Mental health literacy in Changsha, China
2011-12-11YuanPENGXiaolingWANGPingfeiLIKunLIU
Yuan PENG*, Xiaoling WANG, Pingfei LI, Kun LIU
· Research Article ·
Mental health literacy in Changsha, China
Yuan PENG*, Xiaoling WANG, Pingfei LI, Kun LIU
Objective:Assess public awareness about mental health and the prevention of mental illnesses in Changsha, China.Methods:A multistage cluster-sampling method identified 1 660 households in two rural and two urban communities in the Changsha Municipality. One family member 15 years of age or older randomly selected from each household was asked to complete a standardized 20-item survey about mental health awareness developed by the Chinese Ministry of Health (MOH).Results:1 563 valid surveys were completed by 676 males and 887 females who had a mean (SD) age of 41.9 (15.9) years.The mean (SD) proportion of correct responses in the total sample was 68.5% (46.4%); the proportion correct in urban respondents [70.5% (13.6%)] was higher than that in rural respondents [66.2% (13.5%)] (t=6.18,p<0.001). The proportion of correct responses had a significant negative correlation with age (r=-0.21;p<0.001), a significant positive correlation with level of education (r=0.28,p<0.001) and varied by occupation and marital status. A stepwise regression analysis found that level of education, age and occupation (farmer or worker versus other occupations) were independently related to the level of mental health literacy. The overall internal consistency of the 20 items in the survey and of the four subscales in the survey were weak (alpha=0.27-0.57).Conclusion:The overall level of awareness about mental health issues in Changsha residents is relatively high but there are still some areas, particularly regarding the causes of mental disorders, that are in need of improvement. The level of mental health literacy varies substantially by demographic characteristics so cohort-specific educational interventions will be needed to effectively improve community awareness. Further revision of the MOH survey will be needed to improve its reliability, validity and internal consistency.
General public; Mental health; Mental disorders; Knowledge and awareness; Survey
1 Introduction
The level of awareness about mental health issues and about the prevention of mental disorders in community members is one of many factors that influence the rate of care-seeking in persons with psychological problems and the stigmatization of persons with mental illnesses[1]. Improving mental health literacy in a community is presumed to be one of the cornerstones of improving overall mental health[2].Standardized assessment of community member’s knowledge about mental illness is essential to both the development and evaluation of mental health promotion campaigns. A wide variety of measures have been employed to assess community-based mental health literacy[3,4]but differences in the content of these instruments makes it impossible to make meaningful comparisons between communities. The current study administered an instrument developed by the Chinese Ministry of Health for use around China—Survey Questionnaire on Knowledge of Mental Health and Mental Disorder Prevention among the General Public[5]—to assess mental health literacy in community members of Changsha, China from January to March 2011.
2 Subjects and Methods
2. 1 Sampling of subjects
The identification process for subjects is shown in Figure 1. A multistage cluster-sampling method was employed to identify subjects. Two urban districts(Furong and Yuelu) and two rural counties (Wangcheng and Ningxiang) were randomly selected from nine districts and counties of the Changsha Municipality (the capital of Hunan Province). One urban neighborhood was randomly selected from each of the two districts and one rural village was randomly selected from each of the counties. 1,660 households were randomlyselected from the four communities. Interviewers visited the households and randomly selected one family member 15 years of age or older who was in the household at the time of the visit and asked him or her to complete the survey. If no person was present in a selected household an adjacent household was selected. After respondents completed the survey the questionnaire was reviewed by the interviewer to ensure that there were no inconsistencies or missing items.
2. 2 Content of survey
The Survey Questionnaire on Knowledge of Mental Health and Mental Disorder Prevention among the General Public, which was developed by the Chinese Ministry of Health (MOH), was used in the current survey. The questionnaire contains 20 self-completion items (shown in Table 1), most of which derive from the core information contained in the ‘MOH Essential Knowledge for Mental Health Advocacy and Education’released by the Administrative Office of China’s MOH[5].
