深度学习图像重建算法在80 kV管电压下冠状动脉CT血管造影中的应用
2024-10-19向青曹键罗涛朱璇覃杰郭亚豪黎超

【摘要】 目的 探讨80 kV深度学习图像重建(DLIR)算法在冠状动脉CT血管造影(CCTA)中的应用价值。方法 将接受心脏CCTA检查的60例患者按扫描方案分为100 kV组(A组,n = 30)和80 kV组(B组,n = 30)。A组采用60% 权重自适应统计迭代重建-Veo(ASIR-V)算法(A-AV60)、DLIR算法(A-DLIR);B组采用DLIR算法(B-DLIR)。记录2组的CT容积剂量指数(CTDIvol)、剂量长度乘积(DLP),计算有效辐射剂量(ED)。将感兴趣区(ROI)分别置于主动脉根(AR)、左前降支(LAD)、左回旋支(LCX)、右冠状动脉(RCA)及同层胸前脂肪区域,记录各ROI的CT值、噪声值,计算信噪比(SNR)和对比噪声比(CNR)。主观评价2组经2代冻结技术后的原始轴位、曲面重建(CPR)、容积再现(VR)重建和最大强度投影(MIP)重建,并且对2组图像进行主观质量评价。结果 B组较A组ED降低45.14%。B-DLIR中AR、LAD、LCX、RCA的CT值均高于A-AV60及A-DLIR,比较差异均有统计学意义(P均< 0.001)。A-DLIR与B-DLIR相比,AR、LAD、LCX的噪声值相近,仅在RCA中比较差异有统计学意义(P < 0.05);A-DLIR与B-DLIR的噪声值均小于A-AV60,比较差异均有统计学意义(P均< 0.001)。A-DLIR与B-DLIR中AR、LAD、LCX、RCA的SNR、CNR相近,均高于A-AV60(P均< 0.05)。B-DLIR主观图像质量平均分高于A-AV60(P < 0.05),但低于A-DLIR(P < 0.05)。A-DLIR与B-DLIR的清晰度、伪影、小分支可见度比较差异均无统计学意义(P均> 0.05)。结论 在CCTA检查中,采用80 kV DLIR算法有助于获得质量更优的图像,进一步提高诊断效能,且可减少有效辐射剂量。
【关键词】 深度学习图像重建;自适应统计迭代重建;冠状动脉CT血管造影;信噪比;对比噪声比
Application of CCTA under 80 kV tube voltage based on deep learning image reconstruction algorithm
XIANG Qing, CAO Jian, LUO Tao, ZHU Xuan, QIN Jie, GUO Yahao , LI Chao
(Department of Radiology, the Third Affiliated Hospital of Sun Yat-sen University, Guangzhou 510630, China)
Corresponding author: GUO Yahao, E-mail: guoyh65@mail.sysu.edu.cn
【Abstract】 Objective To explore the application value of 80 kV deep learning image reconstruction (DLIR) algorithm in coronary CT angiography (CCTA). Methods Sixty patients who underwent CCTA were divided into two groups based on the scanning protocols: 100 kV group (Group A, n = 30) and 80 kV group (Group B, n = 30). In Group A, 60% ASIR-V (A-AV60) and DLIR high-level reconstruction (A-DLIR) was adopted. In Group B, DLIR high-level reconstruction (B-DLIR) was employed. The CT volumetric dose index (CTDIvol) and the dose length product (DLP) were recorded in both groups, and the effective dose (ED) was calculated. Regions of interest (ROI) were placed in the aortic root (AR), left anterior descending coronary artery (LAD), left circumflex coronary artery (LCX), right coronary artery (RCA), and the same-layer pectoral fat area. The CT values and noise values of each ROI were recorded. Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) were calculated. Subjective evaluation was performed on the original axis, curved planar reconstruction (CPR), volume rendering (VR), and maximum intensity projection (MIP) reconstructions after the second-generation freeze technology (Snapshot Freeze 2, SSF-2), and the images in two groups were subject to subjective image quality evaluation. Results The ED in Group B was reduced by 45.14% compared to that in Group A. The CT values for AR, LAD, LCX, and RCA in the B-DLIR were higher than those in the A-AV60 and A-DLIR groups, and the differences were statistically significant (all P < 0.001). The noise values for AR, LAD and LCX were similar, whereas statistical significance was observed in RCA between the A-DLIR and B-DLIR groups (P < 0.05). The noise values in the A-DLIR and B-DLIR groups were smaller than that in the A-AV60 group, and the differences were statistically significant (both P < 0.001). The SNR and CNR for AR, LAD, LCX and RCA were similar between the A-DLIR and B-DLIR groups, which were higher than those in the A-AV60 group (all P < 0.05). The average subjective evaluation score of image quality in the B-DLIR group was higher than that in the A-AV60 group (P < 0.05), whereas lower than that in the A-DLIR group (P < 0.05). There were no significant differences in clarity, artifact and small branch visibility between the A-DLIR and B-DLIR groups (all P > 0.05). Conclusions During CCTA, the 80 kV DLIR algorithm contributes to yielding high-quality images, further improves the diagnostic efficiency and reduces the irradiation dose.
