Clinical Observation on Scalp Acupuncture Combined with Rehabilitation Training for Hemiplegia After Stroke
2013-07-18QiuYalong
Qiu Ya-long
Xikou Hospital of Fenghua City, Zhejiang 315502, China
Clinical Observation on Scalp Acupuncture Combined with Rehabilitation Training for Hemiplegia After Stroke
Qiu Ya-long
Xikou Hospital of Fenghua City, Zhejiang 315502, China
Objective: To observe the clinical efficacy of the scalp acupuncture combined with rehabilitation training for hemiplegia.
Methods: One hundred and thirty-six cases with hemiplegia after stroke who met the inclusion criteria were randomly divided into three groups according to visiting sequence. Forty-eight cases in the observation group were treated by scalp acupuncture combined with rehabilitation training, 35 cases in the medicine group were treated by Chinese and Western medicines, and 53 cases in the medicine plus rehabilitation group were treated by Western medicine and rehabilitation training. Patients' consciousness, speech and limb functions were scored before and after treatment, and the results were compared.
Results: After treatment, the scores of consciousness, speech and limb functions after treatment were lower than those before treatment. And their decrease in the observation group were more statically significant than that in the medicine group and the medicine plus rehabilitation group (P<0.01 orP<0.05). The total effective rates of the three groups were significantly different (P<0.01 orP<0.05). The total effective rate of the observation group was better than that of the other two groups (bothP<0.01).
Conclusion: Scalp acupuncture combined with rehabilitation therapy has better effect for stroke hemiplegia.
Acupuncture Therapy; Scalp Acupuncture; Stroke; Complications; Hemipligia; Rehabilitation
Stroke is an emergent cerebrovascular condition often seen in the middle-aged and elderly population. Clinically, it is divided into hemorrhagic stroke and ischemic stroke. Its dysfunction is mainly manifested by consciousness, movement, perception, cognition, speech and emotion, etc. And hemiplegia is the most common dysfunction following stroke. In recent years, the improvement of early diagnosis, treatment and rescue levels has reduced the mortality, and early involvement of rehabilitation also decreased morbidity and increased survival rate, but medical staff still need to pay much attention to the morbidity and recurrence rates. Acupuncture is widely used for hemiplegia, but the specific methods vary.
Rehabilitation is the functional recovery after injury. Rehabilitation after stroke aims to restore function maximumly through integrated measures based on physical therapy and occupational therapy to prevent from disuse and misuse syndrome and reduce sequelae; meanwhile, it can strengthenand use residual function as well as make patients achieve self-care and return to society by the use of tools and the transformation of living environment. This study observed the clinical efficacy of scalp acupuncture combined with rehabilitation in treating post-stroke hemiplegia, and the report is given as follows.
1 Clinical Materials
1.1 Diagnostic criteria
Diagnostic criteria of traditional Chinese medicine were proposed based on theStandard for Diagnosis and Therapeutic Effect Evaluation of Stroke(Trial)[1]. Diagnostic criteria of Western medicine is proposed referring to theKey Diagnostic Points for Cerebrovascular Diseases[2], and all the patients were diagnosed by CT or MRI.
1.2 General data
One hundred and thirty-six patients were enrolled, including 70 men, and 66 women; their mean age was 63 years old, ranging from 35 to 83 years old; their duration varied from 5 to 130 d with an average of 15.4 d; 113 cases were cerebral infarction, 23 cases were cerebral hemorrhage (patients with subarachnoid hemorrhage were not enrolled).
Patients were grouped according to their visiting sequence. Forty-eight patients who were admitted in hospital or outpatient and asked for acupuncture treatment since August 1, 2005 were enrolled in the observation group. Thirty-five patients who were treated by Western medicine before August 1, 2005 were enrolled in the medicine group. And 53 patients who accepted Western medicine and rehabilitation training after August 1, 2005 due to fears of acupuncture were enrolled in the medicine plus rehabilitation group. Statistically, According to statistical analysis, the patients' age, disease duration, disease type, treatment score in three groups were not statistically significantly different (P>0.05), indicating the three groups were comparable.
