Surgical therapy and prognosis of sarcomatoid carcinoma of the gallbladder
2010-12-14ZhenHuaHuZhiWeiLiLiangShenMinZhangandShuSenZheng
Zhen-Hua Hu, Zhi-Wei Li, Liang Shen, Min Zhang and Shu-Sen Zheng
Hangzhou, China
Surgical therapy and prognosis of sarcomatoid carcinoma of the gallbladder
Zhen-Hua Hu, Zhi-Wei Li, Liang Shen, Min Zhang and Shu-Sen Zheng
Hangzhou, China
(Hepatobiliary Pancreat Dis Int 2010; 9: 175-179)
gallbladder neoplasm;sarcomatoid carcinoma;surgical therapy;prognosis
Introduction
Primary gallbladder carcinoma is a malignant neoplasm with an incidence of 1.2 cases per 100 000 people each year. Its occurrence increases with age,particularly in women.[1]It is the fi fth most common cancer of the gastrointestinal tract, and the most common malignancy in the biliary tract.[2]Adenocarcinoma is the most common type of gallbladder neoplasm whereas sarcomatoid carcinoma is rarely seen in the gallbladder.Sarcomatoid carcinoma possesses malignant epithelial and sarcomatous components at the same time, and it has been found in many organs including the gallbladder,lung, kidney, uterus and breast.[3-5]To our knowledge, only 46 cases with sarcomatoid carcinoma of the gallbladder have been reported in the English-language literature,[6-32]mostly case reports and few articles on further analysis of the behavior and prognosis of the tumor.
Therapeutic methods of the tumor include surgery,chemotherapy, radiotherapy, and medical treatment. If possible, however, the patients with this carcinoma are usually treated by either radical or palliative surgery.In general, conservative treatments are thought to be unfavourable to the tumor.[20]Therefore, surgery is considered as the only approach.
To understand the manifestations and surgical outcome of the tumor, we reviewed the data of 56 patients(10 patients in our center and 46 reported elsewhere).
MethodsPatients
From 2004 to 2009, ten patients were pathologically diagnosed with sarcomatoid carcinoma of the gallbladder and received surgical treatment at our center. The median age was 67 years (inter-quartile range 59-74 years).
Surgical procedures
Surgery was palliative or radical. The palliative surgery included exploratory laparotomy, simply cholecystectomy,bile drainage of tumor-induced obstruction or biopsy.The radical one referred to extensive resection of primary tumor and peripheral metastatic lymph nodes or tissues.
Pre-operative examination and TNM staging
Before operation, the patients were subjected to routine examinations including review of case history,physical examination, laboratory tests, and imagings such as abdominal sonography, CT scan, magnetic resonance imaging (MRI) or endoscopic retrograde cholangiopancreaticography (ERCP). Tumor-node-metastasis (TNM)was staged according to the 2002 TNM classi fi cation for gallbladder carcinoma revised by the American Joint Committee on Cancer (AJCC).[33]
Summary of international literatures
We analyzed the data of 46 patients reported previously[6-32]and the data of our 10 patients who received surgery for sarcomatoid carcinoma of the gallbladder.
Statistical analysis
The descriptive variables were expressed as median value (inter-quartile range), and the overall survival rates were calculated using the Kaplan-Meier method and compared using the log-rank test. SPSS version 15.0 statistic software (SPSS Inc, Chicago, IL) was used for data analysis and a P value less than 0.05 was considered statistically signi fi cant.
ResultsCharacteristics of patients
The gender, age, clinical manifestations, operative methods and TNM staging of the 10 patients are shown in Table. Abdominal pain, either chronic or acute, was felt in the 10 patients; however, tumor mass was dif fi cult to be palpated. In only 5 patients the tumor mass was felt by surgeons before operation. Seven patients with multiple stones in the gallbladder were associated with cholelithiasis and cholecystitis. The median size of sarcomatoid carcinoma of the gallbladder was 5.2 cm(inter-quartile range 3.1-7.9 cm) in the 10 patients.