【Key words】 Deep learning image reconstruction; Adaptive statistical iterative reconstruction ; Coronary CT angiography; Signal-to-noise ratio; Contrast-to-noise ratio
动脉粥样硬化是一种发病率和病死率均非常高的全身性疾病,最常见表现为冠状动脉疾病 (coronary artery disease,CAD)[1]。数字减影血管造影(digital subtraction angiography,DSA)是诊断动脉粥样硬化的金标准,但具有一定的创伤性,患者需要长时间暴露于射线,且操作方法复杂,费用较高[2]。冠状动脉计算机断层扫描血管造影(coronary computed tomographic angiogram,CCTA)具有侵入性小、检查时间短以及可用性、准确性高的优点[3],已经成为诊断心血管疾病的主要手段[4-6]。目前已经出现了几种迭代重建(iterative reconstruction,IR)算法可以有效降低图像噪声,提高图像质量。现阶段最常用的自适应统计迭代重建-Veo(adaptive statistical iterative reconstruction-Veo,ASIR-V)算法在较低辐射剂量下可提供比传统迭代重建更好的图像质量[7-8]。但仍存在与 ASIR算法相同的不足,包括高权重下改变噪声纹理,图像具有蜡状、塑料外观或点状不自然的外观[9]。
近年来,一种基于深度学习图像重建(deep learning image reconstruction,DLIR)的算法出现,深度学习是机器学习的一个子集,两者均为人工智能(artificial intelligence,AI)的子集。机器学习可以从数据、模式和特征中学习,以便在最少的人工干预下做出决策;深度学习利用了深度神经网络(deep neural network,DNN)来完成机器学习所做的相同任务。DNN由多层数学方程组成,无论是线性关系还是非线性关系,它都可以找到正确的数学操作步骤将输入转化为输出。深度学习的强大之处在于其处理复杂模型和大量参数的能力远远超过了人类工程师和科学家[10]。深度学习应用于CCTA可获得良好的图像质量[11]。目前已出现不少关于DLIR结合低辐射剂量的研究,其中采用100 kV管电压的CCTA的研究结论也被广泛认可[12]。考虑到图像对密度分辨率的要求,100 kV
被认为是CCTA所用电压的极限,本研究团队设计了低管电压80 kV结合DLIR算法的更低剂量的扫描方案,探讨其应用价值。
1 对象与方法
1.1 研究对象
研究对象为2023年2月至7月在我科接受心脏CCTA检查的60例患者,其中男35例、女25例,年龄55(31~88)岁。纳入标准:年龄>18岁;有临床疾病需要行CCTA增强检查。排除标准:碘对比剂过敏;孕妇;有肾功能不全、心力衰竭、肝功能不全、甲状腺功能亢进、影响数据测量的其他情况。根据扫描方案将60例患者分为100 kV方案组(A组)和80 kV 方案组(B组)各30例(保证体脂均衡)。本研究通过我院伦理委员会的批准(批件号:中大附三医伦Ⅱ2024-048-01),患者均签署知情同意书。
1.2 CT扫描方案
采用512层CT扫描仪(Revolution Apex)进行CCTA检查,患者在CCTA检查前舌下含服
