牛痘疫苗接种家兔炎症皮肤提取物早期治疗颈髓过伸伤的疗效观察
2014-02-14接健陈福扬冯玉旭徐国浩王梅生
接健 陈福扬 冯玉旭 徐国浩 王梅生
牛痘疫苗接种家兔炎症皮肤提取物早期治疗颈髓过伸伤的疗效观察
接健 陈福扬 冯玉旭 徐国浩 王梅生
目的探讨早期应用牛痘疫苗接种家兔炎症皮肤提取物 ( Neurotropin,NTP ) 治疗颈髓过伸伤的初步临床疗效。方法2010 年 1 月至 2014 年 1 月,我科收治的部分颈椎过伸伤患者 20 例,随机数表法分为 NTP 组 ( NTP 治疗 ) 和对照组 ( 非 NTP 治疗 )。NTP 组应用 NTP 结合牵引治疗 3 周后,石膏固定 3 个月;对照组仅行颌枕带牵引治疗 3 周,石膏固定 3 个月。应用视觉模拟评分法 ( visual analogue scale,VAS ) 测定两组患者的疼痛、肢体麻木及触电感,并记录和比较两组治疗前、牵引结束时以及治疗结束时的评分。结果牵引结束时,NTP 组患者疼痛、肢体麻木及触电感均较治疗前明显改善,其疼痛、肢体麻木及触电感的 VAS评分 ( 1.2±0.78 ) 分、( 1.6±0.84 ) 分、( 0.6±0.51 ) 分均较治疗前 ( 6.2±1.81 ) 分、( 5.3±1.15 ) 分、( 5.4± 0.84 ) 分明显减少,差异有统计学意义 ( P<0.05 );对照组除触电感外患者疼痛、肢体麻木感的 VAS 评分( 2.3±0.82 ) 分、( 2.9±0.99 ) 分也均较治疗前 ( 7.1±1.37 ) 分、( 4.3±1.56 ) 分明显减少,差异有统计学意义 ( P<0.05 );且 NTP 组患者疼痛、肢体麻木及触电感 VAS 评分分别小于对照组,差异有统计学意义 ( P<0.05 )。治疗结束时,两组的疼痛、麻木、触电感 VAS 评分分别与各自牵引结束时的变化均不大,差异无统计学意义 ( P>0.05 );NTP 组患者疼痛、肢体麻木及触电感的 VAS 评分 ( 1.3±0.98 ) 分、( 1.8±0.86 ) 分、( 0.5±0.49 ) 分仍分别小于对照组 ( 2.6±0.49 ) 分、( 2.9±1.26 ) 分、( 1.8±0.76 ) 分,差异均有统计学意义 ( P<0.05 )。20 例至解除石膏固定时,颈椎力线均恢复,颈椎稳定,无颈椎不稳定、肺炎、褥疮等并发症的发生。Frankel 分级 A 级的 3 例中 2 例为 NTP 治疗,1 例为非 NTP 治疗,治疗后均获不同程度的改善,其中 2 例改善至 C 级,1 例改善至 D 级。结论NTP 结合保守牵引治疗可以有效减轻患者的颈椎过伸伤患者的神经症状,明显改善患者疼痛、肢体麻木及触电感。
椎间盘移位;颈椎;治疗结果;药物疗法
颈椎过伸性损伤是颈椎过度伸展性暴力造成的颈脊髓损伤,通常有较轻微或隐匿的骨损伤,X 线多无异常征象。牛痘疫苗接种家兔炎症皮肤提取物 ( Neurotropin,NTP ) 为从牛痘免疫病毒疫苗接种到家兔皮肤的炎性组织中提纯而成的一种非蛋白小分子生物活性物质,在颈腰椎退行性疾病及术后疼痛防治方面已得到广泛应用,但其对过伸伤患者急性期的疼痛麻木及触电感的治疗尚缺乏临床报道[1-3]。因此,2010 年 1 月至 2014 年 1 月,我科利用 NTP 结合牵引治疗部分颈椎过伸伤患者,并观察其治疗颈髓过伸伤的初步临床疗效,为 NTP 治疗颈髓过伸伤的临床应用研究提供基础,现报道如下。
资料与方法
一、纳入和排除标准