TNM staging and surgical procedure
TNM staging is used to de fi ne the progress of malignant tumor. In our series, none was in stage Ⅰ, 8 in stage Ⅱ (2 in stage ⅡA and 6 in stage ⅡB respectively),1 in stage Ⅲ and 1 in stage Ⅳ (Table). The ten patients had lymph node metastasis or distant organ metastasis.Abdominal CT revealed a mass suspicious of malignant neoplasm of the gallbladder and enlarged lymph nodes in the retroperitoneum (Fig. 1). The stage Ⅳ patient received palliative cholecystectomy, and the other 9 patients underwent radical surgery of tumor involved tissues observed by surgeons. The operation consisted of resection of primary gallbladder tumor, resection of involved liver tissue, resection of extrahepatic biliary tract, clearance of the portal hepatis and retroperitoneal lymph nodes. TNMstaging is important to assess the severity of carcinoma,in addition to histological examination. Pathologically,the epithelial component of adenocarcinoma could be noted in 7 of the 10 patients while others the epithelial component of squamous cell carcinoma or both. The histological appearance of sarcomatoid carcinoma of the gallbladder is shown in Fig. 2.
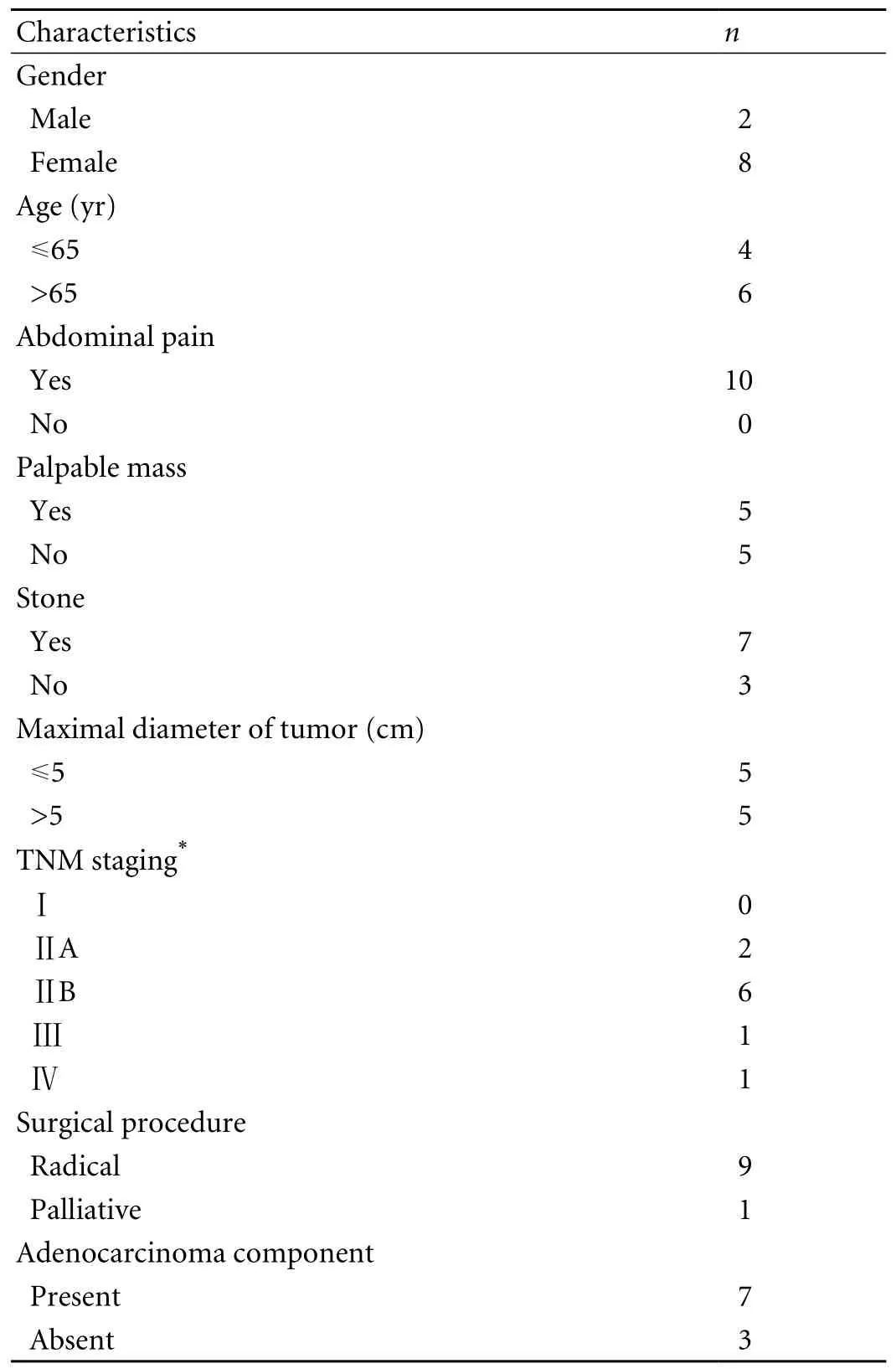
Table. Clinical characteristics of the 10 patients
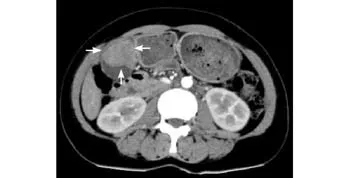
Fig. 1. Abdominal computed tomography reveals a mass lesion of the gallbladder (arrows).