The scale has previously been used with middle-school students[6]but not with community-based samples.The reliability and validity of the scale in middle school students was acceptable[6](overall alpha=0.73 test-retest reliability ICC=0.68) but the reliability and validity in community samples have not been formally assessed.
Based on the work with middle students[6], the 20-item scale is divided into four subscales that assess knowledge about 1) the characteristics of mental illnesses (items 1, 3, 5, 8, 11, 13 and 14); 2) the causes of mental illnesses (items 2, 4, 12, 15 and 15); 3) the prevention of mental illnesses (items 6, 7, 9 and 10);and 4) mental health promotion activities (items 17-20).Correct responses were ‘yes’ for items 1, 3, 5, 7, 8, 11,12 and 15-20, and ‘no’ for items 2, 4, 6, 9, 10, and 13.The correct answers are given one point and incorrect answers are given 0 points, so the range of total scores is from 0 to 20 with a higher score representing a higher level of mental health literacy. These scores are converted to a ‘percent correct’ measure in the analysis.
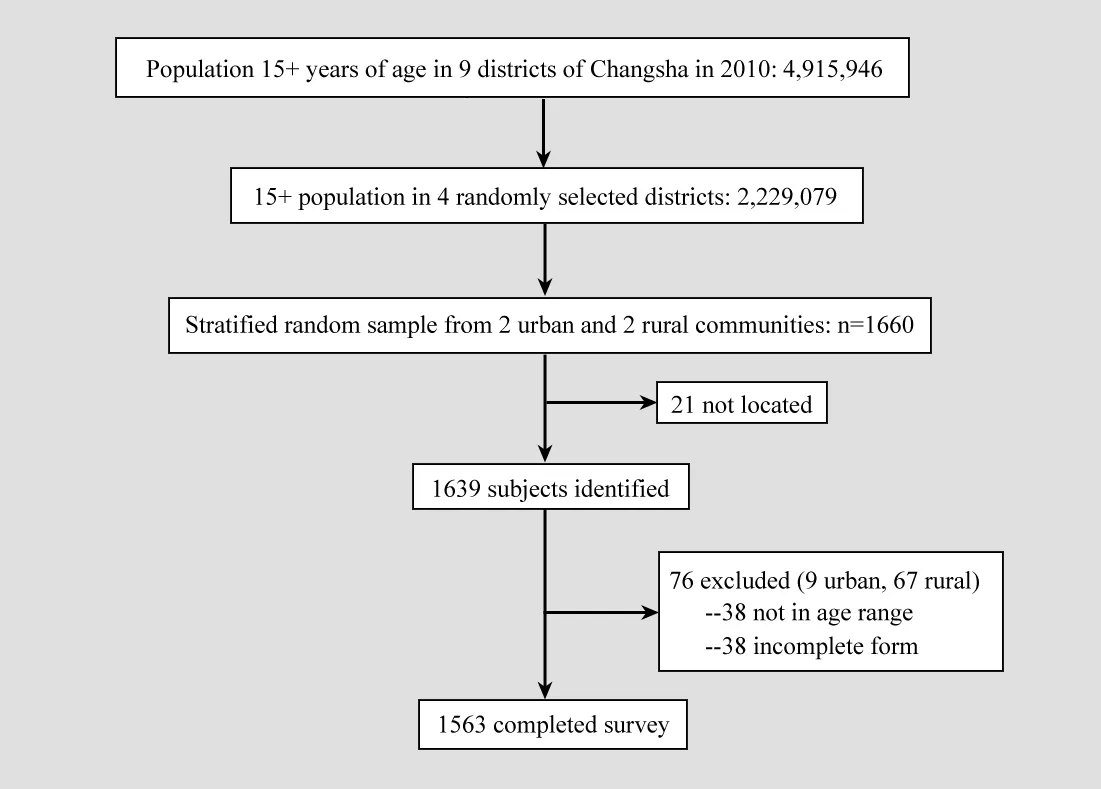
Figure 1. Flowchart of subject enrollment
2. 3 Statistical analysis
Analyses of the survey results between different categories of respondents used t-tests and ANOVA with the Tukey test used to make poshoc comparisons between multiple categories of subjects. Pearson correlation coefficients were used to assess the relationship of age and level of education with the level of mental health literacy. Regression analysis was used to identify the characteristics of respondents that were independently related to the assessed level of mental health literacy. The internal consistency of the survey and its subscales were assessed using alpha values. The study was approved by the Changsha City Bureau of Health.