2 Therapeutic Methods
2.1 Observation group
2.1.1 Scalp acupuncture
Points: Take the upper 2/5 area on the Contralateral Anterior Oblique Line of Vertex- Temporal (MS 6) for lower limb paralysis patient, and take the middle 2/5 area on the contralateral Anterior Oblique Line of Vertex-Temporal (MS 6) for patient with upper limb paralysis or paresthesia, and take lower 1/5 area on the contralateral Anterior Oblique Line of Vertex-Temporal (MS 6) for patient with facial paralysis or paresthesia; take upper 2/5 area on the contralateral Posterior Oblique Line of Vertex-Temporal (MS 7) for patient with lower limbs paresthesia[3].
Operation: After routine disinfection on the acupoint area, filiform needle of 0.30 mm in diameter and 40-50 mm in length was quickly inserted into scalp by 15°-20° angle, and you can have a reduced resistance sensation when the needle reaches the lower subgaleal, then make the needle parallel with the scalp and continue twisting and rotating till reaching appropriate depth, and rapidly twist the needle for 1-2 min and retain it for 2 h. The operation is conducted every other day, 10 times as a course of treatment.
2.1.2 Rehabilitation
Modern rehabilitation methods were used. The patients were treated by comprehensive treatment including physical therapy and occupational therapy.
2.2 Medicine group
The patients were treated by conventional medicine, such as symptomatic treatment, stimulating blood circulation to expel blood stasis and so on.
2.3 Medicine plus rehabilitation group
The patients in this group were treated by the combination of Western medicine (same as the medicine group) and rehabilitation (same as the observation group).
3 Therapeutic Efficacy Observation
3.1 Efficacy criteria
This is accorded to the therapeutic efficacy criteria of stroke in theGuiding Principles for Clinical Study of New Chinese Medicines[4]. Scoring method was used before and after treatment to evaluate patients’consciousness, speech, physical activity and other main symptoms. Specific scoring rules are as follows.
3.1.1 State of consciousness
0 point: Be conscious.
1 point: Drowsy, but can be aroused, answer or respond.
2 points: Lethargic or obtunded, cannot answer or respond accurately.
3 points: Coma.
4 points: Coma with manifestations of collapse syndrome such as heavy sweating, cold limbs, closed eyes and open mouth, released hands and enuresis, weak pulse.
3.1.2 Speech function
0 point: Normal speech.
1 point: Fair speech function and anomia.
2 points: Can say a sentence but can not express precisely.
3 points: Cannot finish a word or phrase.
4 points: Almost cannot say anything.
3.1.3 Upper limbs and shoulder joints
0: Normal.
1 point: Normal lifting, but poor muscle force.
2 points: Can lift the arm till shoulder or slightly over the shoulder.
3 points: Cannot reach the shoulders.
4 points: Cannot move or swing slightly from anterior to posterior.
3.1.4 Knuckles of upper limbs
0 point: Normal.
1 point: Effectively separate finger movements but poor muscle force.
2 points: Just can make a fist and release fingers.
3 points: Be flexed and cannot make a fist or extend.
4 points: Cannot move.
3.1.5 Lower limbs and hip
0: Normal.
1 point: Elevation >45 °.
2 points: Elevation <45 °.
3 points: Can swing and slide.
4 points: Cannot move.
3.1.6 Toe joints
0: Normal.
1 point: Complete but weak extension and flexion.
2 points: Insufficiency flexion and extension.
3 points: Slight movement.
4 points: Cannot move.
3.1.7 Comprehensive functions
0 points: Independent and can communicate.
1 point: Independent living; able to do simple movements; there are some dysfunctions.
2 points: Able to walk; but needs help.
3 points: Able to stand and take a step, but relies on help.
4 points: Immobile.
Efficacy was assessed by Nimodipine method which calculates the reduction rate of the overall score.
Reduction rate = (Score of before treatment - Score of after treatment) ÷ Score of before treatment × 100%.
