Electroacupuncture combined with traction and tuina for lumber intervertebral disc herniation
2015-05-18HuangYu-bin,BianRong-min
Electroacupuncture combined with traction and tuina for lumber intervertebral disc herniation
Objective: To observe the effect of electroacupuncture (EA) combined with traction and modified oblique Ban-pulling manipulation on lumber intervertebral disc herniation (LIDH).
Acupuncture Therapy; Electroacupuncture; Traction; Tuina; Massage; Low Back Pain; Intervertebral Disc Displacement
Lumber Intervertebral disc Herniation (LIDH) is a degeneration or wear and tear of the lumbar intervertebral disc due to trauma or accumulation of stresses over time. During this process, rupture of the annulus fibrosus can cause bulging or herniation of the nucleus pulposus to irritate and compress the spinal nerve root, resulting in inflammation and impairment of neurotrophy and conduction as well as low back pain, sciatica and significant neurological deficits[1-3]. Severe LIDH can affect the patients’ quality of life in daily living and work. To investigate better treatment methods for LIDH, we’ve treated LIDH patients with electroacupuncture (EA) combined with traction and modified oblique Ban-pulling manipulation between April 2013and December 2013. The report is now presented as follows.
1 Clinical Data
1.1 Diagnostic criteria
This is based on the diagnostic criteria for LIDH stipulated in the Shanghai Diagnostic and Therapeutic Guidelines of Traditional Chinese Medicine[4]: a history of lumbar trauma, chronic strain or external contraction of cold-dampness; low back pain that radiates to the buttocks and lower limbs and aggravates by increased abdominal pressure (such as coughing or sneezing); scoliosis, absence of physiological spinal curvature, tenderness around the affected vertebrae that radiates downward and restricted lumbar movement; positive results of straight leg raise test and enhanced test, weakor absent knee and tendon reflex, weak dorsiflexion of the great toe or muscular atrophy in patients with a long duration; LIDH confirmed by X-ray, CT scan or MRI examination.
1.2 Inclusion criteria
Those who met the above diagnostic criteria; aged between 20 and 65 years; having a clear mind to complete the treatment independently; and those who were willing to participate in the study and signed the informed consent.
1.3 Exclusion criteria
Spinal or intra-canal tumor or tuberculosis; lumbar spinal stenosis, spondylolisthesis and severe osteoporosis; pregnant women; having other medical conditions that are not suitable for acupuncture; and those who received other therapies during the treatment.
1.4 Statistical method
The SPSS 13.0 version software was used for statistical analysis. The measurement data was expressed with mean ± standard deviation (x ±s). The t-test was used for intra-group comparison, analysis of variance for inter-group comparison, and Chi-square test for ratio comparison. A P value <0.05 indicates a statistical significance.
1.5 General materials
A total of 90 cases (44 males and 46 females) in the Traumatology Department in our hospital were included in the study. They are aged between 23 and 65 years. The LIDH duration lasted from 1 week to 32 months.
The 90 cases were randomly allocated into three groups (A, B and C) by their visit sequence, 30 in each group. There were no statistical significances among the three groups in differences of gender, age and duration (P > 0.05), indicating that the three groups were comparable (Table 1).
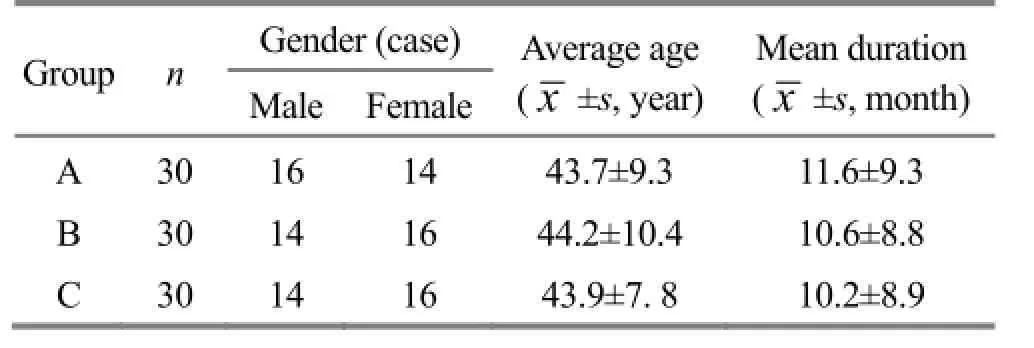
Table 1. Inter-group comparison of general materials
2 Treatment Methods
2.1 Group A
2.1.1 EA
Points: Four local points (1 cm lateral to the superior and inferior spinous processes of the affected intervertebral disc), Huantiao (GB 30), Juliao (GB 29), Ashi point [the most painful tender point on the line connecting Huantiao (GB 30) and Juliao (GB 29)]and Weizhong (BL 40)[3].