3 Results
In 21 cases the selected household or individual was not located and an appropriate replacement household was not available. Among the 1,639 individuals who were identified, 1,563 (95.4%) had valid surveys; they included 676 males and 887 females with a mean age of 41.9 years (SD=15.9, range 15-86). Of the 76 invalid questionnaires, 38 lacked age information and the remaining 38 forms had incorrect codes or missing items; 67 of these invalid forms were completed by respondents from rural communities and 9 by respondents from urban communities.
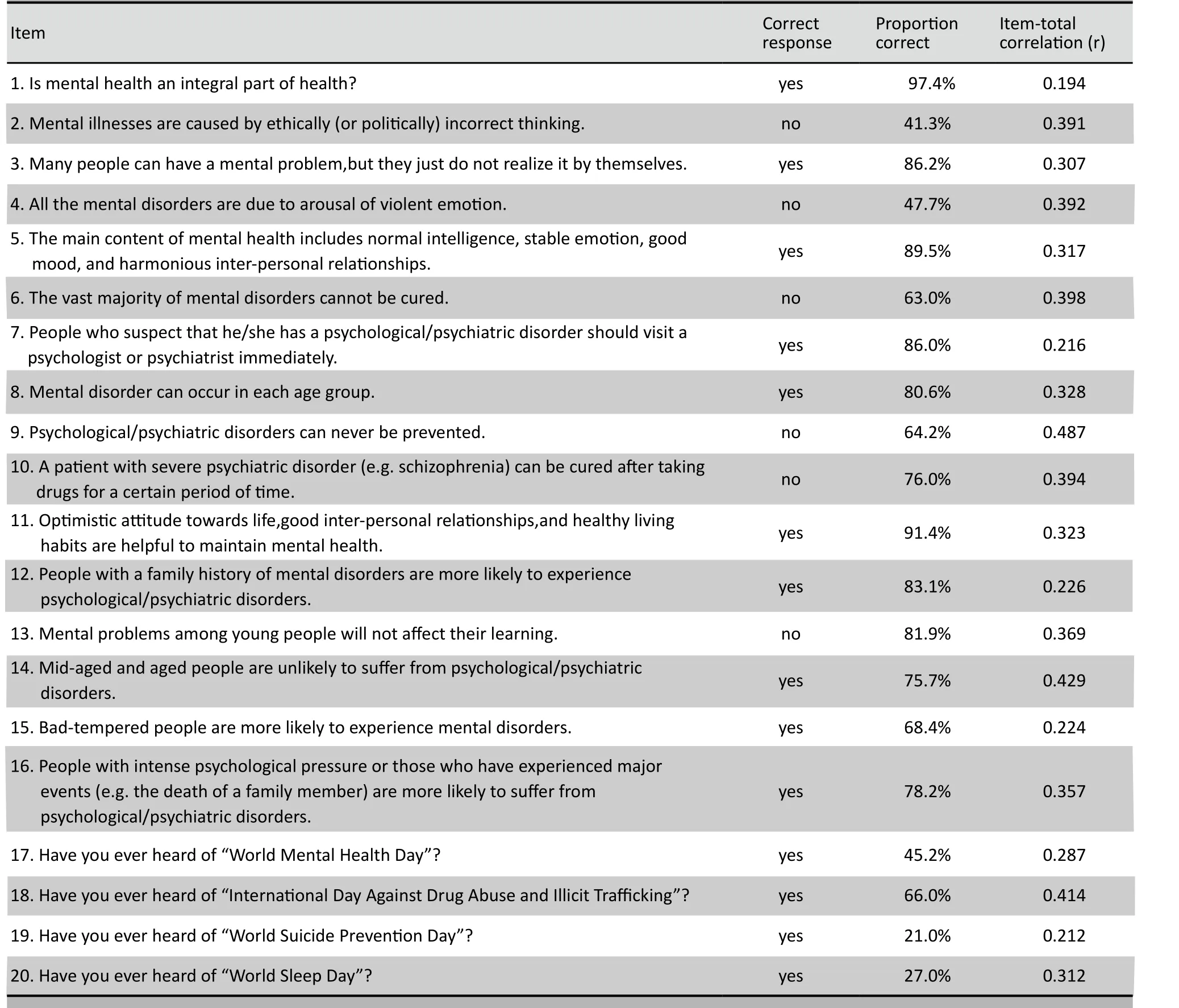
Table 1. Proportion of 1563 community-resident respondents from Changsha, China who correctly answered 20 items on a mental health literacy survey
3. 1 Correct-response rate
The overall mean (SD) proportion of correct responses in the 1,563 validly completed surveys was 68.5% (46.4%). As shown in Table 1 the items that were most likely to be answered correctly were “Is mental health an integral part of health?” (item 1) and “An optimistic attitude towards life, good inter-personal relationships, and healthy living habits are helpful to maintain mental health” (item 11). Items with the