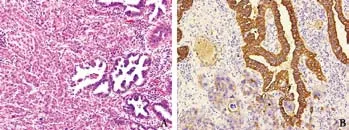
Fig. 2. A: Histological appearance of the sarcomatoid carcinoma of the gallbladder (hematoxylin-eosin, original magni fi cation ×200).B: focal staining of immunohistochemistry to anti-cytokeratin(original magni fi cation ×200).
Analysis of prognosis
In this series, the median survival time was 9 months (inter-quartile range 6-12 months). Three patients were alive during the follow-up period; however,two of them had tumor recurrence: one received another resection of the metastatic tumor, and the other was given conservative treatment.
Global data analysis
We identi fi ed 56 patients altogether with sarcomatoid carcinoma of the gallbladder, with complete data on age,operative modes and survival time. The female to male ratio was 5∶2, with the median age of morbidity was 66 years (inter-quartile range 61-74.5 years). The median size of gallbladder carcinoma was 8.0 cm (inter-quartile range 5-10 cm) (according to available data). Totally, the median survival time was 5.5 months (inter-quartile range 2.5-10 months). The survival time of the patients after radical surgery was signi fi cantly longer than that of those after palliative surgery, with the median values being 6 months (inter-quartile range 3-12 months) and 4 months (inter-quartile range 2-8 months), respectively(P=0.031) (Fig. 3).

Fig. 3. Cumulative survival rate of the patients undergoing radical and palliative surgery.
Discussion
Sarcomatoid carcinoma of the gallbladder is an extremely rare malignancy in the biliary tract. Sporadic case reports on this tumor concentrated on the pathological changes.Those with sarcomatoid carcinoma of the gallbladder presented with the following symptoms: abdominal pain, fever, jaundice, nausea, vomiting, and poor appetite.[6-32]Most of the patients were also diagnosed with cholelithiasis with multiple stones detected by sonography.
For the diagnosis of the tumor, abdominal sonography, CT scan and MRI are essential. Sonography is sensitive to show an abnormal echo of diffusion,localization or irregulation of the gallbladder wall. Since the characteristics of sarcomatoid carcinoma of the gallbladder and adenocarcinoma are quite similar, they are dif fi cult to be distinguished by imaging.[11]Imaging is helpful to proceed TNM staging and select operative mode. In our series, all patients were diagnosed with gallbladder neoplasm pre-operatively and TNM staging was done after operation. Therefore, pre-operative imaging is critical to surgeons in decision-making.
TNM staging is a synthetic method evaluating the tumor and its stages, which is important for the prognosis of gallbladder neoplasm.[34]The median size of gallbladder carcinoma in the 56 patients was 8.0 cm(inter-quartile range 5-10 cm). Using the 2002 TNM staging revised by AJCC, we found 8 of our 10 patients were in late stages (stage ⅡB, stage Ⅲ and stage Ⅳ).
Pathologically, sarcomatoid carcinoma is composed of both epithelial and mesenchymal components.Many case reports emphasized the constructions of sarcomatoid carcinoma.[16-19]Zhang et al[32]analyzed data in terms of pathological components, with regard to epithelial constituent they grouped 79.2% as cases of adenocarcinoma, 9.4% as cases of squamous cell carcinoma, and 11.3% as cases of a mixture of both. With regard to mesenchymal constituent, 44.6% were sorted as cases of spindle cells, 10.7% as cases of chondroid, 8.9%as cases of rhabdomyoid, 5.4% as cases of osteoid, and 30.4% as cases of other histopathological types. In our series, epithelial components of the patients were mostly adenocarcinoma like.
