超声引导下腹股沟韧带上髂筋膜阻滞联合喉罩全麻在老年患者大隐静脉曲张手术中的应用
2024-10-19徐方胜马舒玉刘容光王梅芳濮健峰



【摘要】 目的 探讨超声引导下腹股沟韧带上髂筋膜阻滞联合喉罩全身麻醉(全麻)在老年患者大隐静脉曲张手术中的应用价值。方法 选取择期行单侧大隐静脉高位结扎点式剥脱联合激光闭合术的老年患者60例,随机分为A组(单纯喉罩全麻)和B组(超声引导下腹股沟韧带上髂筋膜阻滞联合喉罩全麻),每组30例。记录术中麻醉药物用量、血流动力学波动和喉罩拔除时间;评估术后静态和动态疼痛视觉模拟量表(VAS)评分、15项恢复质量(QoR-15)评分、简易智力状态检查(MMSE)评分以及不良反应情况,并进行比较。结果 B组术后24 h QoR-15和MMSE评分均高于A组(P均<0.05);A组切皮时的平均动脉压和心率均高于B组(P均<0.05);B组术后5 min、30 min、6 h、12 h静态和动态疼痛VAS评分均低于A组(P均<0.05);B组丙泊酚用量、瑞芬太尼用量及喉罩拔除时间均低于A组,差异均有统计学意义(P均<0.05)。结论 超声引导下腹股沟韧带上髂筋膜阻滞联合喉罩全麻可改善患者术后恢复质量和认知功能,减少麻醉药物用量,缩短拔管时间,增强血流动力学稳定性,减轻术后疼痛,从而促进快速康复。
【关键词】 腹股沟韧带上髂筋膜阻滞;老年患者;大隐静脉曲张;术后恢复质量;喉罩全麻
Application of ultrasound-guided suprainguinal fascia iliaca block combined with general anesthesia with laryngeal mask in elderly patients undergoing surgery for great saphenous varicose veins
XU Fangsheng, MA Shuyu, LIU Rongguang, WANG Meifang, PU Jianfeng
(Department of Anesthesiology, Affiliated Changshu Hospital of Nantong University, Changshu 215500, China )
Corresponding author: PU Jianfeng, E-mail: pjh61255397@163.com
【Abstract】 Objective To evaluate the application value of ultrasound-guided suprainguinal iliaca fascia block combined with general anesthesia with laryngeal mask in elderly patients undergoing surgery for the great saphenous varicose veins. Methods Sixty elderly patients scheduled for unilateral high ligation and stripping of the great saphenous veins combined with endovenous laser ablation were randomly divided into Group A (general anesthesia with laryngeal mask alone, n = 30) and Group B (ultrasound-guided suprainguinal fascia iliaca block combined with general anesthesia with laryngeal mask, n = 30). Intraoperative anesthetic consumption, hemodynamic fluctuations, and laryngeal mask removal time were recorded. Postoperative changes in static and dynamic Visual Analogue Scale (VAS) pain scores, 15-item Quality of Recovery (QoR-15) scores, Mini-Mental State Examination (MMSE) scores, and adverse events were also evaluated. Results The QoR-15 and MMSE scores at postoperative 24 h in Group B were significantly higher than those in Group A (both P < 0.05). The mean arterial pressure (MAP) and heart rate (HR) during skin incision in Group A were significantly higher than those in Group B (both P < 0.05). The static and dynamic VAS pain scores at postoperative 5 min, 30 min, 6 h, and 12 h in Group B were significantly lower compared to those in Group A (all P < 0.05). In Group B, the consumption of propofol and remifentanil was significantly less, and the laryngeal mask removal time was significantly shorter than those in Group A, with statistically significant differences (both P < 0.05). Conclusion Ultrasound-guided suprainguinal fascia iliaca block combined with general anesthesia with laryngeal mask improves postoperative quality of recovery and cognitive function, reduces anesthetic consumption, shortens extubation time, enhances hemodynamic stability and alleviates postoperative pain, thereby promoting rapid recovery.