lowest correct response rates were “Have you ever heard of ‘World Suicide Prevention Day’? ”(item 19)and “Have you ever heard of ‘World Sleep Day’?” (item 20). More than half of the respondents thought mental illnesses were caused by ethically incorrect thinking(item 2) or arousal of violent emotions (item 4).
3. 2 Relationship of demographic characteristics and level of mental health literacy
Table 2 shows the mean correct response rate for different demographic groups of subjects. There are statistically significant differences in the proportion of correct responses by gender, age, location of residence(urban vs rural), marital status and type of employment.The proportion of correct responses had a negative correlation with age (r=-0.21; p<0.001) and a positive correlation with level of education (r=0.28, p<0.001).As shown in Table 3, after entering all these variables in a stepwise multiple regression analysis the factors that were independently related to the level of mental health literacy included level of education, age and occupation. Agricultural workers and factory workers had a lower level of mental health literacy than persons in other occupations. After controlling for these three factors, gender, marital status and urban versus rural residence was not independently related to mental health literacy.
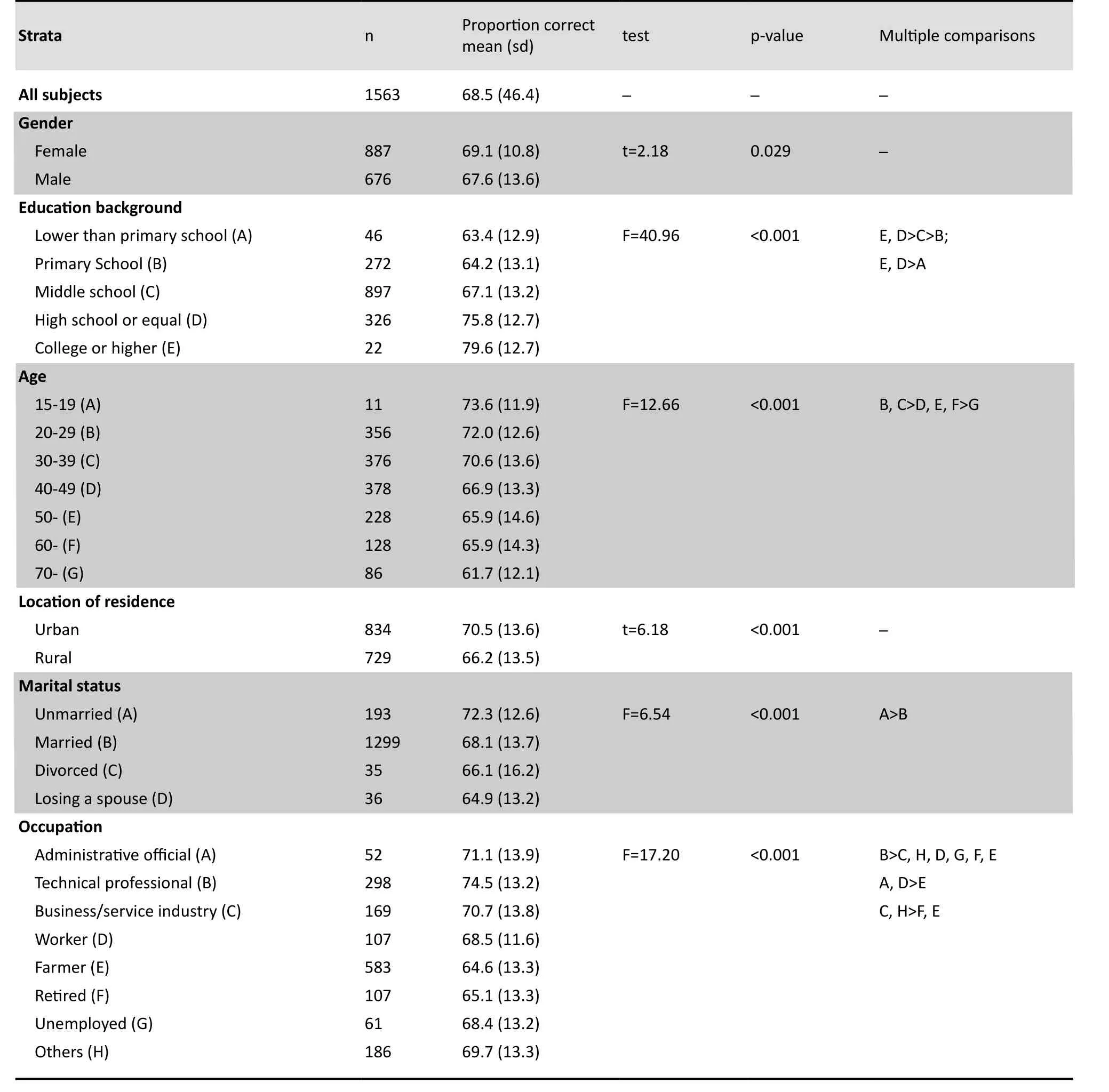
Table 2. Mean (SD) proportion of correct responses to a 20-item questionnaire about mental health literacy among community residents of Changsha,China
3. 3 Internal consistency of the survey instrument
The mean item-total score correlation of the 20 items was relatively low (r=0.33); the range in the correlations was 0.19-0.48 (Table 1). The internal consistency of the 20 items was weak (alpha=0.57) as was that for the four subscales: the four items relating to awareness of the world mental health day, world suicide prevention day, world drug abuse awareness day and world sleep day (items 17-20) had a Cronbachalpha of 0. 57; the seven items related to knowledge of the characteristics of mental illnesses (items 1, 3, 5, 8,11, 13 and 14) had a Cronbach alpha of 0.49; the four items related to the prevention of mental disorders(items 6, 7, 9 and 10) had a Cronbach alpha of 0.42; and the five items related to the causes of mental illness(items 2, 4, 12, 15 and 15) had a Cronbach alpha of 0.27.