Recovery: The reduction rate ≥85%.
Markedly effective: The reduction rate ≥50%, but<85%.
Effective: The reduction rate ≥20%, but <50%.
Invalid: The reduction rate <20%.
3.2 Results
3.2.1 Observation on scores of consciousness, speech and extremity motor functions
There was no statistical difference among the three groups in consciousness, speech function, and extremity motor function scores before treatment (P>0.05), indicating that they were comparable. After treatment, the consciousness, speech function, extremity motor function scores of the three groups were significantly lower, and the observation group decreased more than the other two groups (P<0.01), indicating that the observation group had the best effect on patients’ above symptoms improvement, and the medicine plus rehabilitation group followed, and the medicine group had lowest effect (table 1).
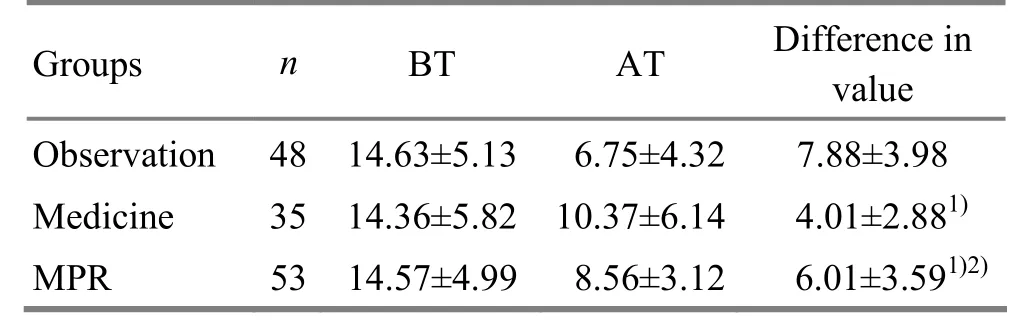
Table 1. Three group comparison of scores of consciousness, speech function and extremity motor function before and after treatment
3.2.2 Total effective rate observation
The total effective rate of the three groups were significantly different (P<0.01), and the observation group was higher than the medicine group and the medicine plus rehabilitation group, and the last group showed higher efficacy than the medicine group (table 2).

Table 2. Comparison of the total efficient rate of the three groups (case)
4 Discussion
In ancient literature, because of the historical conditions and the personal experience, there were a lot of different etiology and pathogenesis theories on stroke and its treatment methods. Based on theories of‘wind is the yang pathogen’ and ‘treatment for Wei-Flaccidity only by selecting Yangming Meridians’,the traditional treatment of acupuncture for stroke mainly uses wind-expelling and meridian-activating method and mostly selects the acupoints in the Yangming Meridians, which is to nourish qi and blood. However, the clinical efficacy is often poor.
Stroke is one kind of the cerebrovascular disorders, and it’s clinically divided into hemorrhagic and ischemic categories. The lesion is in the brain, so the focus of treatment should be on the brain firstly. Scalp acupuncture can directly stimulate the head to promote physical recovery. The CT examination has proved that in the early phase, scalp acupuncture in corresponding stimulation area can promote absorption of hematoma and brain edema[5-8]. Therefore, the earlier acupuncture intervenes, the better the result will be. And the best treatment timing is at the initial stage.
Modern rehabilitation therapy is mainly based on physical therapy and occupational therapy to maximize the recovery, to prevent misuse and disuse syndrome as well as reduce sequelae[9-11]; it also strengthens the residual function, helps patients become as independent as possible and return to society through the use of assistant appliances, as well as the transformation of the living environment. Rehabilitation treatment time should be synchronized with the acupuncture treatment, but the content and intensity of rehabilitation items depend on individual differences.
Because scalp acupuncture can directly stimulate the head, while the rehabilitation mainly aims at treating the limbs, so that the two complement each other to relieve symptoms and treat lesion simultaneously[12-13]. That is why the effect is better compared to rehabilitation alone. In the simple use of acupuncture, there is a possibility of disuse and misuse of limbs, which often induces difficulty treating sequelae at the late phase and negative influence on the efficacy. Therefore, its efficacy is not as good as the combining use of the two methods.