Method: The patient was asked to take a prone position to fully expose the treatment area. After routine sterilization, the aforementioned points were punctured using filiform needles of 0.30 mm in diameter and 75 mm in length. Upon arrival of qi, reducing manipulation by rotating, lifting and thrusting was used to cause local soreness and distension that radiate towards the buttocks and thighs, especially the three points in the buttocks. However, strong stimulation should be avoided to prevent the sciatic nerve from being injured. Then the KWD-8081 electric stimulator was connected, using continuous wave and tolerable intensity for 20 min. During retention of the needles, the TDP-CQ was used for lumbar irradiation.
2.1.2 Modified oblique Ban-pulling manipulation
Method: The patient was asked to take a side lying position (the affected side on top) with flexed hip and knee of the affected limb and natural extension of the healthy limb. Standing to face with the patient, the practitioner placed one palm on the front part of the shoulder joint and pressed against the posterolateral side of the affected hip bone using the medial side of the flexed elbow of the other hand; then shook the patient’s body back and forth using coordinated force and rotated the lumbar vertebra using opposing force (i.e., pulling the shoulder forward and downward and the buttocks backward and downward); released the force after continuous small-amplitude traction and torsion; after this, applied pulling and rotating to a maximum degree with obvious resistance, paused for a while and conducted a sudden rapid thrust to increase the lumbar range of motion by 5-10°, often coupled with a ‘crack’ sound (Figure 1).

Figure 1. Modified oblique Ban-pulling manipulation
2.1.3 Electronic traction The patient was asked to take a supine position on the traction bed and immobilize the chest, back and pelvis. The traction power was set (1/3-2/3 of the bodyweight) according to patients’ height, weight and gender, 20 min each time. The patient was then asked to rest on a hard mattress.
As for the treatment sequence, the patient was treated with EA first, followed by modified oblique Ban-pulling manipulation and traction. The treatment was done once a day. The therapeutic efficacy was observed after 10 treatments.
2.2 Group B
Patients in group B received same modified oblique Ban-pulling and electronic traction as group A (same method and course of treatment).
2.3 Group C
Patients in group C received same electronic traction as group A (same method and course of treatment).
3 Treatment Results
3.1 Measurements
The low back and leg pain was evaluated according to the Japanese Orthopedic Association (JOA) score rating system[5], including subjective symptoms (9 points), clinical signs (6 points), limitation in daily living (14 points). The JOA score ranged from 0 to 29. A lower score indicates a more severe disability. The improvement of lumbar function after treatment was evaluated by changes in JOA scores.
Improvement rate = (Post-treatment score - Pretreatment score) ÷ (29 - Pre-treatment score) × 100%.
3.2 Therapeutic efficacy criteria
The therapeutic efficacy was evaluated by change in JOA score.
Recovery: Improvement rate equal to 100%.
Marked effect: Improvement rate > 60% but<100%.
Improvement: Improvement rate ≥25% but ≤60%.
Failure: Improvement rate <25%.
3.3 Treatment outcome
3.3.1 Inter-group comparison of JOA scores before and after treatment
The analysis of variance has shown that there was no inter-group statistical significance in JOA score before treatment (P > 0.05); and there were statistical intra-group (P<0.01) and inter-group differences in JOA scores after treatment and 1 month after treatment (P < 0.05). This indicates that all three treatment protocols can improve low back and leg pain in LIDH patients and patients in group A obtained a better result (Table 2).
3.3.2 Inter-group comparison of total effective rate
The total effective rate in group A was 96.7%, versus 90.0% in group B and 70.0% in group C, showing a significantly better effect in group A than the other two groups (both P<0.01), (Table 3).

Table 2. Inter-group comparison of JOA score (x ±s, point)

Table 3. Inter-group comparison of clinical efficacy (case)
4 Discussion
Acupuncture, tuina and traction are all effective for LIDH. Traction of the pelvic can increase the tension of paravertebral muscles, ligaments and annulus fibrosus, widen the intervertebral space, and alleviate stress to the disc tissue. Furthermore, the elasticity of the tightened posterior longitudinal ligament can force the herniated disc to retract or change the relative position between the herniated disc and nerve root, thus alleviating or relieving compression of the herniated disc to the nerve root. Modified oblique Ban-pulling manipulation combines oblique Ban-pulling by rotation and stretching. In case of unstable spine, this manipulation helps to slightly shift facet joints on one side and change the relative position betweenherniated disc and nerve root, relieve mechanical compression to the nerve root, relax the adhesion, restore intervertebral balance and therefore alleviate symptoms[6].