0.5 mg 硝酸甘油以适当扩张血管。患者取仰卧位,检查前对其盆腔进行常规防护。
1.2.1 扫描方案
1)A组扫描方案。采用心脏容积模式(Cardiac)。电压模式:Manual、100 kV,电流模式:Manual、750 mA,平均电流:488 mA,转速:0.28 s/r、前置50% ASIR-V,重建算法:标准算法,探测器宽度:160 mm,螺距:0.992,扫描层厚:2.5 mm,扫描时长:0.42 s,无需憋气(one beat)。
2)B组扫描方案。采用心脏容积模式(Cardiac)。电压模式:Manual、80 kV,电流模式:Manual、750 mA,平均电流:488 mA,转速:
0.28 s/r、前置50% ASIR-V,重建算法:标准算法,探测器宽度:160 mm,螺距:0.992,扫描层厚:2.5 mm,扫描时长:0.42 s,无需憋气(one beat)。
2组均使用阈值触发技术,将感兴趣区(region
of interest,ROI)置于降主动脉,触发阈值设置为65 HU,扫描范围自气管分叉下1 cm至横隔,以智能心电门控自动选择曝光时相。采用2代冻结技术(snapshot freezing,SSF-2)对图像进行运动校正。
1.2.2 注射方案
采用双筒高压注射器经肘正中静脉以5 mL/s
流率注射碘佛醇(Iversol 350)造影剂,总量为60 mL,2组均在注入对比剂后再注入生理盐水
30 mL。
1.3 图像重建
将60例患者原始数据传输至AW4.7后处理工作站进行重建,层厚、层间距0.625 mm。A组采用60% 权重ASIR-V算法及A-DLIR算法,B组采用B-DLIR算法。最后对2组图像进行冠状动脉的容积再现(volume rendering,VR)、最大强度投影(maximum intensity projection,MIP)重建以及曲面重建(curved planar reformation,CPR)。对A组60%权重ASIR-V算法(A-AV60)、A组DLIR算法(A-DLIR)和B组DLIR算法(B-DLIR)共3种方案的图像重建质量进行评价。
1.4 图像重建质量评价
1.4.1 客观图像质量分析
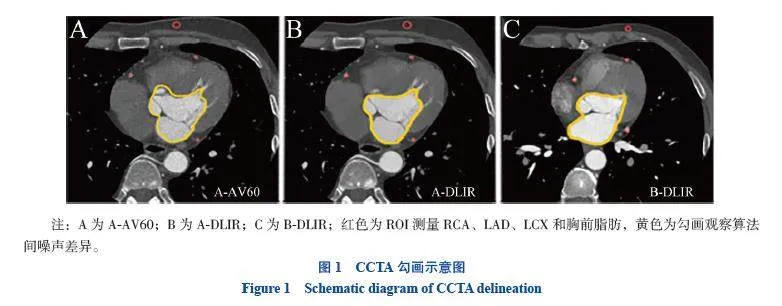
由2名具有4年工作经验的医学影像技师采用轮流监督的方法确保客观图像勾画准确,勾画原则:放大后轴面勾画、避开血管壁,取3次的平均,见图1。出现分歧时由具有17年工作经验的医学影像副主任技师实施最终勾画方案,读取数据。将ROI分别置于主动脉根(aortic root,AR)、左前降支(left anterior descending coronary artery,LAD)、左回旋支(left circumflex coronary artery,LCX)、右冠状动脉(right coronary artery,RCA)及同层胸前脂肪密度较均匀的区域内,记录各ROI的CT值及噪声值。参照测量层上下滚动测量3次,取3次平均值作为最终结果,计算各血管的信噪比(signal-to-noise ratio,SNR)和对比噪声比(contrast-to-noise ratio,CNR)。
1.4.2 主观图像质量分析
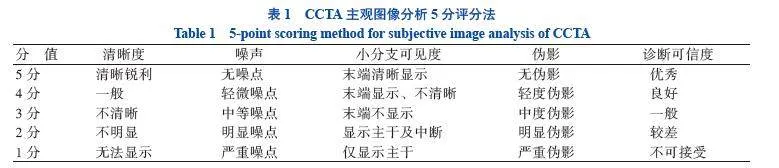
