.5~1,完全无价值的诊断为0.5,完善的诊断为1[13]。本例ROC值为0.850,说明本方程准确性较好。
[1]Bortone L,Ingelmo P,Grossi S,et al.Emergence agitation in preschool children:double-blind,randomized controlled trial comparing sevoflurane and isoflurane anesthesia[J].Paediatr Anaesth,2006,16(11):1138-1143.
[2]Heinmiller LJ,Nelson LB,Goldberg MB,et al.Clonidine premedication versus placebo:effects on postoperative agitation and recovery time in children undergoing strabismus surgery[J].J Pediatr Ophthalmol Strabismus,2013,50(3):150-154.
[3]Fagin A,Palmieri T,Greenhalgh D,et al.A comparison of dexmedetomidine and midazolam for sedation in severe pediatric burn injury[J].J Burn Care Res,2012,33(6):759-763.
[4]Akin A,Bayram A,Esmaoglu A,et al.Dexmedetomidine vs midazolam for premedication of pediatric patients undergoing anesthesia[J].Paediatr Anaesth,2012,22(9):871-876.
[5]Kim D,Doo AR,Lim H,et al.Effect of ketorolac on the prevention of emergence agitation in children after sevoflurane anesthesia[J].Korean J Anesthesiol,2013,64(3):240-245.
[6]Kim MS,Moon BE,Kim H,et al.Comparison of propofol and fentanyl administered at the end of anaesthesia for prevention of emergence agitation after sevoflurane anaesthesia in children[J].Br J Anaesth,2013,110(2):274-280.
[7]Zand F,Allahyary E,Hamidi AR.Postoperative agitation in preschool children following emergence from sevoflurane or halothane anesthesia:a randomized study on the forestalling effect of midazolam premedication versus parental presence at induction of anesthesia[J].Acta Anaesthesiol Taiwan,2011,49(3):96-99.
[8]Alletag MJ,Auerbach MA,Baum CR.Ketamine,propofol,and ketofol use for pediatric sedation[J].Pediatr Emerg Care,2012,28(12):1391-1395.
[9]Anghelescu DL,Rakes LC,Shearer JR,et al.Prevention of emergence agitation in seven children receiving low-dose ketamine and propofol total intravenous anesthesia[J].AANA J,2011,79(3):238-242.
[10]Key KL,Rich C,De Cristofaro C,et al.Use of propofol and emergence agitation in children:a literature review[J].AANA J,2010,78(6):468-473.
[11]Chen J,Li W,Hu X,et al.Emergence agitation after cataract surgery in children:a comparison of midazolam,propofol and ketamine[J].Paediatr Anaesth,2010,20(9):873-879.
[12]Fan H,Tao F,Wan HF,et al.A prospective cohort study of the risk factors of emergence agitation in pediatric after general anesthesia[J].Zhonghua Yi Xue Za Zhi,2012,92(17):1194-1197.
[13]汪海波,罗莉,吴为,等.SAS统计分析与应用从入门到精通[M].北京:人民邮电出版社,2013:439.
The incidence and risk factor for agitation after the general anesthesia from 500 pediatric patients
LiFaying,XuFeng△,ZhangXianlong
(DepartmentofAnaesthesiology,Huai′anFirstPeople′sHospitalAffiliatedtoNJMU,Huai′an,Jiangsu223300,China)
Objective To identify the incidence and risk factors that are associated with agitation after general anesthesia from 500 pediatric patients.Methods Data about any kinds of the index from 500 pediatric patients,ASA Ⅰand Ⅱ,receiving general anesthesia were recorded.such as the age,sex,weight,anxious before the anesthesia,kinds of the disease,class of ASA,kinds and dosage of the anesthesia drug,such as ketamine,propfol,sevoflurane,fentanyl,the intubation,length of anesthesia time,the recovery time and the agitation grade.According to the agitation grade,all the patients divided into two group,the agitation group and the non-agitation group.Logistic regression with a descending stepwise algorithm was performed to identify independent variables.The discriminative power of the Logistic regression model was checked with a receiver operating characteristic curve.Results Agitation meeting the predefined criteria occurred in 153 patients(30.6%).The Logistic analysis identified the following varables to be associated with agitation after the anesthesia:age,sex,weight,anxious before the anesthesia,the use of the ketamine and the sevoflurane,the intubation.The agitation correlation coefficients for the age,sex,and the use of the ketamine were negative,otherwise the weight,anxiety,the use of sevoflurane and the intubation were positive.The area of ROC was 0.850.Conclusion This study contributes to the identification of patients with a high risk for agitation after general anethesia.The index of the age,sex,weight,anxious before the anesthesia,the use of the ketamine and the sevoflurane,the intubation should be comprehensive evaluated.
pediatric;anesthesia;agitation;Logistic regression
李法印(1979-),主治医师,本科,主要从事临床麻醉镇痛机制研究。△
,Tel:13952346702;E-mail:xf169873@126.com。
10.3969/j.issn.1671-8348.2015.08.024
R614
A
1671-8348(2015)08-1082-03
2014-10-01
2014-12-20)