As to solid tumor, the fi rst choice of therapy is always surgical resection. Surgery is an effective treatment for sarcomatoid carcinoma of the gallbladder. Neither radiotherapy nor chemotherapy contributes to the survival rate.[27]However, due to the high malignancy of sarcomatoid carcinoma, many patients are diagnosed with the tumor at late stage, for instance, stage ⅡB or stage Ⅲ, and even stage Ⅳ. Even after extensive resection of the visible tumor-involved tissues, some patients still may die shortly after the surgery due to tumor recurrence.Liu et al[20]compared the survival rate of patients with sarcomatoid carcinoma of the gallbladder and adenocarcinoma, and found that the latter patients lived longer. We analyzed the data from the 46 patients[6-32]and our 10 patients, the inter-quartile range of survival time was 2.5 to 10 months, with a median value of 5.5 months.In our series, the longest survival time was 43 months,and this patient is presently alive and relapse-free. Two patients unfortunately have been detected with tumor recurrence or metastasis. We found that the survival time of patients undergoing radical surgery was signi fi cantly longer than that of those receiving palliative surgery.
By statistical analysis of data on diagnosis and treatment of sarcomatoid carcinoma of the gallbladder,we suggest that once sarcomatoid carcinoma of the gallbladder is suspected, it is absolutely necessary to inform the patient and his/her relatives of the aggressive biological behavior of the tumor and its prognosis. Thus surgeons could decide radical surgery as quickly as possible.
In conclusion, the biological behavior of sarcomatoid carcinoma of the gallbladder is extremely cacoethic and the prognosis is always desolate. Nevertheless,radical surgery is still the fi rst choice for patients with sarcomatoid carcinoma of the gallbladder if possible.
Funding: This study was supported by grants from the Investigative Foundation of Medical Science of Zhejiang Province (2008B050).
Ethical approval: This study was approved by the Ethics Committee of the hospital.
Contributors: HZH and ZSS proposed the study. HZH and LZW wrote the fi rst draft. LZW analyzed the data. All authors contributed to the design and interpretation of the study and to further drafts.ZSS is the guarantor.
Competing interest: No bene fi ts in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Albores-Saavedra J, Cruz-Ortiz H, Alcantara-Vazques A,Henson DE. Unusual types of gallbladder carcinoma. A report of 16 cases. Arch Pathol Lab Med 1981;105:287-293.
2 Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics,2002. CA Cancer J Clin 2005;55:74-108.
3 Reuter VE. Sarcomatoid lesions of the urogenital tract. Semin Diagn Pathol 1993;10:188-201.
4 Koss MN, Hochholzer L, Frommelt RA. Carcinosarcomas of the lung: a clinicopathologic study of 66 patients. Am J Surg Pathol 1999;23:1514-1526.
5 Inoshita S. Phyllodes tumor (cystosarcoma phyllodes) of the breast. A clinicopathologic study of 45 cases. Acta Pathol Jpn 1988;38:21-33.
6 Mehrotra TN, Gupta SC, Naithani YP. Carcino-sarcoma of the gall bladder. J Pathol 1971;104:145-148.
7 Higgs WR, Mocega EE, Jordan PH Jr. Malignant mixed tumor of the gallbladder. Cancer 1973;32:471-475.
8 Mansori KS, Cho SY. Malignant mixed tumor of the gallbladder. Am J Clin Pathol 1980;73:709-711.
9 Aldovini D, Piscioli F, Togni R. Primary malignant mixed mesodermal tumor of the gallbladder. Report of a case and critical review of diagnostic criteria. Virchows Arch A Pathol Anat Histol 1982;396:225-230.
10 Von Kuster LC, Cohen C. Malignant mixed tumor of the gallbladder: report of two cases and a review of the literature.Cancer 1982;50:1166-1170.