由2名分别具有16年和18年工作经验的放射科医师通过对冠状动脉3个主要分支:RCA、LAD、LCX的原始轴位图像、VR图、MIP图及CPR图进行5个因素的评分,包括清晰度、伪影、噪声、小分支可见度、诊断可信度。对每个因素采用 5 分评分法,见表1。5个因素平均得分2~5分被视为满足诊断需求,分析2名放射科医师的评价一致性[13]。2名放射科医师均不知道患者信息和重建方法。
1.5 有效辐射剂量
记录2组的容积CT剂量指数(volume CT dose index,CTDIvol)、剂量长度乘积(dose length product,DLP),并计算有效辐射剂量(effective dose,ED),冠状动脉的ED转换因子为0.014 mSv/(mGy·cm)。
1.6 统计学方法
采用SPSS 27.0进行统计分析 ,正态分布计量资料用表示,2组比较采用独立样本t检验,组内比较采用配对t检验;计数资料用n(%)表示,比较采用χ 2检验。具体为A组与B组患者年龄、身高、体质量、体质量指数(body mass index,BMI)、CTDIvol、DLP和ED的比较采用独立样本t检验,性别比较采用χ 2检验;客观图像质量评价指标中A-AV60和A-DLIR 2种算法之间的比较采用配对t检验,A-DLIR和B-DLIR 2种算法之间以及A-AV60和B-DLIR 2种算法之间的比较均采用独立样本t检验。采用Kappa检验分析2位放射科医师主观评分的一致性,Kappa值≤0.2为一致性程度很差,0.2 < Kappa值≤0.4为一致性程度一般,0.4 <Kappa值≤0.6为一致性程度中等,0.6 < Kappa值≤0.8为一致性程度较强,Kappa > 0.8为一致性程度很强。双侧P < 0.05表示差异有统计学意义。
2 结 果
2.1 一般资料
2组的年龄、BMI具可比性(P均> 0.05),但CTDIvol、DLP、ED等比较差异均有统计学意义(P均< 0.05),见表2。B组较A组ED降低45.14%。
2.2 客观图像质量评价
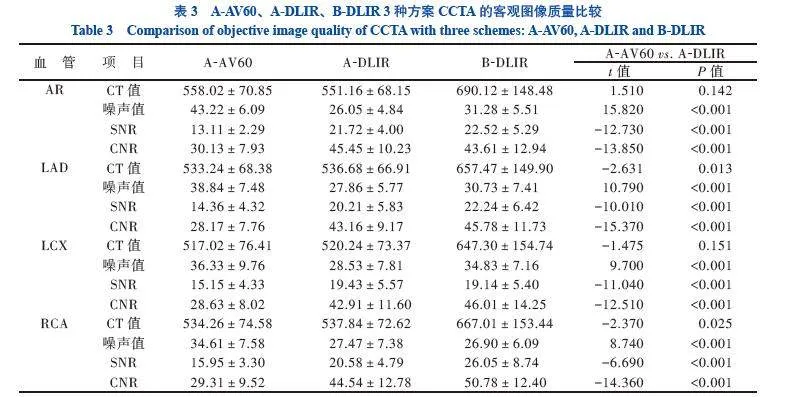
B-DLIR中AR、LAD、LCX、RCA的CT值均高于A-AV60及A-DLIR,比较差异均有统计学意义(P均< 0.001)。A-DLIR与B-DLIR相比,AR、LAD、LCX的噪声值相近,仅在RCA中比较差异有统计学意义(P < 0.05);A-DLIR与B-DLIR的SD均小于A-AV60,比较差异均有统计学意义(P均< 0.001)。A-DLIR与B-DLIR中AR、LAD、LCX、RCA的SNR、CNR相近,均高于A-AV60(P均< 0.05)。B-DLIR在客观图像评价中更具优势。
2.3 主观图像质量评价
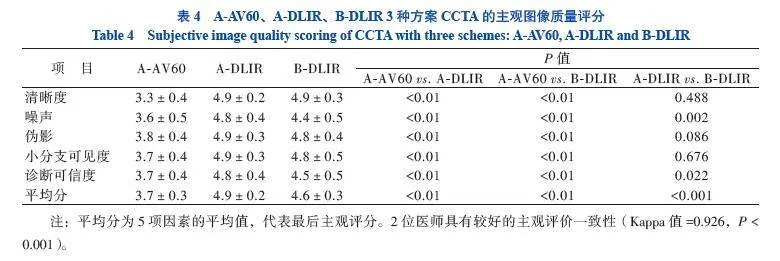
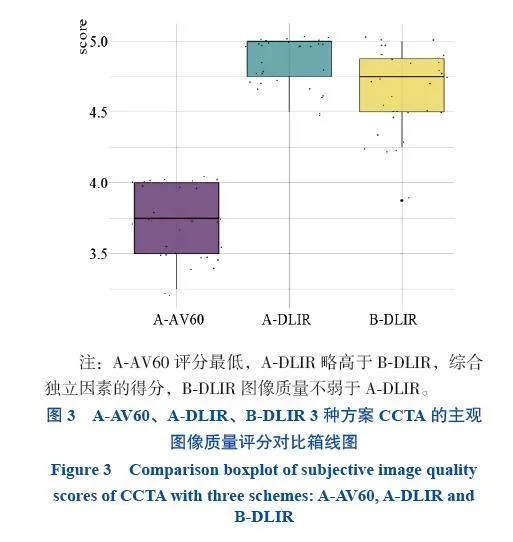
2名放射科医师主观图像质量评价有较强的一致性(Kappa=0.926,P < 0.001)。B-DLIR主观图像质量平均分高于A-AV60(P < 0.05),但低于A-DLIR(P < 0.05)。A-DLIR与B-DLIR的清晰度、伪影、小分支可见度比较差异均无统计学意义(P均>0.05)
3 讨 论
随着我国人口老龄化的加剧,动脉粥样硬化发病率逐渐上升,及早诊断对于控制病程进展成为重要。CCTA是冠状动脉粥样硬化性心脏病(冠心病)的常规检查方法之一,有助于正确诊断[13-14]。
尽管CCTA在解剖描述方面表现出色,也在功能预测方面具有巨大潜力,但辐射隐患仍然存在[15-20]。