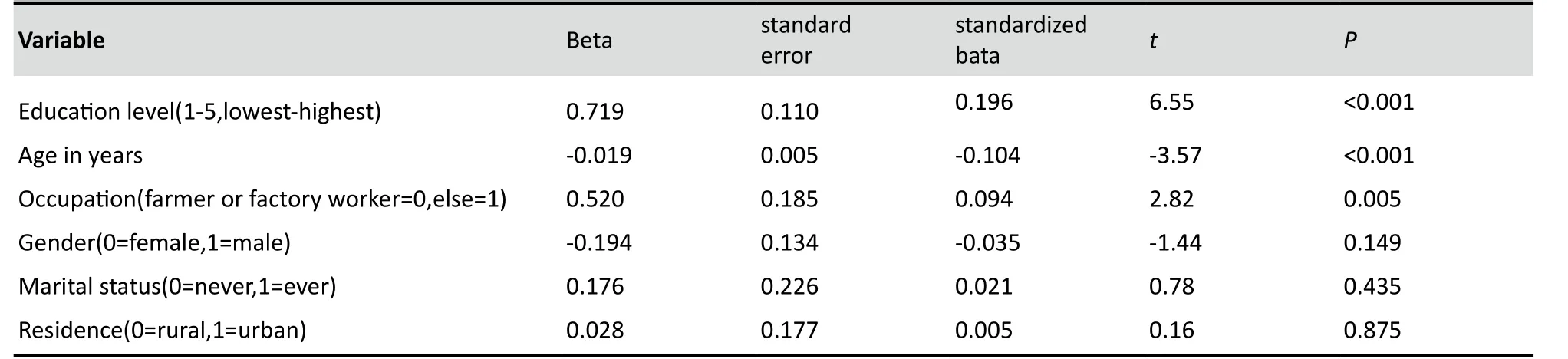
Table 3. Multiple regression results of factors associated with level of mental health literacy
4 Discussion
4. 1 Main findings
In 2002 China’s Ministry of Health and some other Chinese ministries and organizations jointly issued the Chinese Mental Health Work Plan (2002-2010)[7], one of the aims of which was to “widely carry out advocacy and education of mental health among the general public”. The goal of the work plan was to achieve 50% ‘awareness of mental health’ (which was not operationally defined in the document) by 2010. The present survey in Changsha (the capital of Hunan Province) is based on a protocol developed by the China Ministry of Health; it produced data on community members’ knowledge and awareness of mental health and on the prevention of mental disorders. This type of information provides a scientific basis for mental health advocacy and education.
The proportion of correct responses in the current study (68.5%) was higher than that reported in prior mental health literacy studies conducted in Shanghai,Xi’an, Kunming, and other major cities in China[8-13]. But the other studies used different methods and different instruments so its hard to interpret the meaning of the different results. Meaningful cross-community comparisons of mental health literacy requires the use of a common method of assessing this construct. One study among middle school students in Wuhan[6](the capital city in Hubei Province) that did use the same survey instrument as the current study found a mean correct response rate of 68.2% (10.9%); this is not significantly different from the 73.6% (11.9%) correct response rate among 15-19 year old participants in the current study (t=1.06; p=0.289).
A majority of this representative sample of community respondents believed that mental illnesses are caused by ethically incorrect thinking or the arousal of violent emotions. It is somewhat unclear what type of mental illness the subjects were considering when they provided these responses, but it is clear that these misconceptions about the causes of mental illnesses—misconceptions that magnify the stigmatization of the mentally ill—should be a focus of subsequent mental health promotion campaigns. Similarly, most respondents had not heard about World Mental Health Day, World Suicide Prevention Day and World Sleep Day. Promotion efforts to increase awareness of these issues need to broaden to reach different sectors of the community.
Given the relatively large sample, it is not surprising that there were statistically significant differences in the mental health literacy measure between different demographic groups of respondents. Multivariate analysis found that the most robust factors associated with mental health literacy were age, education, and occupation. As expected, individuals who are younger,who have a higher level of education and who do not work as farmers or factory workers have a higher level of mental health literacy. This information is helpful in targeting different types of mental health promotion efforts for different segments of the population.