纳入标准:( 1 ) 颈髓过伸伤后 8 h 内入院者;( 2 ) 椎管内无明显骨性致压物者;( 3 ) 无椎管明显狭窄者;( 4 ) 脊髓水肿范围不局限者;( 5 ) 未见明显不稳定性骨折现象者;( 6 ) 有合并手术禁忌证者。
排除标准:( 1 ) 骨折患者;( 2 ) 椎管内有继发性椎管狭窄者。
二、一般资料
入组 20 例,其中男 16 例,女 4 例,年龄 26~67 岁,平均 50.05 岁。车祸伤 12 例,高处跌落伤6 例,其它外伤 2 例。20 例均有脊髓损伤,其中损伤节段在 C4的 12 例,C5的 6 例,C6的 2 例。采用 ASIA 改良 Frankel 分级标准[4]:A 级 3 例,B 级 4 例,C 级 7 例,D 级 6 例。入院辅助检查未发现明显神经压迫现象,部分患者可见颈椎间盘突出表现;上肢症状明显重于下肢,手部功能障碍重于肩肘部,其中部分患者出现感觉分离。X 线检查:颈椎屈度过伸 12 例,变直 4 例,中立 4 例。椎管狭窄者 12 例,占 60%,狭窄节段以 C4~5最明显。椎前软组织水肿 18 例,椎体退行性变 19 例。MRI 检查:椎前血肿和水肿 12 例,前纵韧带断裂 3 例,椎间盘撕裂 2 例、突出 17 例;脊髓受压变形 16 例、水肿 20 例,髓内弥漫性出血 2 例,髓内血肿 7 例,T2像示颈髓内均有不同程度的高信号影。
三、实验分组
将 20 例随机数表法[5]分为 NTP 治疗组 ( NTP组 ) 和非 NTP 治疗组 ( 对照组 ),各 10 例。两组治疗前性别、年龄、Frankel 分级、疼痛、肢体麻木及触电感等情况比较,差异无统计学意义 ( P>0.05 ) ( 表1)。
表1 两组的一般情况比较 (±s )Tab.1 Comparison of the general conditions between the 2 groups (±s )
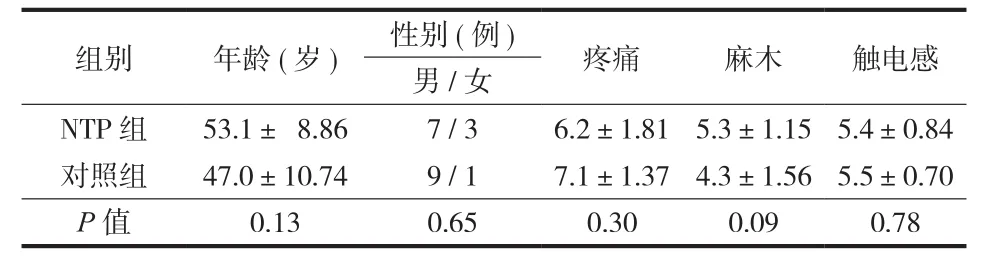
表1 两组的一般情况比较 (±s )Tab.1 Comparison of the general conditions between the 2 groups (±s )
组别 年龄 ( 岁 ) 性别 ( 例 ) 疼痛 麻木 触电感男 / 女NTP 组 53.1± 8.86 7 / 3 6.2±1.81 5.3±1.15 5.4±0.84对照组 47.0±10.74 9 / 1 7.1±1.37 4.3±1.56 5.5±0.70 P 值 0.13 0.65 0.30 0.09 0.78
四、治疗方法
NTP 组病例均选择 NTP 结合颌枕带牵引治疗:入院后指导患者卧床休息,颈部沙袋制动,行颌枕带牵引,注射用甲泼尼龙琥珀酸钠 120 mg 每日 1 次冲击治疗,NTP 10.8 U 每日 1 次静脉滴注,缓解症状,高压氧治疗,牵引后 3 周改头颈胸石膏固定,共 3 个月解除。对照组行颌枕带牵引治疗:入院后指导患者卧床休息,颈部沙袋制动,仅注射用甲泼尼龙琥珀酸钠 120 mg 每日 1 次冲击治疗,脱水补液,高压氧治疗,牵引后 3 周改头颈胸石膏固定,共 3 个月解除,不使用 NTP 作缓解症状及营养神经处理。
五、疗效观察
应用视觉模拟评分法 ( visual analogue scale,VAS ) 测定两组患者的疼痛、肢体麻木及触电感[6]。分别记录两组治疗前、牵引结束时以及治疗结束时的评分结果,并比较两组评分。
六、统计学方法
