血管紧张素转换酶基因多态性与儿童原发性肾病综合征关联性的系统评价和Meta分析
2015-05-04谢敏娟徐石张傅小一
谢敏娟 徐石张 傅小一
血管紧张素转换酶基因多态性与儿童原发性肾病综合征关联性的系统评价和Meta分析
谢敏娟1徐石张2傅小一1
目的 系统评价血管紧张素转换酶(ACE)基因多态性与儿童原发性肾病综合征(PNS)的关联。方法 计算机检索PubMed、EMBASE、Wiley Online Library、Cochrane图书馆、Science Citation Index、Google Scholar、中国期刊全文数据库、万方数据库、中国生物医学文献数据库和维普数据库,检索时间为2000年1月1日至2014年5月31日,纳入ACE基因多态性与儿童PNS关联的病例对照研究。提取PNS组和对照组基因型和等位基因频率,计算各纳入文献对照组Hardy-Weinberg平衡(HWE),并进行文献偏倚评价。采用Stata 12.0软件,对PNS组和对照组ACE基因DD、DI、II基因型和D、I等位基因频率的差异行Meta分析。结果 14篇文献进入Meta分析,共纳入2 849例研究对象,其中PNS组1 264例,对照组1 585例。14篇文献偏倚风险较大。①D等位基因频率PNS组高于对照组(OR=1.277,95%CI 1.080~1.509,P=0.004);I等位基因频率PNS组低于对照组(OR=0.811,95%CI 0.738~0.892,P<0.001)。②DD基因型频率PNS组高于对照组(OR=1.505,95%CI 1.136~1.994,P=0.004);II基因型频率PNS组低于对照组(OR=0.746,95%CI 0.634~0.877,P<0.001);DI基因型频率PNS组与对照组差异无统计学意义(OR=0.932,95%CI 0.805~1.079,P=0.347)。③6篇文献对照组不符合HWE,剔除后8篇文献行敏感性分析,结果无明显变化;④DD基因型和D等位基因的文献间具有异质性,对照人群的来源、种族可解释部分的异质性,HWE与否不是异质性的原因。结论ACE基因DD基因型和D等位基因与儿童PNS的关联性不确定,如果有关联,强度可能较低。
血管紧张素转换酶; 基因多态性; 儿童; 肾病综合征; Meta分析
随着分子生物学技术的广泛应用,某些与原发性肾病综合征(PNS)发病相关的致病基因陆续被发现,其中包括较为常见的血管紧张素转换酶(ACE)基因[1,2]。有研究发现,ACE基因的第16内含子中存在287 bp片段的缺失(D)与插入(I),主要表现为缺失纯合子DD,并能影响血液中ACE水平[3,4]。之后多项研究发现ACE基因的D或I等位基因与多种肾脏病(如糖尿病肾病、IgA肾病)存在关联[5~7]。ACE基因多态性与PNS是否存在联系,目前仍无明确结论。Zhou等[8,9]曾对ACE基因多态性与儿童PNS的关联性行系统评价,但该研究未能对不同种族ACE基因多态性与PNS的关联性进行分析,尤其缺乏中国儿童PNS的数据。本文在已发表相关Meta分析的基础上,进一步检索和纳入中国PNS患儿的文献,探讨ACE基因多态性与PNS的关联性。
1 方法
1.1 文献纳入标准 ①ACE基因与PNS关联性的病例对照研究;②文献中有关于PNS诊断标准的描述;③PNS组年龄<18岁,对照组为健康成人或儿童;④采用PCR技术行ACE基因检测,PCR引物序列根据Rigat等[3]采用的ACE基因序列设计;⑤文献中提供了两组ACE各基因型或等位基因的例数;⑦中文和英文文献。
1.2 文献排除标准 重复发表的文献。
1.3 文献检索策略