4. 2 Limitations
There are several questions related to the conduct of the survey and about the survey instrument itself that need to be clarified before one can fully interpret these findings. The survey included individuals who were in the home at the time the interviewer visited the household so the sample may under-represent younger people and males who are more likely to be out of the home working. The test-retest reliability of the survey has not been assessed in adults so the stability of this assessment of respondent mental health literacy is in doubt. In contrast to the relatively good internal consistency of the survey when used with middle school students[6], the low item-total scale correlations(0.19-0.48) and the low alpha values for the total scale and the subscales (0.27-0.57) found in this study with adults suggest that the questions in the subscales are NOT assessing distinct constructs. There may be benefit to conducting exploratory and confirmatory factor analysis to see if there is a more stable set of subscales in the instrument. And there has been no assessment of the concurrent validity of the survey (e.g., relating the survey scores to attitudes about health care-seeking for mental health problems and to stigmatizing beliefs about the mentally ill) so we cannot be certain whether or not this set of items actually captures all the relevant domains of ‘mental health literacy’. Until a reliable and valid instrument is available it will not be possible to conduct the stratified analyses needed to identify the specific content of mental health education efforts that would be most appropriate for different population cohorts.
Another issue that will require further elaboration is the respondents’ concept of what does and does not constitute a ‘mental illness’, a factor that might be quite different for different types of respondents. Many rural and less educated respondents only consider bizarre psychotic behavior as ‘mental illness’, while more educated urban residents may include depression and anxiety disorders under the label of ‘mental illness’.Very few respondents (urban or rural) consider alcohol and substance abuse and dependence a ‘mental illness’.Given the wide range of conditions that respondents could potentially consider a mental illness, differences in the responses about the causes and prevention of mental illnesses will be very difficult to interpret. In future such surveys must initially clearly circumscribe the definition of ‘mental illness’ for respondents prior to asking about their beliefs about the causes and prevention of mental illness.
4. 3 Implications
Improving mental health literacy in the community is one of the cornerstones of improving mental health both in high-income and in low- and middle-income countries. Developing reliable methods of assessing mental health literacy is, however, a complicated process that must take into consideration a wide range of cultural, social, economic and medical factors.The survey instrument developed by the Ministry of Health in China is a first attempt to employ a consistent method of making this type of assessment nationally.The ultimate goal is to use the results of the survey to develop and test mental health promotion campaigns with different messages for different target groups; but the current survey instrument will probably require further revision before it can be used in this way.
Acknowledgments
We are grateful for the kind assistance provided by the Centers for Disease Control of Furong, Yuelu,Wangcheng, and Ningxiang and by the community health-care centers dealing with chronic diseases and mental disorders in these districts and counties.
Funding
The study was funded from the public health budget of the Changsha Centers for Disease Control.
Conflict of interest
The authors report no conflict of interest related to this paper.
1. Kelly CM, Jorm AF, Wright A. Improving mental health literacy as a strategy to facilitate early intervention for mental disorders.Med J Aust, 2007, 187(7 Suppl):S26-30.
2. Jorm AF. Mental health literacy:Empowering the community to take action for better mental health. Am Psychol, 2011,PMID:22040221.
3. Evans-acko S, Little K, Meltzer H, Rose D, Rhydderch D, Henderson C, Thornicroft G. Development and psychometric properties of the Mental Health Knowledge Schedule. Can J Psychiatry, 2010,55(7):440-48.
4. Swami V, Papanicolaou A, Furnham A. Examining mental health literacy and its correlates using the overclaiming technique. Br J Psychol, 2011, 102(3):662-75. doi:10. 1111/j. 2044-295. 2011.02036.
5. China Ministry of Health. Mental Health Indicator Survey/Assessment Protocol. http://www. gov. cn/gzdt/2010-03/08/content_1550552. htm. Accessed November 11, 2011.