【Key words】 Suprainguinal fascia iliaca block; Elderly patient; Great saphenous varicose vein; Postoperative quality of recovery;
General anesthesia with laryngeal mask
大隐静脉曲张是一种常见的慢性血管疾病,与长时间站立、缺乏运动等生活方式密切相关,常见于中老年患者,若不及时治疗,可能导致皮肤溃烂、血管破裂出血和血栓形成等严重并发症,对患者的健康造成极大影响[1-2]。腔内激光闭合术作为下肢静脉曲张一种安全有效的微创治疗技术已被广泛应用,联合点状剥脱和高位结扎术,不仅可以全面清除异常的静脉组织,还可降低术后复发率,提高治疗成功率和长期临床疗效[3-5]。目前临床多采用椎管内麻醉方案,但部分老年患者伴有脊柱畸形、凝血功能障碍等,这些因素显著增加椎管内麻醉的风险[6]。喉罩全身麻醉(全麻)作为一种替代方案,不仅操作简便易行、对患者刺激小,而且能够提供全程的气道保护,具有更高的安全性[7-9]。联合区域阻滞技术可以有效提升术中血流动力学的稳定性、降低麻醉药物用量和减轻术后疼痛影响,有助于提升患者的医疗满意度和加速康复[10-11]。腹股沟韧带上髂筋膜阻滞是近年来提出的新型区域阻滞技术,具有操作简便、安全性高等特点,能够有效地阻滞股神经、闭孔神经和股外侧皮神经,可为大隐静脉曲张手术提供较为满意的镇痛[12-14]。
但目前关于超声引导下腹股沟韧带上髂筋膜阻滞联合喉罩全麻在老年大隐静脉曲张手术中的研究仍较有限。因此,本研究旨在评估这一麻醉方案的临床效果,为优化老年患者的麻醉策略提供参考。
1 对象与方法
1.1 研究对象
选择2021年1月至2023年12月于南通大学附属常熟医院行择期单侧大隐静脉高位结扎点式剥脱联合激光闭合术的老年患者60例。纳入标准:年龄≥65岁、体质量指数(body mass index, BMI)18~30 kg/m2、ASA分级Ⅰ~Ⅲ级。排除标准:既往神经精神疾病史、酰胺类局部麻醉药物过敏史、阿片类药物成瘾史、穿刺部位感染、凝血功能障碍或严重肝肾功能不全者。采用随机数表法将患者分为A组和B组:A组采用单纯喉罩全麻,B组采用超声引导行腹股沟韧带上髂筋膜阻滞联合喉罩全麻,每组各30例。本研究经南通大学附属常熟医院伦理委员会批准(批件号:2020-KY-021),患者或其授权委托人均签署了知情同意书。
样本量的计算根据姜卜维等[15]探讨髂筋膜阻滞对全髋置换术患者术后恢复质量影响的研究,使用PASS软件进行计算,假设α=0.05,1-β=0.8,最终确定每组纳入30例患者。
1.2 麻醉方法
术前常规禁饮禁食,入室后开放上肢静脉通路补液;常规监测患者各项生命体征,如血压、心率(heart rate,HR)、心电图(electrocardiogram,ECG)、脉搏血氧饱和度(pulse oxygen saturation,SpO2)和脑电双频指数(bispectral index,BIS)。B组于麻醉诱导前先行超声引导下腹股沟韧带上髂筋膜阻滞:患者取仰卧位,触诊确定髂前上棘,将高频线阵探头置于髂前上棘内侧,与脐连线外1/3处,调整探头使成像清晰,辨别髂骨、髂腰肌、髂筋膜和旋髂深动脉,见图1。消毒铺巾后,采用平面内进针技术,从髂前上棘处进针,针尖到达髂肌表面后给予2 mL生理盐水进行水分离试验。若液体沿髂腰肌表面呈线性扩散,表明位置正确,给予0.25%罗哌卡因30 mL完成注射。操作完成后间隔5 min测试股神经、股外侧皮神经及闭孔神经皮区感觉,以针刺痛觉减退或消失为阻滞成功。