1.3.1 数据库 计算机检索PubMed、EMBASE、Wiley Online Library、Cochrane图书馆、Science Citation Index、Google Scholar、中国期刊全文数据库、万方数据库、中国生物医学文献数据库和维普数据库。检索起止时间均为2000年1月至2014年5月。并回溯检索到相关文献的参考文献。
1.3.2 检索式 中文检索词:血管紧张素、血管紧张素转换酶、基因、多态性、儿童、小儿、肾病综合征等;英文检索词:angiotensin converting enzyme、ACE、nephrotic syndrome、NS、gene、polymorphism、childen、pediatric、idiopathic。以PubMed数据库为例,英文检索式:“angiotensin converting enzyme” (MeSH) OR pediatric (MeSH) OR “nephritic syndrome” (MeSH);以CBM数据库为例,中文检索式:血管紧张素转换酶 AND 儿童 AND 肾病综合征。
1.4 文献筛选、资料提取和偏倚评价 由谢敏娟、徐石张完成,如遇分歧由傅小一决定。
1.4.1 文献筛选和资料提取 阅读文题和摘要排除明显不相关的文献,对可能符合纳入标准的文献阅读全文决定是否纳入。提取项目包括:第一作者、发表时间、国家、语种、对照人群类型、样本量、样本来源、实验方法、PNS组和对照组ACE各基因型(DD、DI、II)的例数和等位基因的频数。对纳入文献对照组行Hardy-Weinberg平衡(HWE)检验。

1.5 统计学分析 采用Stata 12.0软件行Meta分析,采用比值比(OR)作为效应量行Meta分析。行文献间异质性检验,P<0.1为文献间存在统计学异质性,采用随机效应模型;P≥0.1为文献间具同质性,采用固定效应模型合并结果。对于存在显著统计学异质性的文献,采用亚组分析和回归分析行异质性原因分析。发表偏倚检验采用漏斗图和Begg检验。P<0.05为差异有统计学意义。
2 结果
2.1 文献检索结果 依据本文文献检索策略获得270篇文献,14篇文献[10~23]符合纳入和排除标准进入本文系统评价(图1)。14篇文献共纳入2 849例研究对象,其中PNS组为1 264例,对照组为1 585例。文献[12~15]以健康成人为对照组,余文献以健康儿童作为对照组;中国人群的研究7篇[17~23]。纳入14篇文献的一般情况和ACE基因型、等位基因数据见表1。
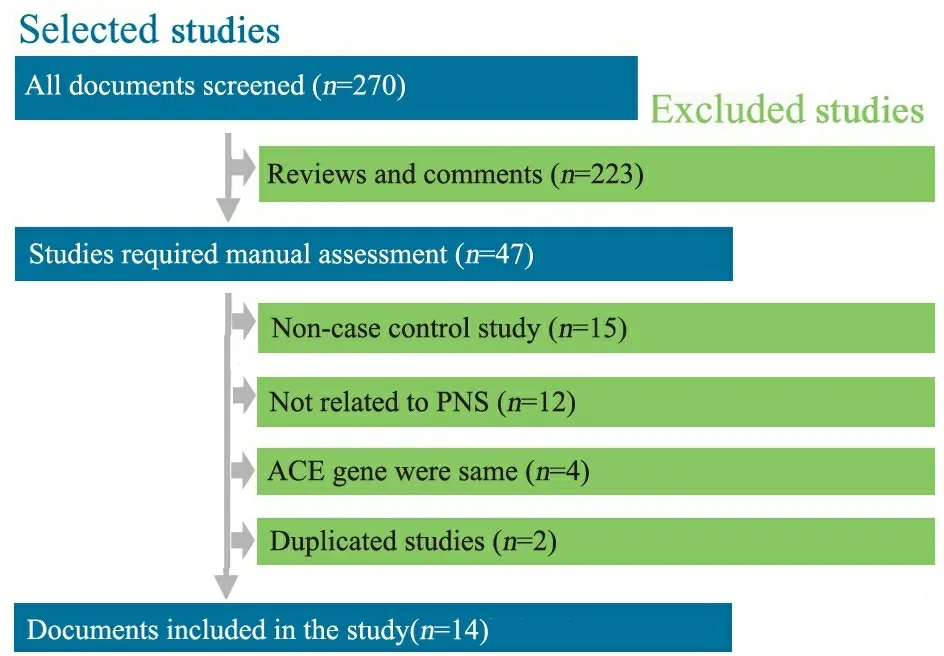
图1 文献筛选流程图
Fig 1 Flow chart of aricle screening and selection process
2.2 文献偏倚风险评价 图2显示,14篇文献条目1、4、6、8~10、12~14符合率为0,条目2、3符合率为92.9%,条目7的符合率为57.1%,条目5的符合率为21.4%,条目11的符合率为14.3%。
2.3 发表偏倚 对14篇纳入文献的DD基因型行发表偏倚检验,漏斗图对称(图3),Begg检验P=0.743,提示发表偏倚可能性不大。
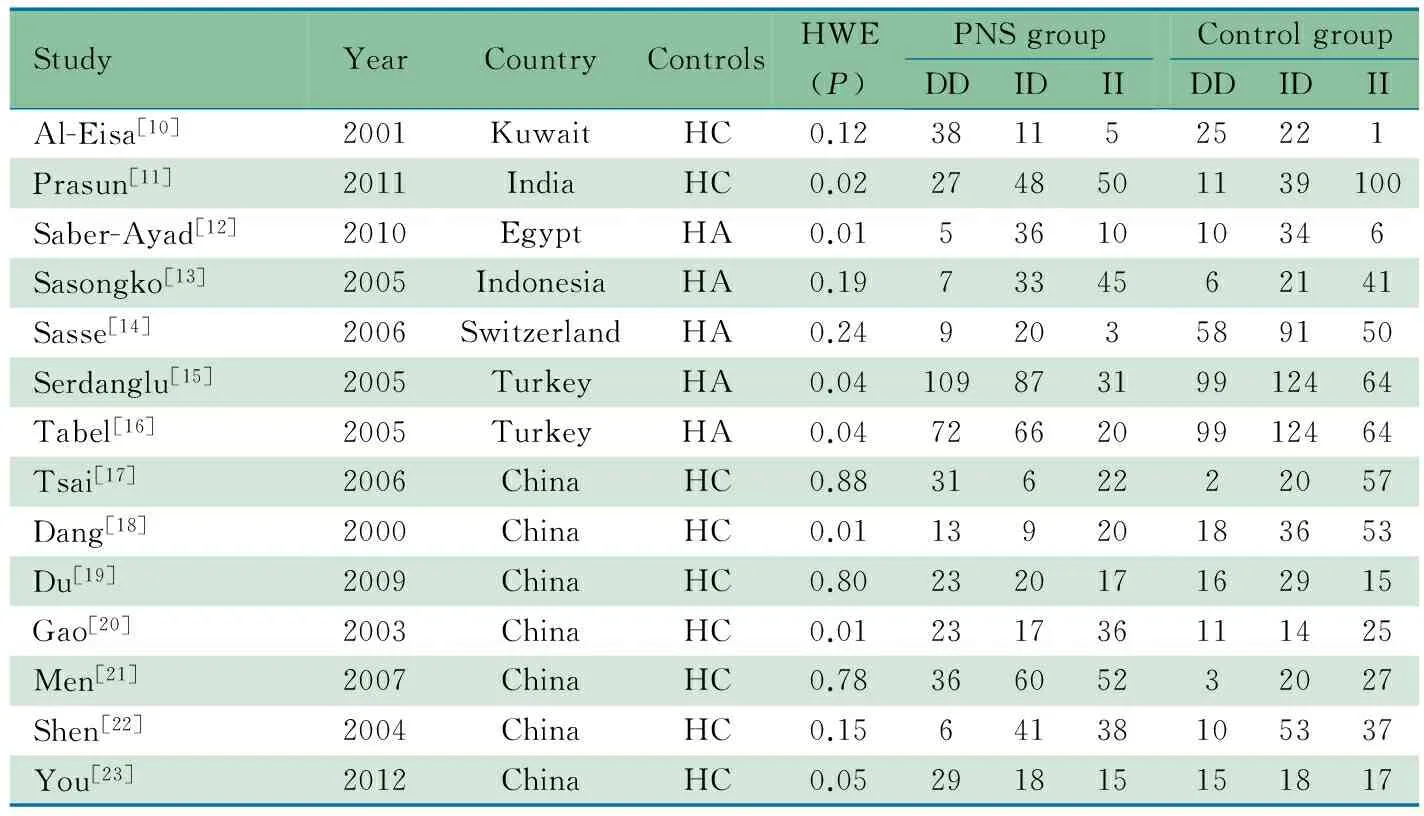
表1 纳入14篇文献的基本情况(n)
Notes HWE: Hardy-Weinberg equilibrium; HC: healthy children; HA: healthy adult
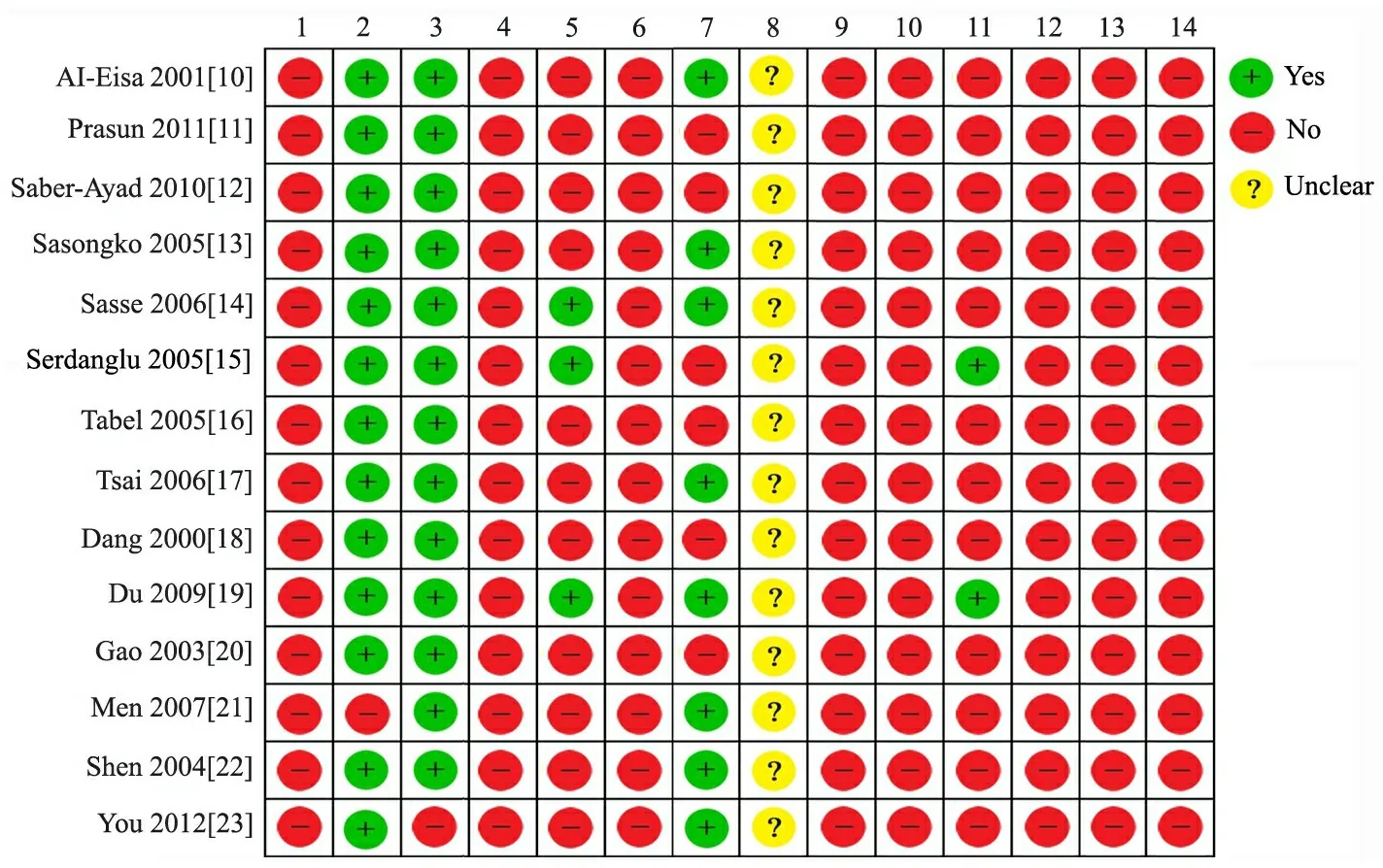
图2 纳入14篇文献的偏倚风险评价结果
Fig 2 Quality of 14 included studies