LIDH manifests as congestive edema of intra-canal nerve root due to mechanical compression and irritation. The inflammation causes pain that radiates along the nerve and result in low back and leg pain. Pain can cause local muscle spasm. Persistent spasm, in turn, causes microcirculation disorder, releases inflammatory substances and aggravates the pain. Consequently, the treatment principles are to improve local microcirculation, relieve muscle spasm, relax adhesion, resolve congestive edema of the nerve root and thus ease pain.
Four local points in this study are full of nerves and blood vessels. With deep puncture, needles can almost reach the nerve root. It’s believed that receptors of acupuncture analgesia lie in the anterior and posterior branches of the spinal nerve root, spinal ganglion, sympathetic ganglion, gray and white communicating branches of the sympathetic trunk and other neurovascular tissues. Spinal ganglion is considered as regulator of the low back and leg pain because it can synthesize and release multiple neuropeptides[7-9]. Some scholars believe that EA can increase endorphin release in the brain to exert immuno-regulatory effect. In addition, stimulating lumbar nerves can conduct impulses to the cerebral cortex, resulting in transmarginal inhibition on pathologic reaction of herniated disc. Subsequently, this can improve microcirculation surrounding the nerve root and alleviate aseptic inflammation[10]. Needling this point can improve microcirculation in localized area, alleviate spasm, resolve edema and relieve clinical symptoms. Of three points in the buttocks, needling Huantiao (GB 30) can alleviate sciatica and release gluteal muscle spasm; needling Juliao (GB 29) can release piriform muscle spasm, resolve local inflammatory edema and relieve compression and irritation to the nerves and blood vessels[11]. Ashi point in the buttocks is similar to trigger points in modern medicine, referring to palpable nodules in taut bands of muscle fibers and hyperirritable spots in the fascia surrounding the skeletal muscle[12]. Needling this point can increase localized blood circulation, release muscle spasm and alleviate or relieve symptoms. Needling the three buttock points can relax tendons, unblock meridians and alleviate pain. As the old saying goes, treating lumbar-back problems by puncturing Weizhong (BL 40), which is a distal point along the meridian, needling this point can regulate qi of the Bladder Meridian[13-15].
The findings of this observation have shown that the total effective rate in group A (treated with EA combined with traction and modified oblique Ban-pulling manipulation) was higher than that in the other two groups, indicating that a more comprehensive therapy can obtain a better efficacy.
Conflict of Interest
The authors declared that there was no potential conflict of interest.
Acknowledgments
This work was supported by Community Health Service Center, Changjiang Road, Baoshan District, Shanghai.
Statement of Informed Consent
All of the patients in the study signed the informed consent.
Received: 16 August 2014/Accepted: 20 October 2014
[1]He BZ. Clinical observation and mechanism on reduction by rotation for lumbar intervertebral disc herniation. Zhongguo Zhongyi Gushangke Zazhi, 2006, 14(suppl): 41-42.
[2]Xiao H, Xiao F, Guo XQ. The clinical efficacy of acupuncture and chiropractic techniques in the treatment of lumbar disc herniation. Zhongguo Yiliao Qianyan, 2013, 8(17): 75-76.
[3]Liu J. Effect observation on acupuncture for lumbar intervertebral disc herniation. Zhongguo Yiyao Zhinan, 2013, 28(10): 212.
[4]Shanghai Municipal Health Bureau. Shanghai Diagnostic and Therapeutic Guidelines of Traditional Chinese Medicine. 2nd Edition. Shanghai: Publishing House of Shanghai University of Traditional Chinese Medicine, 2003: 402.
[5]Fukui M, Chiba K, Kawakami M, Kikuchi S, Konno S, Miyamoto M, Seichi A, Shimamura T, Shirado O, Taguchi T, Takahashi K, Takeshita K, Tani T, Toyama Y, Wada E, Yonenobu K, Tanaka T, Hirota Y. JOA back pain evaluation questionnaire: initial report. J Orthop Sci, 2007, 12(5): 443-450.
[6]Gu F, Fang M. To study normalized manipulation and quantificated curative effect for treating Lumbar Disc herniation with massage therapy. Jing Yao Tong Zazhi, 2010, 31(1): 9-11.
[7]Huang SR, Shi YY, Zhan HS. Dynamic control observation on the clinical analgesic effect of different points electroacupuncture on lumbar intervertebral disc herniation. Zhongguo Tengtong Yixue Zazhi, 2006, 12(4): 203-205, 209.
[8]Zhang DQ, Zhao YH, Li HN, Zhong JB, Liu J, Yu R.Effect of electroacupuncture on Oswestry disability indexes in patients with lumbar intervertebral disc herniation. Zhongyi Yanjiu, 2013, 26(11): 56-58.