喉罩全麻方案:全麻诱导采用瑞芬太尼靶控输注,效应室浓度为2 ng/mL,静脉推注依托咪酯1.5~2.0 mg/kg和罗库溴铵注射液6 mg/kg。BIS值降至40~60,且肌松满意后,置入喉罩行机械通气。术中维持采用丙泊酚和瑞芬太尼效应室浓度靶控输注,并按需追加肌松药。调整呼吸参数和麻醉药物输注速度,维持术中血流动力学平稳,呼气末二氧化碳分压35~45 mmHg,BIS值40~60。手术结束前10 min给予0.1 mg芬太尼用于术后镇痛,手术结束前5 min停用丙泊酚和瑞芬太尼,并给予1 mg/kg舒更葡糖拮抗肌松。唤醒患者,待其呼吸频率10~20次/分,潮气量> 8 mL/kg后拔除喉罩。若术中出现低血压(收缩压较基础值降低30%或< 90 mmHg)或心动过缓(HR< 50次/分),则静脉注射麻黄碱6 mg/次或阿托品0.5 mg/次,必要时重复给药。若术后静态疼痛视觉模拟量表(visual analogue scale,VAS)评分>3分,给予50 mg曲马多补救镇痛。
1.3 观察指标
①记录2组患者麻醉诱导前(T1)、喉罩置入时(T2)、手术切皮时(T3)和手术结束时(T4)的平均动脉压(mean arterial pressure,MAP)和HR;②记录术后5 min(T5)、30 min(T6)、6 h(T7)、12 h(T8)、24 h(T9)静态和动态疼痛VAS评分;③记录术中丙泊酚、瑞芬太尼用量和喉罩拔除时间;④记录T1和T9时的15项恢复质量(15-item Quality of Recovery,QoR-15)评分和简易智力状态检查(Mini-mental State Examination,MMSE)评分;⑤记录术后补救镇痛情况,苏醒期躁动、呼吸抑制、恶心呕吐、咽痛和头晕等不良反应发生情况。
1.4 统计学方法
应用SPSS 27.0进行数据分析,正态分布的计量资料以表示,2组间比较采用独立样本t检验,血流动力学资料采用重复测量方差分析,单独效应分析采用独立样本t检验和配对t检验。偏态分布计量资料以M(P25,P75)表示,VAS评分资料采用广义估计方程分析,单独效应分析采用Wilcoxon秩和检验及符号秩和检验。计数资料以n(%)表示,组间比较采用χ 2检验或Fisher确切概率法。以双侧P < 0.05为差异有统计学意义。
2 结 果
2.1 2组患者术前一般资料比较
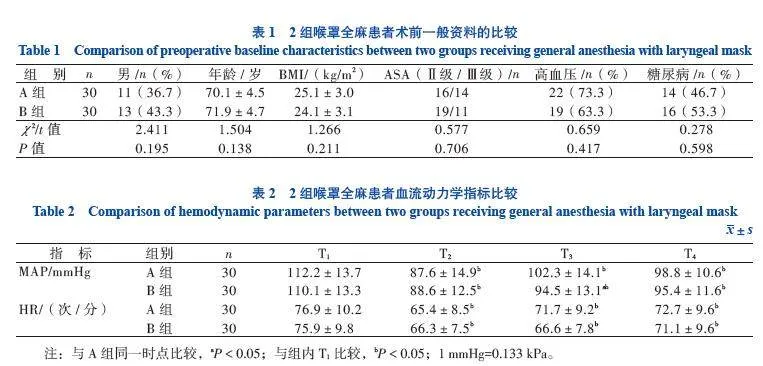
2组患者性别、年龄、BMI、ASA分级、高血压及糖尿病比例差异均无统计学意义(P均>0.05),见表1。
2.2 2组患者血流动力学指标比较
MAP比较:重复测量方差分析显示Mauchly’s球形检验P < 0.001,不符合球形性对称检验,采用Greenhouse-Geisser方法进行校正,时间因素和组别因素存在交互作用(F=18.101,P < 0.001),因此分析单独效应,结果显示A组T3时的MAP高于B组(P < 0.05),其余时刻比较差异均无统计学意义,A组和B组T2~T4时的MAP均低于T1,差异有统计学意义(P均< 0.05),见表2。
HR比较:重复测量方差分析显示Mauchly’s球形检验P = 0.227,符合球形性对称检验,时间因素和组别因素无交互作用(F=1.444,P = 0.234),分组因素对HR的主效应无统计学意义(F=2.346,P = 0.131),时间因素对HR的主效应有统计学意义(F=19.315,P < 0.001),事后分析显示A组和B组T2~T4时的HR均低于T1(P均< 0.05),见表2。