Notes 1:power;2:controls characterization;3:case characterization;4: LD exploration;5:polymorphism identification;6:genotyping error check;7:Hardy-Weinberg equilibrium;8: blinding;9:multiple testing ;10:covariate adjusment;11:risks;12:population stratification adjustment;13:replication;14:functional study
2.4 Meta分析结果
2.4.1 D和I等位基因与PNS的关联性 报道D等位基因文献的异质性检验I2=61.2%,有统计学异质性,采用随机效应模型合并结果。Meta分析结果显示,D等位基因频率PNS组高于对照组,OR=1.277,95%CI 1.080~1.509,P=0.004(图4)。
报道I等位基因文献的异质性检验I2=8.5%,无统计学异质性,采用固定效应模型合并结果。Meta分析结果显示,I等位基因频率PNS组低于对照组,OR=0.811,95%CI 0.738~0.892,P<0.001(图4)。
2.4.2 不同基因型与PNS的关联性 报道DD基因型文献间存在统计学异质性(P=0.013,I2=51.6%),采用随机效应模型合并结果,Meta分析结果显示,DD基因型频率PNS组高于对照组,OR=1.505,95%CI 1.136~1.994,P=0.004(图5) 。

图3 DD基因型发表偏倚的漏斗图
Fig 3Funnel plot of D allele
报道II和DI基因型文献间具同质性(I2分别为18.8%和7.6%),固定效应模型的Meta分析结果显示,II基因型频率PNS组低于对照组,OR=0.746,95%CI 0.634~0.877,P<0.001(图5),DI基因型频率PNS组与对照组差异无统计学意义,OR=0.932,95%CI 0.805~1.079,P=0.347(图5,6)。
2.5 敏感性分析 本文6篇文献对照组不符合HWE,剔除后8篇文献行敏感性分析,Meta分析结果显示,D等位基因频率PNS组高于对照组,OR=1.521,95%CI: 1.273~1.820;DD基因型频率PNS组亦高于对照组,OR=2.083,95%CI:1.542~2.805(表3),与原结果相比无明显变化。
2.6 异质性原因分析 DD基因型和D等位基因文献间具显著异质性,以对照人群来源、国家、HWE行异质性原因分析,表3显示,DD基因型非中国人群、成人对照的文献间无统计学异质性,D等位基因成人对照的文献间无统计学异质性。HWE与否不是异质性的原因。
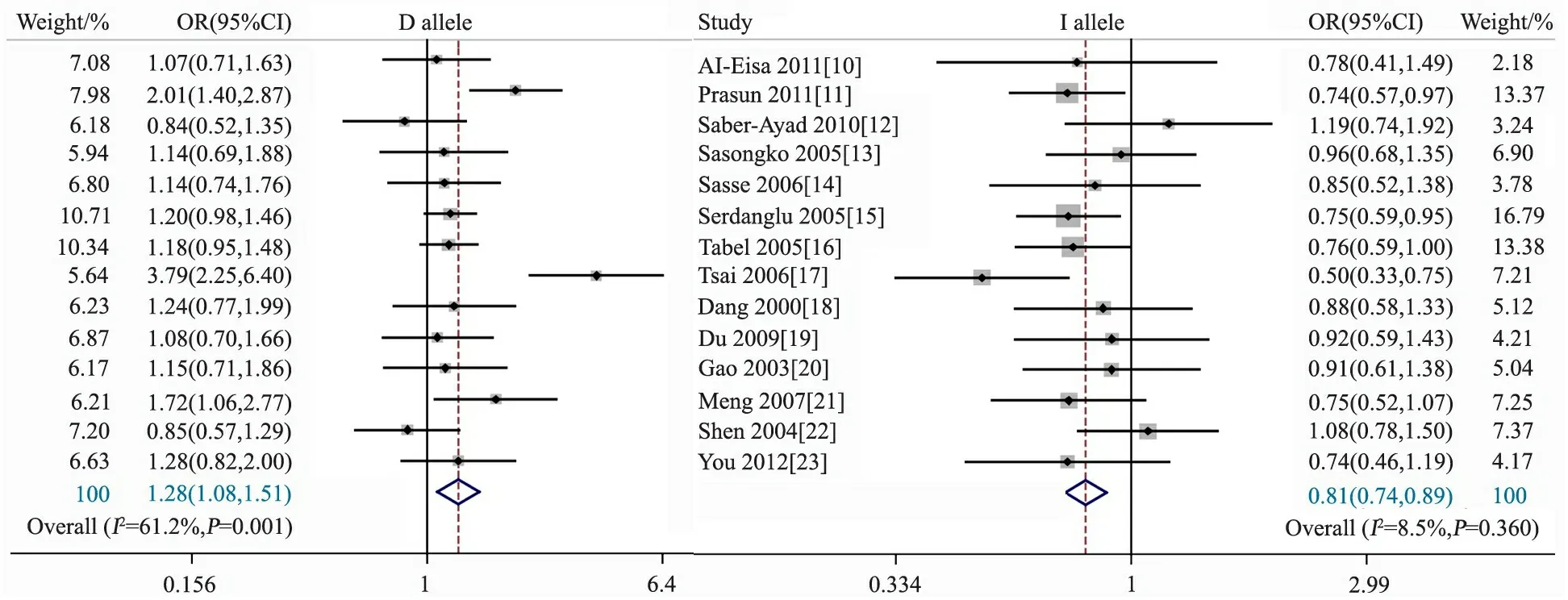
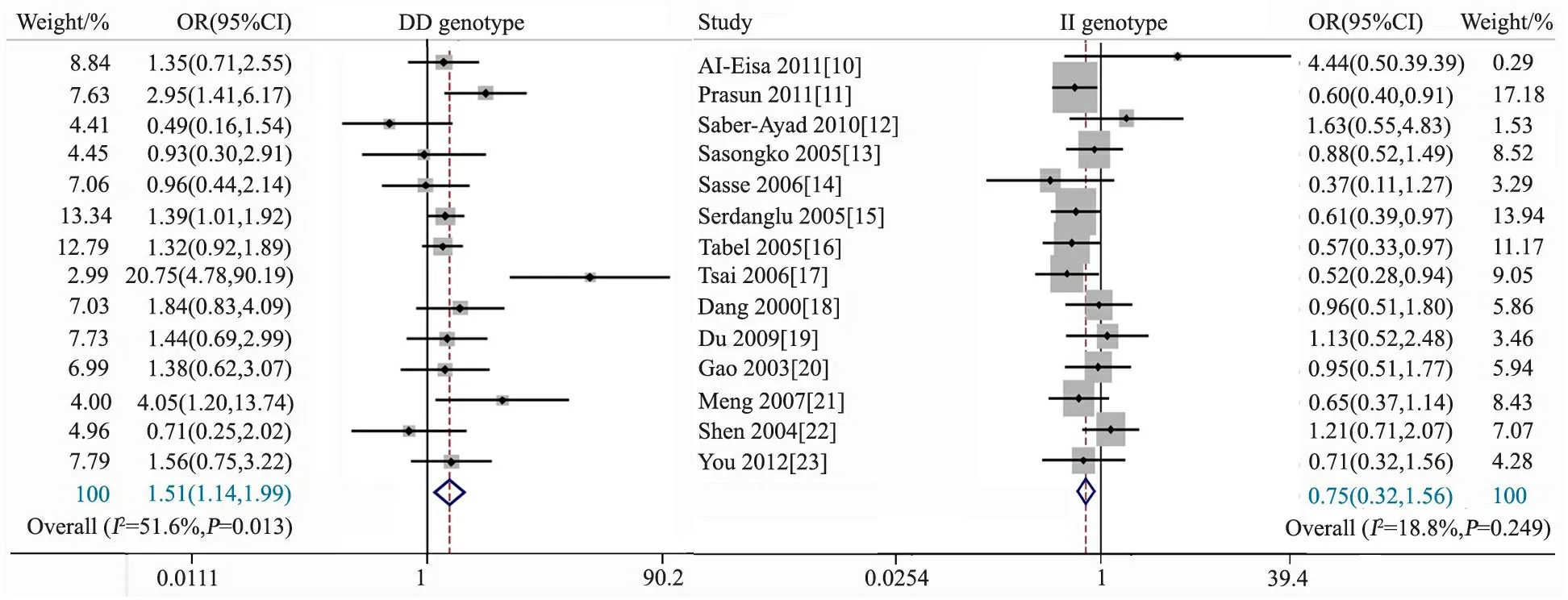
图4 D、I等位基因与PNS关联性的Meta分析
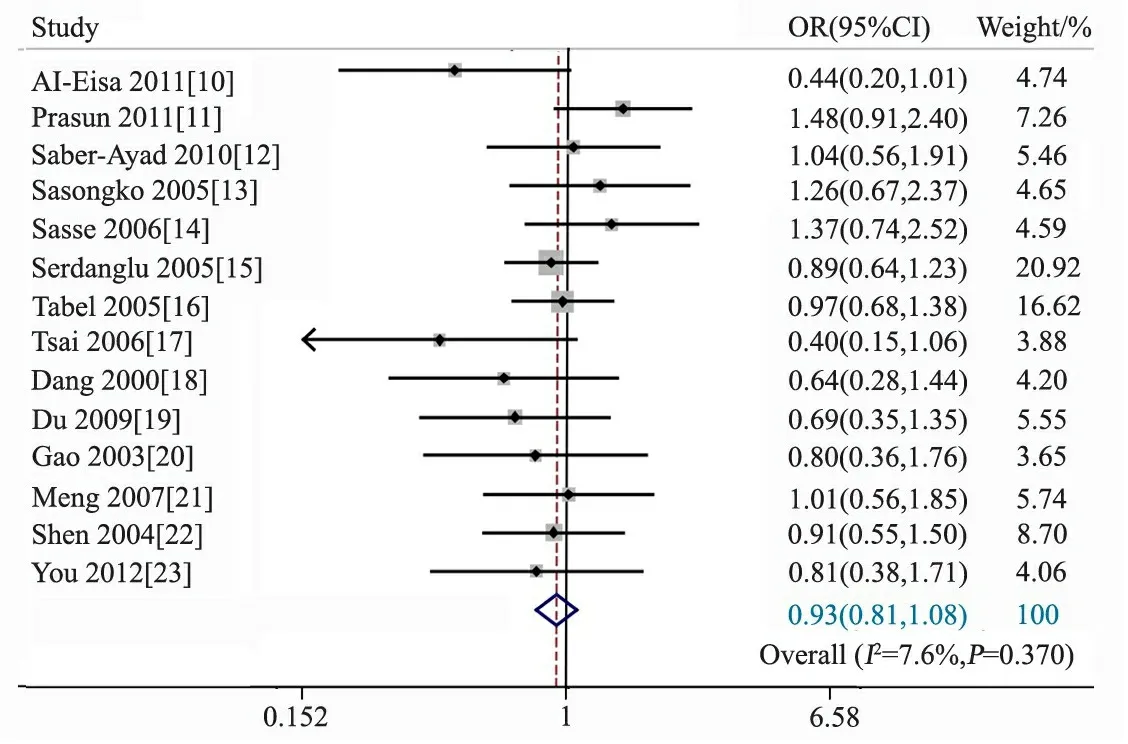
图5 DD、II基因型与PNS关联性的Meta分析
图6 DI基因型与PNS关联性的Meta分析
Fig 6 Meta analysis of relationship between DI genotype and PNS
3 讨论
本文Meta分析纳入14篇ACE基因与儿童PNS的遗传关联性研究,行14个条目的文献质量评价显示,9/14个条目的符合率为0,仅2个条目的符合率>90%,2个条目的符合率<25%,且有6篇文献对照组不符合HWE,提示本文Meta分析纳入的文献具有局限性。14篇文献的发表偏倚可能性不大。本Meta分析的证据强度低。