采用 SPSS 14.0 软件对数据进行处理,计数资料采用 χ2检验,计量采用 t 检验,检验水准 α=0.05。
结 果
本研究中患者多为外地患者,3 个月解除石膏固定后失访患者较多,故未进行长期随访。
牵引结束时,NTP 组患者疼痛、肢体麻木及触电感均较治疗前明显改善,其疼痛、肢体麻木及触电感的 VAS 评分均较治疗前明显减少,且差异均有统计学意义 ( P<0.05 );对照组除触电感外患者的疼痛、肢体麻木感也均较治疗前改善,差异有统计学意义 ( P<0.05 );且 NTP 组患者疼痛、肢体麻木及触电感的 VAS 评分分别小于对照组,差异均有统计学意义 ( P<0.05 )。治疗结束时,两组的疼痛、麻木、触电感 VAS 评分分别与各自牵引结束时比较,变化均不明显,差异无统计学意义 ( P>0.05 );NTP 组患者疼痛、肢体麻木及触电感的 VAS 评分仍分别小于对照组,差异均有统计学意义 ( P<0.05 ) ( 表2 )。
20 例至解除石膏固定时,颈椎力线均恢复,颈椎稳定,无颈椎不稳定、肺炎、褥疮等并发症的发生。Frankel 分级 A 级的 3 例中 2 例为 NTP 治疗,1 例为非 NTP 治疗,治疗后均获不同程度的改善,其中 2 例改善至 C 级,1 例改善至 D 级。
讨 论
颈椎过伸伤是一种常见的颈椎损伤,而过伸外伤是致伤的主要原因,多见于高处坠落、跌倒和交通事故中头面部撞击障碍物产生过伸性暴力,而直接遭受打击者少见。该损伤合并骨折脱位者较少见,偶有颈椎体下缘撕脱骨折者。有报道,该损伤占脊髓损伤发病机制的 40%~80%[7]。Taylor[8]对颈椎过伸伤的损伤机制进行了研究,经过尸检及实验均证实此种损伤在过伸位时引起,过伸时黄韧带前突,椎管前方的间盘或骨赘也格外突出,二者相互挤压致脊髓损伤。近年来,国内外对影像学上没有骨折脱位改变而颈脊髓损伤的情况进行了大量探索,认为颈椎过伸伤存在前述的颈椎管发育性狭窄、颈椎退行性变、颈椎不稳及后纵韧带骨化 ( ossification of the posterior longitudinal ligament,OPLL ) 等原始基础病变[9]。在颈椎过伸伤的治疗方法选择上,国内外一直存在争议。目前,多数学者认为,MRI 特征性改变与神经损害的对应关系有助于了解脊髓损伤的程度和预后,对于 MRI 示颈髓以水肿为主且临床表现较轻者,采取非手术疗法,可获得较满意效果;对于 MRI 示脊髓受压、颈髓出血肿胀明显、蛛网膜下隙消失且临床表现较重者,手术减压有助于减轻脊髓的继发性损伤和促进其功能恢复[10-11]。Yazdani 等[12]利用骨髓间充质基质细胞和雪旺细胞结合治疗 8 例过伸性脊髓损伤,患者接受这种自体细胞移植到直接损伤部位,治疗后 24 个月,患者排尿和排便感觉有一定的改善。Sengul等[13]利用 β 干扰素治疗急性脊髓过伸伤大鼠,接受β 干扰素治疗的大鼠其组织中热休克蛋白 70 水平显著提高,出血、水肿坏死及多形核白细胞浸润明显减少。这项研究的结果表明,β 干扰素可能通过增加细胞热休克蛋白 70 水平,来治疗脊髓损伤。
表2 两组疼痛、肢体麻木及触电感 VAS 评分比较 (±s )Tab.2 Comparison of the VAS scores of pain, limb numbness and electrifed sensation between the 2 groups (±s )