[9]Ao JB, Chen J, Mu JP, Peng L, Cheng JM, Zhou ZY, Wang J. Clinical observation on electroacupuncture at Jiaji (EX-B 2) points combined with 3-D traction for lumbar intervertebral disc herniation in 40 cases. Zhongguo Zhongyi Jizheng, 2008, 17(5): 626-627.
[10]Huang Y. Clinical research overview on lumbar disc herniation based on caller needle treatment. Hunan Zhongyiyao Daxue Xuebao, 2014, 16(1): 109-112.
[11]Zhu JH, Chen HY, Chen JY. Treating 30 cases of backbone of sciatica by hip three-needle-based acupuncture. Zhongyi Linchuang Yanjiu, 2011, 3(5): 78-79.
[12]Wang YS, Yao M. Research advance in myofascial trigger points. Harbin Yike Daxue Xuebao, 2001, 35(3): 230-231.
[13]Jiang JJ. Clinical observations on point Weizhong pricking bloodletting treatment for lumbar intervertebral disc herniation. Shanghai Zhenjiu Zazhi, 2013, 32(12): 1037-1038.
[14]Bi HJ, He YY. General research situation of the classic saying of treating lumbar-back problems by puncturing Weizhong (BL 40). Hebei Zhongyi, 2013, 35(4): 615-617.
[15]Yang L, Huang QF, Wu HG, Liu XX, Ding GH, Ma XP, Feng XM, Dou CZ. Analysis of the frequency of clinical acupoint use based on ‘Traditional Chinese Medical Acupuncture-moxibustion Information Databank’. J Acupunct Tuina Sci, 2014, 12(2): 80-88.
Translator: Han Chou-ping (韩丑萍)
电针结合牵引及推拿治疗腰椎间盘突出症
Huang Yu-bin (黄郁斌), Bian Rong-min (卞蓉民)
Community Health Service Center, Changjiang Road, Baoshan District, Shanghai, Shanghai 200431, China
目的:观察电针配合牵引及改良斜扳法治疗腰椎间盘突出症(lumber intervertebral disc herniation, LIDH)的临床疗效。方法:将 90 例符合诊断标准的患者随机分为 3 组,每组 30 例。A 组予以电针、牵引及改良斜扳法推拿治疗;B组予以与A组相同的牵引及推拿治疗;C组予以与其他两组相同的牵引治疗。治疗结束后根据日本骨科协会(Japanese Orthopedic Association, JOA)的评估分数评价疗效。结果:治疗后及随访 1 月后,3 组 JOA 评分均较本组治疗前有改善(均 P<0.01)。A 组总有效率为 96.7%,B 组和 C 组分别为 90.0%和 70.0%,A 组总有效率明显优于其他两组(P<0.01)。结论:电针配合牵引及改良斜扳法可提高腰椎间盘突出症的疗效,优于单纯牵引和牵引配合改良斜扳法。
针刺疗法;电针;牵引;推拿;按摩;腰痛;椎间盘移位
R246.2
A
Author: Huang Yu-bin, bachelor, attending physician. E-mail: 1732098900@qq.com
Huang YB, Bian RM. Electroacupuncture combined with traction and tuina for lumber intervertebral disc herniation. J Acupunct Tuina Sci, 2015, 13 (1): 27-31
10.1007/s11726-015-0818-x
Methods: A total of 90 eligible cases were randomly allocated into three groups, 30 in each group. Cases in group A were treated with EA, traction and tuina of modified oblique Ban-pulling manipulation; cases in group B were treated with traction and tuina (same as group A); and cases in group C were treated with traction alone (same as the other two groups). Then the therapeutic efficacies in the three groups were evaluated using the Japanese Orthopedic Association (JOA) score rating system.
Results: The results after treatment and 1-month follow up showed that JOA scores in all three groups were improved (P<0.01); the total effective rate in Group A was 96.7%, versus 90.0% in group B and 70.0% in group C, showing a significantly better effect than the other two groups (P<0.01).
Conclusion: EA combined with traction and modified oblique Ban-pulling manipulation can obtain better effect than traction alone and traction combined with modified oblique Ban-pulling manipulation for LIDH.
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- 复式针刺补泻对臀大肌挛缩术后髋关节和膝关节屈伸角度的影响
- 电针对脑缺血再灌注模型大鼠血清白介素的影响
- 隔药灸天枢和气海对慢性炎性内脏痛大鼠痛行为和痛情绪的影响
- Clinical observation on warm needling in canicular days for knee osteoarthritis
- Observation on clinical effect of electroacupuncture plus pricking-cupping bloodletting therapy for herpes zoster
- Observation on clinical effect of acupuncture plus Zi Shen Tiao Gan Decoction for perimenopausal insomnia