Lee等研究发现,42%的DD基因型患者进展为终末期肾病(ESRD),而在II基因型中仅有25%的患者最终发展为ESRD[24]。Frishberg等[25]研究显示,近50%携带D等位基因的患者随访过程中出现肾功能损害,II基因型者肾功能均正常。Luther等发现2/21例基因型II患者出现肾功能损害,50例携带等位基因D的患者中,超过60%出现肾功能损害[26]。存在等位基因D的患儿更易进展为局灶性节段性肾小球硬化[24,27],提示ACE基因多态性可能与PNS相关。
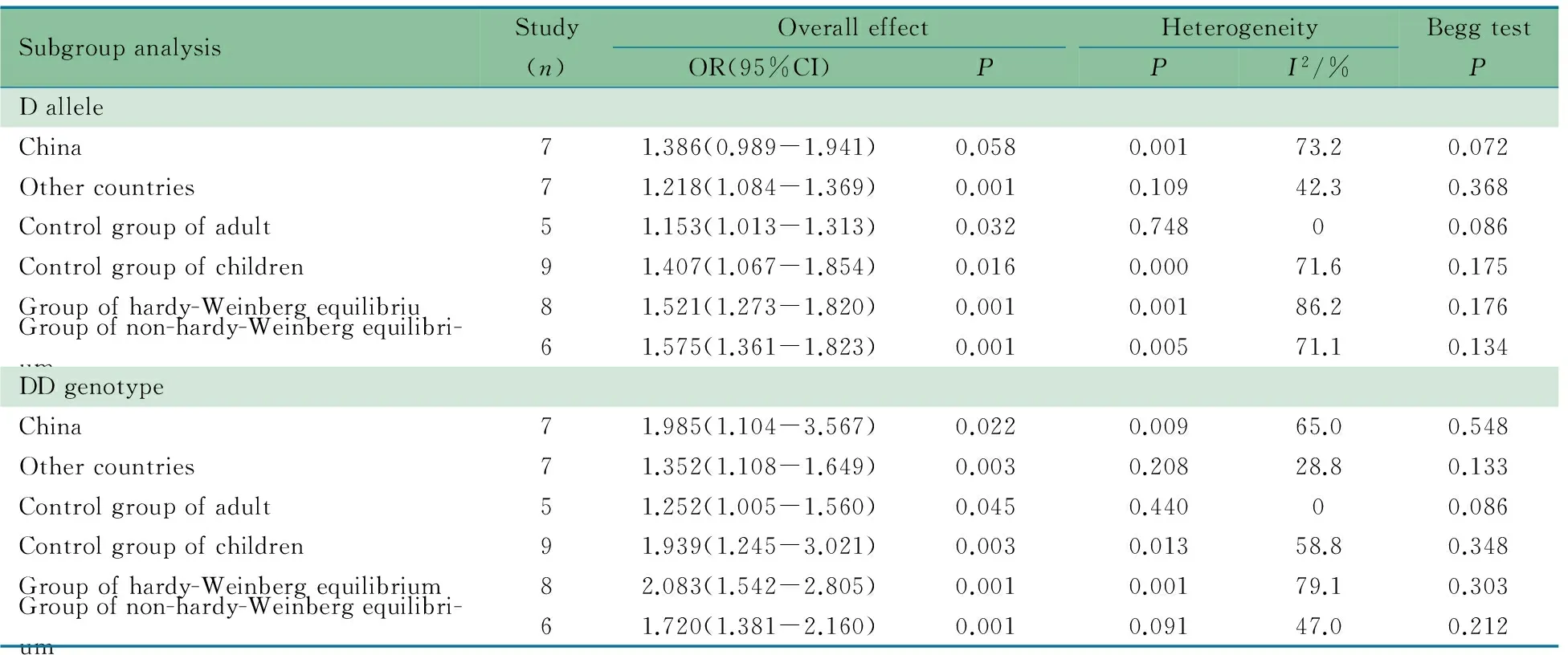
表3 等位基因D与基因型DD的亚组分析
本文ACE基因多态性的Meta分析结果提示, DD基因型和D等位基因与PNS的发生存在统计学关联,但文献间存在统计学异质性,以对照人群来源、国家行亚组分析,能部分解释异质性的来源。同时本文纳入的14篇文献中有6篇(42.9%)对照组不符合HWE,提示ACE基因可能不是一个特异性的PNS相关的基因,异质性来源与HWE无关,进一步对HWE或非HWE文献的敏感性分析显示,结果无明显变化。
本文Meta分析结果效应值的95%CI下限接近无效值1,行亚组分析后更为明显,特别是中国人群DD基因型与PNS的关联性差异无统计学意义,结果存在显著的不精确性,提示ACE基因DD基因型和D等位基因与儿童PNS的关联性不确定,如果有关联,强度可能较低。
[1]Mishra OP, Gupta AK, Prasad R, et al. Antioxidant status of children with idiopathic nephrotic syndrome. Pediatr Nephrol, 2011, 26(2): 251-256
[2]Oktem F, Sirin A, Bilge I, et al. ACE I/D gene polymorphism in primary FSGS and steroid-sensitive nephrotic syndrome. Pediatr Nephrol, 2004, 19(4): 384-389
[3]Rigat B, Hubert C, Alhenc-Gelas F, et al. An insertion/deletion polymorphism in the angiotensin I-converting enzyme gene accounting for half the variance of serum enzyme levels. J Clin Invest, 1990, 86(4): 1343-1346
[4]Costerousse O, Alledgrini J, Lopez M, et al. Angiotensin I converting enzyme in human circulating mononuclear cells: genetic polymorphism of expression in T-lymphocytes. Biochem J, 1993, 290(1): 33-40
[5]Arfa I, Abid A, Nouira S, et al. Lack of association between the angiotensin-converting enzyme gene (I/D) polymorphism and diabetic nephropathy in Tunisian type 2 diabetic patients. J Renin Angiotensin Aldosterone Syst, 2008, 9(1): 32-36
[6]Woo KT, Lau YK, Chan CM, et al. Angiotensin-converting enzyme inhibitor versus angiotensin 2 receptor antagonist therapy and the influence of angiotensin-converting enzyme gene polymorphism in IgA nephritis. Ann Acad Med Singapore, 2008, 37(5):372-376