目前常用低电压、自动管电流调制、大螺距、ASIR-V、缩小Z轴长度(减少无效扫描层面)等方法来降低CCTA辐射剂量[21-23]。然而,降低有效辐射剂量会直接影响CCTA的图像质量,因此,如何在低电压下保持甚至提高诊断图像质量是一个重大的技术挑战。
在 CCTA 扫描期间,钙化斑块会导致图像出现2种类型的伪影,一种是光晕伪影,另一种是射线束伪影。有研究者比较了IR算法与滤波反投影(filtered back projection,FBP)重建算法对严重钙化血管的评估,结果表明,与FBP重建算法相比,IR算法的诊断准确性更高,这与其降低了图像的噪声和伪影有关[24]。但目前常用的ASIR-V算法仍存在图像具有蜡状、塑料外观或点状不自然的伪影等缺点[25-26]。DLIR算法随人工智能的发展而出现,其被应用于低剂量CT中,能有效降低图像噪声[27],在不改变图像纹理的同时提高空间分辨率[28],从而提高图像质量。DLIR算法在诊断准确性、敏感性和特异性方面与IR算法相当[10]。
基于既往研究在CCTA中使用60%权重的ASIR-V算法的图像质量最佳的结论[29],本研究将使用60%权重的ASIR-V算法与DLIR算法进行比较。此外,本研究进一步探讨了DLIR算法更低辐射的可行性,进一步降低电压至80 kV[12]。结果显示与100 kV方案相比,80 kV DLIR算法的表现更出色,在主观图像质量评分中,尽管B-DLIR平均得分低于A-DLIR,但其中3个因素两者比较差异没有统计学意义。既往研究显示,在腹部CT和CT尿路造影中使用DLIR算法能减少有效辐射剂量,提高图像质量[30-31],这与本研究的结论一致,使用DLIR算法可以弥补低辐射剂量所致的噪声增加的缺点,并且可在低噪声下避免ASIR-V算法高权重出现的塑料、玻璃样伪影。
本研究有以下突破点:第一,DLIR算法可以降低CCTA检查的有效辐射剂量,减少辐射暴露,此外采用了更低的电压80 kV。第二,DLIR算法可以有效地降低图像噪声,提高整体图像质量,且在临床可诊断的低剂量辐射水平下保持FBP样噪声纹理,不影响解剖和病理结构[32],更低剂量并没有降低图像质量。第三,在提高末端血管的显示及清晰度方面,低剂量高权重的ASIR-V算法降噪后会出现蜡状或点状纹理,降低了低对比度物体的分辨率,使得小血管末端显示不佳,而DLIR算法可以在不改变图像纹理的情况下提高空间分辨率,因此对血管细小分支显示良好[26]。本研究初步证实了对于高空间分辨率的血管疾病,DLIR算法的诊断优势明显,这与同样属于高空间分辨率的结石的诊断效果相同[31]。
本研究存在一定局限性:第一,样本量较少,需要在后续临床工作中扩大样本量,进一步探讨DLIR算法在提高CCTA诊断性能方面的作用。第二,基于前人的结论,未开展其他权重ASIR-V算法和DLIR算法低、中、高级别的交叉比较,在以后的工作中将会尝试比较多重权重的效果。第三,未讨论不同BMI对辐射剂量、图像质量的影响。第四,未独立评价病变血管的评分差异,例如未将斑块、狭窄的评级归纳到清晰度、噪声的评价中,这需要在未来的研究中针对病变血管进行Gensini评分。
综上所述,在CCTA检查中,采用80 kV的DLIR算法方案有助于获得质量更优的图像,从而进一步提高诊断效能,且可减少辐射量。
参 考 文 献
[1] 车小双, 魏里, 贾惠娟, 等. 冠脉CTA联合能谱双下肢CTA检查在多血病变患者中的可行性研究[J]. 中国CT和MRI杂志, 2022, 20(9): 86-88. DOI: 10.3969/j.issn.1672-