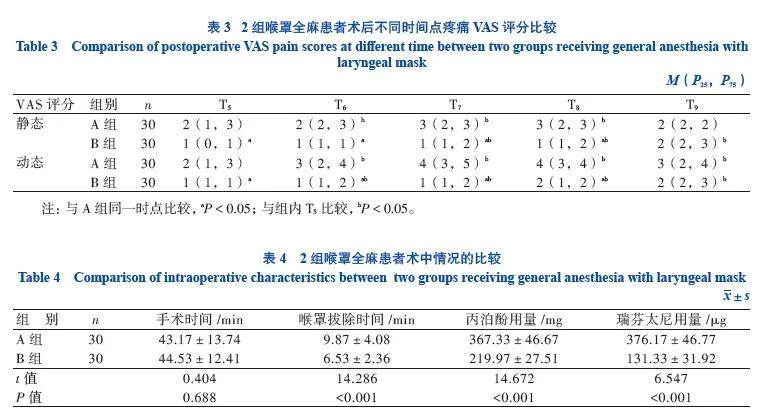
2.3 2组患者疼痛VAS评分比较
静态疼痛VAS评分比较:广义估计方程分析显示时间因素和分组因素存在交互作用(F=20.753,P < 0.001);单独效应分析显示A组T6~T8静态疼痛VAS评分高于T5(P < 0.001),B组T7~T9静态疼痛VAS评分高于T5(P < 0.001),B组T5~T8静态疼痛VAS评分均低于A组(P < 0.05),见表3。
动态疼痛VAS评分比较:广义估计方程分析显示时间因素和分组因素存在交互作用(F=91.347,P < 0.001),单独效应分析显示A组和B组T6~T9动态疼痛VAS评分均高于T5(P均< 0.001),B组T5~T8动态疼痛VAS评分均低于A组(P均< 0.05),见表3。
2.4 2组患者术中情况比较
B组喉罩拔除时间、丙泊酚用量及瑞芬太尼用量均低于A组,差异均有统计学意义(P均< 0.05),见表4。
2.5 2组患者术后恢复情况比较
与T1时相比,2组患者T9的QoR-15评分和MMSE评分均降低(P均< 0.05),B组T9的MMSE评分和QoR-15高于A组,差异均有统计学意义(P均< 0.05),见表5。
2.6 2组患者术后不良反应发生情况比较
2组补救镇痛、恶心、头晕、谵妄的发生情况差异均无统计学意义(P均> 0.05),均无患者发生呕吐、咽痛、呼吸抑制、苏醒期躁动情况,见表6。
3 讨 论
大隐静脉是位于下肢内侧的浅表静脉,起于足背静脉弓内侧端,经过小腿内侧伴隐神经上行,进入大腿内侧,最终汇入股静脉。大隐静脉曲张的手术范围涉及大腿和小腿的前内侧区域,主要受股神经支配,还涉及坐骨神经、生殖股神经及闭孔神经等[16-17]。Li等[18]研究发现,股神经阻滞联合肿胀麻醉用于大隐静脉手术可有效减少肿胀麻醉液的使用量、降低皮肤瘀斑的发生率,并且不增加麻醉或其他手术并发症的风险。李振兴等[19]进一步研究表明,采用股神经联合坐骨神经阻滞可满足大隐静脉剥脱联合高位结扎的手术要求,无需术中追加局部麻醉,其镇痛效果与椎管内麻醉相当,并且术中血流动力学更加平稳。然而,股神经和坐骨神经与血管毗邻,联合阻滞增加了操作难度及复杂度,并且存在神经和血管损伤的风险[20]。随着舒适化医疗理念的推进,目前多采用喉罩全麻联合区域阻滞技术,具有更高的舒适性和安全性。吴培培等[10]研究表明,采用股神经阻滞联合喉罩全麻的镇痛效果确切,术中血流动力学波动较小,有利于促进患者恢复及提高麻醉安全性。但鉴于股神经阻滞距离大隐静脉高位结扎的位置较近,注射的局麻药容易影响手术视野,而腹股沟韧带上髂筋膜阻滞位置较高,有腹股沟韧带阻隔局麻药向尾侧扩散,操作更加简单安全、阻滞范围更广,因此本研究采用腹股沟韧带上髂筋膜阻滞联合喉罩的全麻方案[13, 21]。本研究结果表明,髂筋膜阻滞联合喉罩全麻可减少术中镇痛药物用量,提升血流动力学的稳定性,缩短喉罩拔除时间及降低术后疼痛评分,有助于老年患者的快速康复。这一结果也与既往研究相一致[22-23]。
Bansal等[24]在髋关节镇痛的研究中发现,腹股沟韧带上入路的髂筋膜阻滞能够提供至少24 h的有效镇痛效果,并且相较于腹股沟韧带下入路,其镇痛满意度更高。刘绪华等[25]的研究也验证了髂筋膜阻滞的镇痛效果,其镇痛作用甚至可持续至术后48 h。在本研究中,2组患者术后24 h的静态和动态疼痛VAS评分主要集中在1~2分,表明大隐静脉手术的疼痛主要发生在术后第1天。而B组患者在T5~T8时的静态和动态疼痛VAS评分均低于A组,表明髂筋膜阻滞可以有效地缓解术后疼痛。