[7]Colucci JA, Arita DY, Cunha TS, et al. Renin-angiotensin system may trigger kidney damage in NOD mice. J Renin Angiotensin Aldosterone Syst, 2011, 12(1): 15-22
[8]Zhou TB, Qin YH, Su LN, et al. ACE I/D gene polymorphism can't predict the steroid responsiveness in Asian children with idiopathicnephrotic syndrome: a meta-analysis. PLoS One, 2011, 6(5): e19599
[9]Zhou TB, Ou C, Qin YH, et al. Association of angiotensin converting enzyme insertion/deletion gene polymorphism with idiopathicnephrotic syndrome susceptibility in children: a meta-analysis. J Renin Angiotensin Aldosterone Syst, 2011, 12(4): 601-610
[10]Al-Eisa A, Haider MZ, Srivastva BS. Angiotensin converting enzyme gene insertion/deletion polymorphism in idiopathic nephrotic syndrome in Kuwaiti Arab children. Scand J Urol Nephrol, 2001, 35(3): 239-242
[11]Prasun P, Prasad N, Tripathi G, et al. Association of angiotensin-converting enzyme gene I/D polymorphism with steroid responsiveness in childhood nephrotic syndrome. Indian J Nephrol, 2011, 21(1): 26-29
[12]Saber-Ayad M, Sabry S, Abdel-Latif I, et al. Effect of angiotensin-converting enzyme gene insertion/deletion polymorphism on steroid resistance in Egyptian children with idiopathic nephrotic syndrome. J Renin Angiotensin Aldosterone Syst, 2010, 11(2): 111-118
[13]Sasongko TH, Sadewa AH, Kusuma PA, et al. ACE gene polymorphism in children with nephrotic syndrome in the Indonesian population. Kobe J Med Sci, 2005, 51(3): 41-47