5131.2022.09.032.
CHE X S, WEI L, JIA H J, et al. Feasibility study of coronary CTA combined with lower limb dual energy angiography in patients with arterial disease[J]. Chin J CT MRI, 2022, 20(9): 86-88. DOI: 10.3969/j.issn.1672-5131.2022.09.032.
[2] MOHANKUMAR S P, DAS S, LIKITHA P, et al. Kawasaki disease or polyarteritis nodosa: coronary involvement, a diagnostic conundrum[J]. Rheumatol Int, 2023, 43(12): 2327-2331. DOI: 10.1007/s00296-023-05388-1.
[3] ANTONOPOULOS A S, SIMANTIRIS S. Preventative imaging with coronary computed tomography angiography[J]. Curr Cardiol Rep, 2023, 25(11): 1623-1632. DOI: 10.1007/s11886-023-01982-8.
[4] ABDELRAHMAN K M, CHEN M Y, DEY A K, et al. Coronary computed tomography angiography from clinical uses to emerging technologies: JACC state-of-the-art review[J]. J Am Coll Cardiol, 2020, 76(10): 1226-1243. DOI: 10.1016/j.jacc.2020.06.076.
[5] VAN DRIEST F Y, BIJNS C M, VAN DER GEEST R J, et al. Utilizing (serial) coronary computed tomography angiography (CCTA) to predict plaque progression and major adverse cardiac events (MACE): results, merits and challenges[J]. Eur Radiol, 2022, 32(5): 3408-3422. DOI: 10.1007/s00330-021-08393-9.
[6] STOCKER T J, NÜHLEN N, SCHMERMUND A, et al. Impact of dose reduction strategies on image quality of coronary CTA in real-world clinical practice: a subanalysis of PROTECTION VI registry data[J]. AJR Am J Roentgenol, 2021, 217(6): 1344-1352. DOI: 10.2214/AJR.21.26007.