表2 两组疼痛、肢体麻木及触电感 VAS 评分比较 (±s )Tab.2 Comparison of the VAS scores of pain, limb numbness and electrifed sensation between the 2 groups (±s )
注:a表示牵引结束时和治疗前比较;b表示治疗结束时和牵引结束时比较Notice:aMeant the comparison at the end of traction and before the treatment;bMeant the comparison at the end of the traction.and treatment
疼痛麻木触电感治疗结束时( 分 ) NTP 组 6.2±1.81 1.2±0.78 1.3±0.98 0.01>0.05 5.3±1.15 1.6±0.84 1.8±0.86 0.00>0.05 5.4±0.84 0.6±0.51 0.5±0.49 0.00>0.05对照组 7.1±1.37 2.3±0.82 2.6±0.49 0.03>0.05 4.3±1.56 2.9±0.99 2.9±1.26 0.04>0.05 5.5±0.70 1.7±0.48 1.8±0.76 0.05>0.05 P 值 0.3 0.02 0.03 0.09 0.00 0.02 0.78 0.00 0.00组别aP 值bP 值治疗前 牵引结束时( 分 )治疗结束时( 分 )aP 值bP 值aP 值bP 值( 分 )治疗前( 分 )牵引结束时( 分 )治疗结束时( 分 )治疗前( 分 )牵引结束时( 分 )
NTP 有效成分的化学结构至今尚未清楚,但多项实验证实其药理作用包括:( 1 ) 通过恢复神经突触传导功能、保护缺氧状态下的神经元、促进神经轴突生长、改善病损神经的传导速度、促进雪旺细胞增殖,从而达到营养修复神经的作用;( 2 ) 调节中枢 5-羟色胺能及去甲肾上腺素能系统,激活疼痛下行性抑制系统,在脊髓水平以上抑制疼痛递质的释放,抑制外周激肽酶活性而减少缓激肽的释放,缓解化学性刺激,减轻局部软组织及神经的水肿,达到镇痛作用;( 3 ) 抑制下丘脑腹内侧核神经元放电活动、调节植物神经功能、改善末梢血循环,从而改善冷感、麻木、感觉过敏等神经症状;( 4 ) 修复调节免疫器官结构及功能[14-15]。非甾体类抗炎镇痛药通过抑制下丘脑内侧核神经元放电活动,调节植物神经早后期的镇痛作用,其效果明显比阿片类药物差,且有封顶效应[16]。由于非甾体类抗炎镇痛药的术后镇痛作用有限,故单独使用不能达到满意的效果,但其与阿片类药物联合使用可明显减少舒芬太尼的用量,同时增强镇痛效果。NTP 是多靶点,多层面的治疗药物,不仅具有镇痛及抗炎的作用,还能缓解了神经源性疼痛及伴发的冷感、麻木、触电等症状[17]。与传统的激素冲击治疗方法相比,神经妥乐平对于中枢神经及周围神经损伤具有更好疗效,尤其对于疼痛及触电感症状改善较明显[18]。
本组结果显示,NTP 组患者各项指标较治疗前均有明显地改善,且较对照组而言,其改善的程度更高,差异有统计学意义 ( P<0.05 )。因此,颈椎过伸伤进行保守治疗同时联用 NTP 可以有效减轻患者的神经症状,对预后起到积极的作用。
[1] Okazaki R, Namba H, Yoshida H, et al. Combined antiallodynic effect of Neurotropin® and pregabalin in rats with L5-spinal nerve ligation. Life Sci, 2013, 92(4-5):259-265.