[14]Sasse B, Hailemariam S, Wuthrich RP, et al. Angiotensin converting enzyme gene polymorphisms do not predict the course of idiopathic nephrotic syndrome in Swiss children. Nephrology (Carlton), 2006, 11(6): 538-541
[15]Serdaroglu E, Mir S, Berdeli A, et al. ACE gene insertion/deletion polymorphism in childhood idiopathic nephrotic syndrome. Pediatr Nephrol, 2005, 20(12): 1738-1743
[16]Tabel Y, Berdeli A, Mir S, et al. Effects of genetic polymorphisms of the renin-angiotensin system in children with nephrotic syndrome. J Renin Angiotensin Aldosterone Syst, 2005, 6(3): 138-144
[17]Tsai IJ, Yang YH, Lin YH, et al. Angiotensin-converting enzyme gene polymorphism in children with idiopathic nephrotic syndrome. Am J Nephrol, 2006, 26(2): 157-162
[18]Dang XQ(党西强), Yi ZW, He XJ, et al. Angiotensin I-converting enzyme gene polymorphism in children with nephrotic syndrome. Chin J Pediatr(中华儿科杂志), 2000, 38(5): 288-291
[19]杜悦新. 血管紧张素转换酶基因插入/缺失多态性与儿童原发性肾病综合征的相关研究. 天津医科大学, 2009
[20]Gao Y(高岩), Zhong F, Wan GP, et al. Angiotensin 1-converting enzyme gene polymorphism in children with primary nephritic syndrome. Chinese Journal of Practical Pediatrics(中国实用儿科杂志), 2003, 18(9): 549-552
[21]Meng Q(孟群), Shen Y, Jiang ZF, et al. Research on AGT(M235T) and ACE(I/D) gene polymorphisms in children with primary nephrotic syndrome. J Appl Clin Pediatr(中国实用儿科杂志), 2007, 22(6): 420-423
[22]沈茜. 血管紧张素Ⅰ转换酶和血小板活化因子分解酶基因多态性在小儿原发性肾病综合征中的意义. 复旦大学, 2004
[23]You YW(尤燕舞), Lin X, Wang J, et al. Study on gene polymorphism of renin angiotensin system in refractory nephrotic syndrome children in zhuang population of west Guangxi Zhuang Autonomous Region. Chinese Journal of Practical Pediatrics(实用儿科临床杂志), 2012, 27(17): 1327-1330