6. Zhong BL, Chen HH, Xiao SY, Zhou L, Zhang JF, Xu HM. Reliability and validity of Mental Health Knowledge Questionnaire for middle school students. Chinese Journal of School Health, 2011,32(1):49-50. (in Chinese)
7. Ministries of Health, Public Security, Civil Affairs, and CDPF.National Mental Health Plan. 2002-2010.
8. Meng GR, Li XH, Yao XW, Zhu ZQ. A survey of mental health awareness among 1783 Shanghai citizen. Shanghai Arch Psychiatry, 2005, 17(1):19-20. (in Chinese)
9. Meng GR, Yao XW, Zhu ZQ, Zhang MY. A survey of mental health awareness among Shanghai citizen:2697 questionnaires analysis.Shanghai Arch Psychiatry, 2002, 14(1):56-57. (in Chinese)
10. Shi JG, Luo YY, Tao MZ. Survey on the Mental Health Awareness among Xi’an residents. Chinese Journal of Behavioral Science,2008, 17(4):367-368. (in Chinese)
11. Jiang YH, Bo SM, Shen J, Kang H, Zhang H. Survey on Mental Health Awareness among the general public in minhang district,Shanghai. Shanghai Journal of Preventive Medicine, 2007,19(6):281-282. (in Chinese)
12. Han HQ, Zeng Y, Zhao XD, Liu CP, Xie B. Survey on Mental Health Awareness among the general public in Kunming. China Journal of Health Psychology, 2008, 16(11):1274-1277. (in Chinese)
13. Tian Mei, Zhang Y, Bai Z, Yang CR, Liu YF, Li HMl. Survey on Mental Health Awareness among urban and rural residents. China Journal of Health Psychology, 2011, 19(2):144-146. (in Chinese)
长沙市普通人群的精神卫生知晓情况
彭 元 王晓玲 李平非 刘 鲲
长沙市疾病预防控制中心410001。通信作者:彭元,电子信箱:pengyuanchangsha@sina.com
目的评定长沙市公众精神卫生和精神疾病预防知识的知晓情况。
方法采用多阶段整群随机抽样方法,选取长沙市辖区随机抽取的2个城市社区和2个农村社区的1 660户家庭。从15岁及以上的家庭成员中随机抽取1人进行访谈,完成卫生部推荐的精神卫生知晓率标准问卷(20项)调查。
结果1 563人完成有效问卷调查,其中男性676人,女性887人,平均年龄(标准差)为41.9(15.9)岁。平均(标准差)应答正确率为68.5%(46.4%),城市社区平均(标准差)应答正确率[70.5%(13.6%)]高于农村社区应答正确率[66.2%13.5%)](t=6.18,p<0.001)。 正确应答率与年龄负相关(r=-0.21,p<0.001),与文化程度正相关(r=0.28,p<0.001),与职业和婚姻状态的差异呈多样相关性。采用逐步回归分析发现文化程度、年龄和职业(农民或工人与其他职业比较)为精神卫生知晓率的独立相关因素。问卷20个条目总体内部一致性及4个分量表的内部一致性偏低 (alpha=0.27~0.57)。
结论长沙市普通居民精神卫生知识总体知晓率相对较高,但有些方面仍需提高,特别是对于精神疾病病因的认识。公众精神卫生知识的知晓能力随人口学特征不同而有较大差异,因此对不同人群进行特定的精神卫生教育可有效地提高社区居民的精神卫生知识知晓率。今后需修订调查问卷,提高信、效度和内部一致性。
普通人群 精神卫生 精神疾病 知晓率 调查
10.3969/j.issn.1002-0829.2011.06.005
Centers for Disease Control and Prevention, Changsha 410001, China
*Correspondence: pengyuanchangsha@sina.com
(received: 2011-06-28; accepted: 2011-11-02)
猜你喜欢
杂志排行

上海精神医学的其它文章
- 苯丙胺类兴奋剂所致精神障碍的临床诊治问题
- Cost of treating medical conditions in psychiatric inpatients in Zhejiang, China
- Relationship between blood levels and clinical efficacy of two different formulations of venlafaxine in female patients with depression
- Eight-week follow-up of depressive and anxiety symptoms in patients with chronic hepatitis B, patients with hepatitis B cirrhosis and normal control subjects
- · In This Issue ·
- 创伤与噩梦的相关研究进展