术后恢复质量是以患者为中心的重要结局指标,而QoR-15是目前使用最广的评估工具之一,包括身体舒适度、情绪状态、生理独立性、心理支持及疼痛5个维度,共计15项主观参数,具有较高的简便性和可靠度[26-27]。姜卜维等[15]的研究探讨了髂筋膜阻滞对髋关节置换术后恢复质量的影响,结果显示髂筋膜阻滞能够显著提升患者的术后恢复质量,并促进其康复过程。本研究结果显示,B组患者术后24 h的QoR-15评分高于A组,提示联合髂筋膜阻滞对促进患者术后恢复质量具有积极作用,可能与术后疼痛程度的减轻有关,不仅缓解了患者术后的紧张和焦虑,而且提升了术后的睡眠质量和满意度。
老年患者是术后认知功能减退的高危人群,可能与年龄增长、较高的ASA分级、脑血管疾病和低蛋白等因素密切相关[28]。MMSE量表能够全面、准确、迅速地反映被试者智力状态及认知功能缺损程度,是临床评估患者围术期认知功能的重要手段[29]。本研究结果显示,与术前相比,2组患者术后24 h的MMSE评分均降低,表明手术创伤和疼痛会对患者术后认知功能有一定的影响。而B组术后24 h的MMSE评分高于A组,提示联合髂筋膜阻滞可减轻手术对认知功能的负面影响。孙倩倩等[30]研究也得出类似结论,并发现与中枢神经系统炎症反应、神经功能损伤相关的生物学指标S100B蛋白的升高幅度也随之降低,这说明联合髂筋膜阻滞可有效缓解或抑制术后中枢神经炎症反应,这可能与阿片类药物用量减少以及术后疼痛应激反应减轻有关。
尽管如此,本研究还存在一些局限性。首先,对术后指标的观察仅限于术后24 h,缺乏更长时间的随访数据。其次,本研究未与其他神经阻滞方法进行比较,限制了对不同阻滞技术效果的全面评估。此外,本研究中的术后镇痛和补救镇痛未联合使用非甾体类镇痛药物,未来的研究中需要更好地结合《中国加速康复外科临床实践指南》的推荐,进一步优化术后镇痛方案。最后,由于本研究为单中心研究且样本量较小,研究结果的普适性可能受到限制,因此,未来需要开展多中心、大样本量的随机对照研究,以提供更全面、客观的评估,为临床决策提供更高水平的参考依据。
综上所述,与单纯喉罩全麻相比,术前联合应用超声引导下腹股沟韧带上髂筋膜阻滞可有效减少术中阿片类镇痛药物的用量,增加患者血流动力学的稳定性,缩短麻醉恢复时间,减少术后疼痛评分,提升术后恢复质量并改善术后认知功能,具有较高的应用价值。
参 考 文 献
[1] 何川, 丁洋, 顾俊菲, 等. 原发性大隐静脉曲张传统开放性手术与激光治疗联合泡沫硬化术对机体免疫系统影响的比较[J]. 新医学, 2023, 54(9): 639-643. DOI: 10.3969/j.issn.
0253-9802.2023.09.006.
HE C, DING Y, GU J F, et al. Comparison of the effects between traditional open surgery and laser treatment combined with foam sclerotherapy on immune system in patients with primarygreat saphenous varicose veins. J New Med, 2023, 54(9): 639-643. DOI: 10.3969/j.issn.0253-9802.2023.09.006.