11 Born MW, Ramey WG, Ryan SF, Gordon PE. Carcinosarcoma and carcinoma of the gallbladder. Cancer 1984;53:2171-2177.
12 Lumsden AB, Mitchell WE, Vohman MD. Carcinosarcoma of the gallbladder: a case report and review of the literature. Am Surg 1988;54:492-494.
13 Nishihara K, Tsuneyoshi M. Undifferentiated spindle cell carcinoma of the gallbladder: a clinicopathologic, immunohistochemical, and fl ow cytometric study of 11 cases. Hum Pathol 1993;24:1298-1305.
14 Fagot H, Fabre JM, Ramos J, Laffay V, Guillon F, Domergue J, et al. Carcinosarcoma of the gallbladder. A case report and review of the literature. J Clin Gastroenterol 1994;18:314-316.15 Nakagawa T, Yamakado K, Takeda K, Nakagawa T. An ossifying carcinosarcoma of the gallbladder: radiologic fi ndings. AJR Am J Roentgenol 1996;166:1233-1234.
16 Kim MJ, Yu E, Ro JY. Sarcomatoid carcinoma of the gallbladder with a rhabdoid tumor component. Arch Pathol Lab Med 2003;127:e406-408.
17 Takahashi Y, Fukushima J, Fukusato T, Shiga J. Sarcomatoid carcinoma with components of small cell carcinoma and undifferentiated carcinoma of the gallbladder. Pathol Int 2004;54:866-871.
18 Huguet KL, Hughes CB, Hewitt WR. Gallbladder carcinosarcoma: a case report and literature review. J Gastrointest Surg 2005;9:818-821.
19 Sodergren MH, Silva MA, Read-Jones SL, Hubscher SG,Mirza DF. Carcinosarcoma of the biliary tract: two case reports and a review of the literature. Eur J Gastroenterol Hepatol 2005;17:683-685.
20 Liu KH, Yeh TS, Hwang TL, Jan YY, Chen MF. Surgical management of gallbladder sarcomatoid carcinoma. World J Gastroenterol 2009;15:1876-1879.
21 Agarwal T, Jain M, Goel A, Visayaragavan P, Gupta RK.Carcinosarcoma of the gallbladder. Indian J Pathol Microbiol 2009;52:244-245.
22 Appelman HD, Coopersmith N. Pleomorphic spindle-cell carcinoma of the gallbladder. Relation to sarcoma of the gallbladder. Cancer 1970;25:535-541.
23 Guo KJ, Yamaguchi K, Enjoji M. Undifferentiated carcinoma of the gallbladder. A clinicopathologic, histochemical, and immunohistochemical study of 21 patients with a poor prognosis. Cancer 1988;61:1872-1879.
24 Ishihara T, Kawano H, Takahashi M, Yokota T, Uchino F,Matsumoto N, et al. Carcinosarcoma of the gallbladder. A case report with immunohistochemical and ultrastructural studies. Cancer 1990;66:992-997.
25 Rys J, Kruczak A, Iliszko M, Babinska M, Wasilewska A,Limon J, et al. Sarcomatoid carcinoma (carcinosarcoma) of the gallbladder. Gen Diagn Pathol 1998;143:321-325.
26 Eriguchi N, Aoyagi S, Hara M, Hashino K, Imamura M, Sato S, et al. A so-called carcinosarcoma of the gallbladder in a patient with multiple anomalies--a case report. Kurume Med J 1999;46:175-179.
27 Ajiki T, Nakamura T, Fujino Y, Suzuki Y, Takeyama Y, Ku Y, et al. Carcinosarcoma of the gallbladder with chondroid differentiation. J Gastroenterol 2002;37:966-971.
28 Hotta T, Tanimura H, Yokoyama S, Ura K, Yamaue H. Socalled carcinosarcoma of the gallbladder; spindle cell carcinoma of the gallbladder: report of a case. Surg Today 2002;32:462-467.
29 Kubota K, Kakuta Y, Kawamura S, Abe Y, Inamori M,Kawamura H, et al. Undifferentiated spindle-cell carcinoma of the gallbladder: an immunohistochemical study. J Hepatobiliary Pancreat Surg 2006;13:468-471.
30 Uzun MA, Koksal N, Gunerhan Y, Celik A, Gunes P.Carcinosarcoma of the gallbladder: report of a case. Surg Today 2009;39:168-171.