[24]Lee DY, Kim W, Kang SK, et al. Angiotensin-converting enzyme gene polymorphism in patients with minimal-change nephrotic syndrome and focal segmental glomerulosclerosis. Nephron, 1997, 77(4): 471-473
[25]Frishberg Y, Becker-Cohen R, Halle D, et al. Genetic polymorphisms of the renin-angiotensin system and the outcome of focal segmental glomerulosclerosis in children. Kidney Int, 1998, 54(6): 1843-1849
[26]Luther Y, Bantis C, Ivens K, et al. Effects of the genetic polymorphisms of the renin-angiotensin system on focal segmental glomerulosclerosis. Kidney Blood Press Res, 2003, 26(5): 333-337
[27]Hori C, Hiraoka M, Yoshikawa N, et al. Significance of ACE genotypes and medical treatments in childhood focal glomerulosclerosis. Nephron, 2001, 88(4): 313-319
(本文编辑:丁俊杰)
Relationship between ACE gene polymorphisms and pediatric idiopathic nephrotic syndrome: a meta-analysis
XIEMin-juan1,XUShi-zhang2,FUXiao-yi1
(1DepartmentofPathology,YichunUniversity,Yichun336000; 2DepartmentofNephrology,YichunPeople'sHospital,JiangxiProvince,Yichuan336000,China)
FU Xiao-yi,E-mail:1059139963@qq.com
ObjectiveTo assess the relationship between angiotensin converting enzyme (ACE) gene polymorphism and pediatric idiopathic nephrotic syndrome (PNS).MethodsCase-control studies searched from the database of PubMed, EMBASE, Wiley Online Library, Cochrane Library, Science Citation Index, Google Scholar, China National Knowledge Infrastucture, Wanfang Data, China Biology Medicine, China science and technology journal were recruited to summarize the association betweenACEgene polymorphisms