[2] Chinder PS, Kamath JB, Srivastav H, et al. Research tip neurotropin incorporated nerve sutures. Tech Hand Up Extrem Surg, 2010, 14(3):200.
[3] Yamazaki Y, Kobatake K. Successful treatment of nummular headache with Neurotropin®. J Headache Pain, 2011, 12(6): 661-662.
[4] 侯树勋. 脊柱外科学. 北京: 人民军医出版社, 2005: 355-359.
[5] 金英良, 黄水平, 赵华硕. 利用SPSS产生随机数字的常用方法. 中国卫生统计, 2009, 26(6):659-660.
[6] 苏祥正, 徐辉, 肖嵩华, 等. 神经妥乐平治疗腰椎间盘突出症患者疼痛及麻木症状的临床效果研究. 中国骨与关节杂志, 2014, 3(4):265-267.
[7] Guptarak J, Wiktorowicz JE, Sadygov RG, et al. The cancer drug tamoxifen: a potential therapeutic treatment for spinal cord injury. J Neurotrauma, 2014, 31(3):268-283.
[8] TAYLOR AR. The mechanism of injury to the spinal cord in the neck without damage to vertebral column. J Bone Joint Surg Br, 1951, 33-B(4):543-547.
[9] Xifró X, Puig T, Boadas-Vaello P. Diagnosis and pharmacological treatment of neuropathic pain in spinal cord injury subjects: from laboratory to clinical trial. Med Clin (Barc), 2013, 140(4):175-181.
[10] Bransford RJ, Koller H, Caron T, et al. Cervical spine trauma in diffuse idiopathic skeletal hyperostosis: injury characteristics and outcome with surgical treatment. Spine, 2012, 37(23):1923-1932.
[11] Rahimi-Movaghar V. Clinical trials for the treatment of spinal cord injury:cervical and lumbar enlargements versus thoracic area. Brain, 2009, 132(Pt7):e115-116.
[12] Yazdani SO, Hafizi M, Zali AR, et al. Safety and possible outcome assessment of autologous Schwann cell and bone marrow mesenchymal stromal cell co-transplantation for treatment of patients with chronic spinal cord injury. Cytotherapy, 2013, 15(7):782-791.
[13] Sengul G, Coban MK, Cakir M, et al. Neuroprotective effect of acute interferon-beta 1B treatment after spinal cord injury. Turk Neurosurg, 2013, 23(1):45-49.
[14] 陈明生, 张毅, 罗义骏, 等. 牛痘疫苗接种家兔炎症皮肤提取物联合神经营养液用于腰椎手术失败综合征的临床观察. 临床军医杂志, 2011, 39(1):143-145.
[15] 于杨雅新, 李建国, 王春雷, 等. 牛痘疫苗接种家兔炎症皮肤提取物治疗强直性脊柱炎疼痛的临床观察. 齐齐哈尔医学院学报, 2012, 33(7):912.
[16] Isiordia-Espinoza MA, de Jesús Pozos-Guillén A, Aragon-Martinez OH. Analgesic efficacy and safety of singledose tramadol and non-steroidal anti-inflammatory drugs in operations on the third molars: a systematic review and metaanalysis. Br J Oral Maxillofac Surg, 2014, 52(9):775-783.
[17] 林宪法, 郑燕国, 漆志明, 等. 牛痘疫苗接种家兔炎症皮肤提取物联合硬膜外阻滞治疗腰椎间盘突出症术后残留症状的疗效观察. 中医正骨, 2010, 22(2):12-13.