[7] MØRUP S D, STOWE J, KUSK M W, et al. The impact of ASiR-V on abdominal CT radiation dose and image quality: a phantom study[J]. J Med Imaging Radiat Sci, 2022, 53(3): 453-459. DOI: 10.1016/j.jmir.2022.06.008.
[8] ZHAO Y, LI D, LIU Z, et al. Comparison of image quality and radiation dose using different pre-ASiR-V and post-ASiR-V levels in coronary computed tomography angiography[J]. J Xray Sci Technol, 2021, 29(1): 125-134. DOI: 10.3233/XST-200754.
[9] JIANG B, LI N, SHI X, et al. Deep learning reconstruction shows better lung nodule detection for ultra-low-dose chest
CT[J]. Radiology, 2022, 303(1): 202-212. DOI: 10.1148/radiol.210551.
[10] ZHONG J, SHEN H, CHEN Y, et al. Evaluation of image quality and detectability of deep learning image reconstruction (DLIR) algorithm in single- and dual-energy CT[J]. J Digit Imaging, 2023, 36(4): 1390-1407. DOI: 10.1007/s10278-023-00806-z.
[11] WANG M, FAN J, SHI X, et al. A deep-learning reconstruction algorithm that improves the image quality of low-tube-voltage coronary CT angiography[J]. Eur J Radiol, 2022, 146: 110070. DOI: 10.1016/j.ejrad.2021.110070.
[12] WANG H, WANG R, LI Y, et al. Assessment of image quality of coronary computed tomography angiography in obese patients by comparing deep learning image reconstruction with adaptive statistical iterative reconstruction veo[J]. J Comput Assist Tomogr, 2022, 46(1): 34-40. DOI: 10.1097/RCT.0000000000001252.
[13] 张茸祯, 贾敏, 娄豆豆, 等. 合并心血管疾病的高血压患者强化降压治疗研究进展[J]. 新医学, 2024, 55(4): 248-254. DOI: 10.3969/j.issn.0253-9802.2024.04.002.
ZHANG R Z, JIA M, LOU D D, et al. Advances in intensive antihypertensive treatment in hypertensive patients complicated with cardiovascular disease[J]. J New Med, 2024, 55(4): 248-254. DOI: 10.3969/j.issn.0253-9802.2024.04.002.
[14] LI W, HUANG W, LI P, et al. Application of deep learning image reconstruction-high algorithm in one-stop coronary and carotid-cerebrovascular CT angiography with low radiation and contrast doses[J]. Quant Imaging Med Surg, 2024, 14(2): 1860-1872. DOI: 10.21037/qims-23-864.
[15] PAALIMÄKI-PAAKKI K, VIRTANEN M, HENNER A, et al. Effects of a 360°virtual counselling environment on patient anxiety and CCTA process time: a randomised controlled trial[J]. Radiography, 2023, 29(Suppl 1): S13-S23. DOI: 10.1016/j.
radi.2022.09.013.
[16] AUPONGKAROON P, MAKARAWATE P, CHAOSUWAN-NAKIT N. Comparison of radiation dose and its correlates between coronary computed tomography angiography and invasive coronary angiography in Northeastern Thailand[J]. Egypt Heart J, 2022, 74(1): 6. DOI: 10.1186/s43044-022-00241-5.
[17] CUNDARI G, DEILMANN P, MERGEN V, et al. Saving contrast media in coronary CT angiography with photon-counting detector CT[J]. Acad Radiol, 2024, 31(1): 212-220. DOI: 10.1016/j.acra.2023.06.025.
[18] NAGAYAMA Y, EMOTO T, KATO Y, et al. Improving image quality with super-resolution deep-learning-based reconstruction in coronary CT angiography[J]. Eur Radiol, 2023, 33(12): 8488-8500. DOI: 10.1007/s00330-023-09888-3.
[19] LI W, DIAO K, WEN Y, et al. High-strength deep learning image reconstruction in coronary CT angiography at 70-kVp tube voltage significantly improves image quality and reduces both radiation and contrast doses[J]. Eur Radiol, 2022, 32(5): 2912-2920. DOI: 10.1007/s00330-021-08424-5.