31 Shimada K, Iwase K, Aono T, Nakai S, Takeda S, Fujii M,et al. Carcinosarcoma of the gallbladder producing alphafetoprotein and manifesting as leukocytosis with elevated serum granulocyte colony-stimulating factor: report of a case. Surg Today 2009;39:241-246.
32 Zhang L, Chen Z, Fukuma M, Lee LY, Wu M. Prognostic signi fi cance of race and tumor size in carcinosarcoma of gallbladder: a meta-analysis of 68 cases. Int J Clin Exp Pathol 2008;1:75-83.
33 American Joint Committee on Cancer. AJCC cancer staging manual, 6th ed. New York: Springer; 2002:145-149.
34 Fong Y, Jarnagin W, Blumgart LH. Gallbladder cancer:comparison of patients presenting initially for de fi nitive operation with those presenting after prior noncurative intervention. Ann Surg 2000;232:557-569.
BACKGROUND: Sarcomatoid carcinoma of the gallbladder is rare and its characteristics are poorly understood. This study aimed to understand the behavior and prognosis of sarcomatoid carcinoma of the gallbladder as well as its clinical manifestations and survival rate of patients after radical or palliative surgery,and to review the reported data worldwide and our 10 patients.
METHODS: From 2004 to 2009, ten patients were pathologically diagnosed with sarcomatoid carcinoma of the gallbladder and underwent operation at our center. These characteristics, clinical presentations, tumor-node-metastasis (TNM) staging, surgical modes, and prognosis were reviewed, retrospectively. We collected the data of 46 patients reported in the English-language literature worldwide and analyzed the survival with ours. The survival rate was estimated using the Kaplan-Meier method, and was compared using the log-rank test.
RESULTS: The median age of the 10 patients was 67 years(inter-quartile range 59-74 years), and the size of tumor interquartile ranged from 3.1 to 7.9 cm. In this series, 9 patients
radical surgery, and one undewent palliative surgery.There was no surgical mortality, and one patient underwent a second operation because of liver metastasis. The median survival time of the patients was 9 months (inter-quartile range 6-12 months), with 3 patients still being alive until follow-up; however, two patients had tumor recurrence. The data from the 56 patients (10 patients in our series and 46 reported elsewhere) statistically indicated that the median age was 66 years (inter-quartile range 61-74.5 years) and the overall median survival was 5.5 months (inter-quartile range 2.5-10 months). The survival time in the patients undergoing radical surgery (n=42) was signi fi cantly longer than that in the patients undergoing palliative surgery (n=14) (P=0.031).CONCLUSIONS: The survival of the patients with sarcomatoid carcinoma of the gallbladder is poor. Some patients may die shortly after the surgery because of recurrence or metastasis.However, radical surgery is still necessary if possible.
Author Af fi liations: Division of Hepatobiliary and Pancreatic Surgery;Key Laboratory of Combined Multi-organ Transplantation, Ministry of Public Health; and Key Laboratory of Organ Transplantation Zhejiang Province, First Af fi liated Hospital, Zhejiang University School of Medicine,Hangzhou 310003, China (Hu ZH, Li ZW, Shen L, Zhang M and Zheng SS)Corresponding Author: Shu-Sen Zheng, MD, PhD, FACS, Key Laboratory of Combined Multi-organ Transplantation, Ministry of Public Health, First Af fi liated Hospital, Zhejiang University School of Medicine, Hangzhou 310003, China (Tel: 86-571-87236570; Fax: 86-571-87236884; Email:shusenzheng@zju.edu.cn)
© 2010, Hepatobiliary Pancreat Dis Int. All rights reserved.
December 25, 2009
Accepted after revision March 15, 2010
杂志排行

Hepatobiliary & Pancreatic Diseases International的其它文章
- Delayed hepatocarcinogenesis through antiangiogenic intervention in the nuclear factor-kappa B activation pathway in rats
- Effect of blueberry on hepatic and immunological functions in mice
- Impact of human leukocyte antigen matching on hepatitis B virus recurrence after liver transplantation
- Prognostic models for acute liver failure
- Proteomic analysis of differentially expressed proteins involving in liver metastasis of human colorectal carcinoma
- Protective effects of MCP-1 inhibitor on a rat model of severe acute pancreatitis