[1] Collaborative Group of Acute Encephalopathy of State Administration of Traditional Chinese Medicine. Standard for diagnosis and therapeutic effect evaluation of stroke (trial). Beijing Zhongyiyao Daxue Xuebao, 1996, 19(1): 55-56.
[2] Chinese Neuroscience Society, Chinese Neurosurgical Society. Key diagnostic points for cerebrovascular diseases. Zhonghua Shenjingke Zazhi, 1996, 29(6): 379-380.
[3] General Administration of Quality Supervision, Inspection and Quarantine of the People's Republic of China, Standardization Administration of the People’s Republic of China. Standardized Manipulations of Acupuncture and Moxibustion-Part 2: Scalp Acupuncture. Standards Press of China, 2008.
[4] Ministry of Health of the People’s Republic of China. Guiding Principles for Clinical Study of New Chinese Medicines. Beijing: China Medico-Pharmaceutical Science & Technology Publishing House, 2002: 99-104.
[5] Li J, Xiao JH, Dong GR. Clinical study on effect of scalp acupuncture in treating acute cerebral hemorrhage. Zhongguo Zhongxiyi Jiehe Zazhi, 1999, 19(4): 203-205.
[6] Liu WA, Wu QM, Li XR, Li DD, Fu L, Yi XC, Zhang P. Observations on the efficacy of combined treatment of stroke hemiplegia with scalp electroacupuncture and stoke unit. Shanghai Zhenjiu Zazhi, 2010, 29(3): 149-151.
[7] Xiao XH, Li RC, Zhu HX, Shuai JY, Xu MF, Fu Y. Clinical study of the treatment of ischemic stroke with scalp point-through-point electroacupuncture. Shanghai Zhenjiu Zazhi, 2008, 27(6): 6-8.
[8] Li XJ, Liu WD, Hu CH. Influence of concomitant scalp acupuncture and kinetotherapy on somatosensory evoked potential in hemiplegia patients. Shanghai Zhenjiu Zazhi, 2009, 28(10): 575-576.
[9] Zhu JG, Wei Y, Yuan DC. The influence of positive sequential treatment of modern comprehensive rehabilitation therapy on motor function of patients with acute stroke. Nao Yu Shenjingbing Zazhi. 2008, 16(4): 496-497.
[10] Liu F, Yu CD. Research progress of acupuncture combined with rehabilitation therapy for stroke. Zhongxiyi Jiehe Zazhi, 2007, 5(11): 1097-1098.
[11] Yang D, Zhang CE, Xu Li. Observation on therapeutic effect of acupuncture plus rehabilitation for hemiplegia following stroke. J Acupunct Tuina Sci, 2008, 6(4): 219-221.
[12] Huang LN, An JM, Su TS, Wang P, Dong L, Zhang RP, Ren YJ, Ren YY. Clinical randomized controlled trial of scalp acupuncture theatment for vascular dementia. Shanghai Zhenjiu Zazhi, 2010, 29(2): 79-82.
[13] Xie DL, Zhu LF, Liu HY, Zeng CY. Application of P300 in scalp acupuncture for cognitive disorder due to cerebral infarction. J Acupunct Tuina Sci, 2012, 10(1): 26-28.
Translator: Deng Ying
R246.6
A
Date: May 20, 2013
Author: Qiu Ya-long, attending physician.
E-mail: zjtnyx@126.com
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Clinical Observation on Acupoint Sticking Therapy for Lumbar Intervertebral Disc Hernination
- Clinical Observation on Electroacupuncture for Post-stroke Flaccid Paralysis
- Effect of Electroacupuncture on Anxiety and Craving in Heroin Addicts During Detoxification
- Clinical Study on Acupoint Injection for Primary Osteoporosis
- Treatment of Post-stroke Spastic Hemiplegia by Acupuncture plus Rehabilitation Training
- Immediate Effects of Hegu Needling on Adhesive Scapulohumeral Periarthritis