[20] ZHANG Y, WANG Y, LI J, et al. Refining the radiation and contrast medium dose in weight-grouped scanning protocols for coronary CT angiography[J]. J Appl Clin Med Phys, 2023,
24(7): e14041. DOI: 10.1002/acm2.14041.
[21] KNOTT E A, ROSE S D, WAGNER M G, et al. CT fluoroscopy for image-guided procedures: physician radiation dose during full-rotation and partial-angle CT scanning[J]. J Vasc Interv Radiol, 2021, 32(3): 439-446. DOI: 10.1016/j.jvir.2020.10.033.
[22] ZHOU W, MALAVE M N, MALONEY J A, et al. Radiation dose reduction using spectral shaping in pediatric non-contrast sinus CT[J]. Pediatr Radiol, 2023, 53(10): 2069-2078. DOI: 10.1007/s00247-023-05699-2.
[23] DANKERL P, MAY M S, CANSTEIN C, et al. Cutting staff radiation exposure and improving freedom of motion during CT interventions: comparison of a novel workflow utilizing a radiation protection cabin versus two conventional workflows[J]. Diagnostics (Basel), 2021, 11(6): 1099. DOI: 10.3390/diagnostics11061099.
[24] JEON P H, JEON S H, KO D, et al. Assessment of image quality of coronary CT angiography using deep learning-based CT reconstruction: phantom and patient studies[J]. Diagnostics (Basel), 2023, 13(11): 1862. DOI: 10.3390/diagnostics13111862.
[25] WANG J J, CHI X T, WANG W W, et al. Analysis of contrast-enhanced spectral chest CT optimal monochromatic imaging combined with ASIR and ASIR-V[J]. Eur Rev Med Pharmacol Sci, 2022, 26(6): 1930-1938. DOI: 10.26355/eurrev_202203_28339.
[26] KAGA T, NODA Y, FUJIMOTO K, et al. Deep-learning-based image reconstruction in dynamic contrast-enhanced abdominal CT: image quality and lesion detection among reconstruction strength levels[J]. Clin Radiol, 2021, 76(9): 710.e15-710.710.e24. DOI: 10.1016/j.crad.2021.03.010.
[27] JENSEN C T, LIU X, TAMM E P, et al. Image quality assessment of abdominal CT by use of new deep learning image reconstruction: initial experience[J]. AJR Am J Roentgenol, 2020, 215(1): 50-57. DOI: 10.2214/AJR.19.22332.
[28] LYU P, LI Z, CHEN Y, et al. Deep learning reconstruction CT for liver metastases: low-dose dual-energy vs standard-dose single-energy[J]. Eur Radiol, 2024, 34(1): 28-38. DOI: 10.1007/s00330-023-10033-3.
[29] NAM J G, HONG J H, KIM D S, et al. Deep learning reconstruction for contrast-enhanced CT of the upper abdomen: similar image quality with lower radiation dose in direct comparison with iterative reconstruction[J]. Eur Radiol, 2021, 31(8): 5533-5543. DOI: 10.1007/s00330-021-07712-4.
[30] CHENG Y, HAN Y, LI J, et al. Low-dose CT urography using deep learning image reconstruction: a prospective study for comparison with conventional CT urography[J]. Br J Radiol, 2021, 94(1120): 20201291. DOI: 10.1259/bjr.20201291.
[31] RACINE D, BECCE F, VIRY A, et al. Task-based characterization of a deep learning image reconstruction and comparison with filtered back-projection and a partial model-based iterative reconstruction in abdominal CT: a phantom study[J]. Phys Med, 2020, 76: 28-37. DOI: 10.1016/j.ejmp.2020.06.004.
[32] KAGA T, NODA Y, MORI T, et al. Unenhanced abdominal low-dose CT reconstructed with deep learning-based image reconstruction: image quality and anatomical structure d
epiction[J]. Jpn J Radiol, 2022, 40(7): 703-711. DOI: 10.1007/s11604-022-01259-0.
(责任编辑:洪悦民)