with PNS from January 2000 to May 2014. Meta-analysis of the frequency of D, I alleles and DD, DI, II genotypes between PNS group and the control group were performed by Stata 12.0 software.Results Fourteen literatures including 2 849 subjects (1 264 in PNS group and 1 585 in the control group) were recruited. ① The frequency of D allele in PNS group was higher than that in the control group (OR=1.277,95%CI 1.080-1.509,P=0.004)and the frequency of I allele in PNS group was lower than that in the control group (OR=0.811,95%CI 0.738-0.892,P<0.001). ② The frequency of DD genotype in PNS group was higher than that in the control group (OR=0.746,95%CI 0.634-0.877,P<0.001), the frequency of II genotype in PNS group was lower than that in the control group (OR=0.746,95%CI 0.634-0.877,P<0.001) and there was no significant difference of the frequency of DI genotype between PNS and the control groups. ③ Six literatures did not meet Hardy-Weinberg equilibrium, but it did not bias the study by sensitive analysis. ④ The articles reported D allele and DD genotype showed significant heterogeneity. The control group and race could explain partial heterogeneity, but Hardy-Weinberg equilibrium was not the cause of heterogeneity.ConclusionThe relation about DD gene and D allele with PNS was not indubitable. The strength of the association about ACE gene and PNS gene was possibly lower.
Angiotensin converting enzyme; Gene polymorphism; Pediatrics; Nephritic syndrome; Meta-analysis
10.3969/j.issn.1673-5501.2015.05.009
1 江西省宜春学院病理教研室 宜春,336000;2 江西省宜春市人民医院肾内科 宜春,336000
傅小一,E-mail:1059139963@qq.com
2015-01-24
2015-07-12)