[18] 雷哲, 王俊. 神经妥乐平治疗神经根型颈椎病54例观察. 中国疼痛医学杂志, 2005, (5):314-314.
( 本文编辑:代琴 )
Preliminary observation of effects of extrace from infammatory cutaneous tissues of the rabbit inoculated with vaccina virus in the treatment of hyperextension injuries of cervical spinal cord
JIE Jian, CHEN Fu-yang, FENG Yu-xu, XU Guo-hao, WANG Mei-sheng. Department of Orthopedics, Nanjing Hospital Pukou Branch, Nanjing Medical University, Nanjing, Jiangsu, 211800, PRC
ObjectiveTo explore the preliminary clinical effects of extrace from infammatory cutaneous tissues of the rabbit inoculated with vaccina virus, also called Neurotropin ( NTP ) in the treatment of hyperextension injuries of cervical spinal cord.MethodsFrom January 2010 to January 2014, 20 patients with hyperextension injuries of cervical spinal cord were adopted, who were randomly divided into the NTP group and the control group. Traction was performed on the patients in the NTP group for 3 weeks and then plaster fxation for 3 months, besides the NTP treatment. Occipital-jaw-traction was performed on the patients in the control group for 3 weeks and then plaster fixation for 3 months. The Visual Analogue Scale ( VAS ) was used to assess pain, limb numbness and electrified sensation in both groups, and the scores before the treatment and at the end of traction and treatment were recorded and compared.ResultsThe VAS scores of pain, limb numbness and electrifed sensation in the NTP group were ( 6.2±1.81 ) points, ( 5.3±1.15 ) points and ( 5.4±0.84 ) points before the treatment, which were obviously reduced to ( 1.2±0.78 ) points, ( 1.6±0.84 ) points and ( 0.6±0.51 ) points at the end of traction. The differences between them were statistically signifcant ( P<0.05 ). The VAS scores of pain and limb numbness in the control group were ( 7.1±1.37 ) points and ( 4.3±1.56 ) points before the treatment, which were obviously reduced to ( 2.3±0.82 ) points and ( 2.9±0.99 ) points atthe end of traction. The differences between them were statistically signifcant ( P<0.05 ). The VAS scores of pain, limb numbness and electrifed sensation in the NTP group were lower than that of the control group, and the differences between them were statistically signifcant ( P<0.05 ). No obvious differences at the end of the treatment and traction were noticed in the VAS scores of pain, limb numbness and electrified sensation in both groups, which were not statistically signifcant ( P>0.05 ). The VAS scores of pain, limb numbness and electrifed sensation in the NTP group were ( 1.3±0.98 ) points, ( 1.8±0.86 ) points and ( 0.5±0.49 ) points at the end of treatment, which were respectively lower than ( 2.6±0.49 ) points, ( 2.9±1.26 ) points and ( 1.8±0.76 ) points in the control group. The differences between them were statistically signifcant ( P<0.05 ). Cervical spine alignment was restored in all the patients when the plaster was removed, and the cervical spine was stable. No cervical unstability, pneumonia or bedsore occurred. According to the Frankel grading system, 2 of the 3 patients rated as grade A underwent NTP treatment, and the last one did not. The improvement in different degrees was achieved in all the 3 patients after the treatment. Among them, 2 patients was improved to grade C and 1 patient to grade D.ConclusionsThe neurological symptoms in the patients with hyperextension injuries of cervical spinal cord can be effectively relieved with the treatment of NTP and conservative traction, and pain, limb numbness and electrifed sensation can be signifcantly improved.
Intervertebral disc displacement; Cervical vertebrae; Treatment outcome; Drug therapy
10.3969/j.issn.2095-252X.2014.12.016
:R683.2
211800 南京医科大学附属南京医院浦口分院 ( 接健 );211803 南京市浦口区中心医院骨科 ( 陈福扬、冯玉旭、徐国浩、王梅生 )
2014-07-31 )