[2] MOHAMED A H, HOWITT A, RAE S, et al. Ten-year outcomes of a randomized clinical trial of endothermal ablation versus conventional surgery for great saphenous varicose veins[J].
Br J Surg, 2024, 111(8): znae195. DOI: 10.1093/bjs/znae195.
[3] BARALDI C, BISSACCO D. Safety and efficacy of combining saphenous endovenous laser ablation and varicose veins foam sclerotherapy: an analysis on 5500 procedures in patients with advance chronic venous disease (C3-C6)[J]. Vasc Endovascular Surg, 2024, 58(1): 60-64. DOI: 10.1177/
15385744231188804.
[4] HUANG Y, ZHANG D, ZHOU C, et al. The first meta-analysis research on the effects of endovenous laser ablation combined with sapheno-femoral junction high ligation of the great saphenous vein[J]. Lasers Med Sci, 2023, 38(1): 175. DOI: 10.1007/s10103-023-03833-y.
[5] JIANG W, LIANG Y, LONG Z, et al. Endovenous radiofrequency ablation vs laser ablation in patients with lower extremity varicose veins: a meta-analysis [J]. J Vasc Surg Venous Lymphat Disord, 2024, 12(5): 101842. DOI: 10.1016/j.jvsv.2
024.101842.
[6] MARTIN-FLORES M. Epidural and spinal anesthesia[J]. Vet Clin North Am Small Anim Pract, 2019, 49(6): 1095-1108. DOI: 10.1016/j.cvsm.2019.07.007.
[7] DONG W, ZHANG W, ER J, et al. Comparison of laryngeal mask airway and endotracheal tube in general anesthesia in children[J]. Exp Ther Med, 2023, 26(6): 554. DOI: 10.3892/etm.2023.12253.
[8] KATAOKA N, IMAMURA T. Clinical advantage of laryngeal mask airway over conventional endotracheal intubation during pulmonary vein isolation[J]. J Interv Card Electrophysiol, 2024 Feb 12. DOI: 10.1007/s10840-024-01766-2.
[9] LI X, LIU B, WANG Y, et al. The effects of laryngeal mask airway versus endotracheal tube on atelectasis in patients undergoing general anesthesia assessed by lung ultrasound: a protocol for a prospective, randomized controlled trial[J]. PLoS One, 2022, 17(9): e0273410. DOI: 10.1371/journal.pone.0273410.
[10] 吴培培, 蒋强. 超声引导下股神经阻滞复合全身麻醉对大隐静脉高位结扎加点式剥脱术患者术后镇痛的影响[J]. 重庆医学, 2017, 46(31): 4408-4410. DOI: 10.3969/j.issn.1671-
8348.2017.31.031.
WU P P, JIANG Q. Effect of ultrasound-guided femoral nerve block combined with general anesthesia on postoperative analgesia in patients undergoing high ligation and point stripping of great saphenous vein[J]. Chongqing Med, 2017, 46(31): 4408-4410. DOI: 10.3969/j.issn.1671-8348.2017.31.031.
[11] YANG X, BAO L, GONG X, et al. Impacts of ultrasound-guided nerve block combined with general anesthesia with laryngeal mask on the patients with lower extremity fractures[J].
J Environ Public Health, 2022, 2022: 3603949. DOI: 10.1155/2022/3603949.
[12] GENC C, AKDENIZ S, CANIKLI S, et al. Ultrasound-guided suprainguinal fascia iliaca block as part of anesthesia management for lower extremity surgeries: a single-center retrospective cohort feasibility study [J]. Cureus, 2023, 15(10): e47795. DOI: 10.7759/cureus.47795.
[13] WEN G, FENG W, FU B. Clinical effect of ultrasound-guided inguinal ligament iliac fascia block anesthesia and its effect on postoperative analgesia and stress level[J]. Minerva Med, 2022, 113(3): 591-592. DOI: 10.23736/S0026-4806.20.07175-X.
[14] YAO F, SHUI Y H, XIANG J L, et al. Application of superior iliac fascia block of inguinal ligament combined with patient controlled intravenous analgesia in elderly patients after hip arthroplasty[J]. China J Orthop Traumatol, 2024, 37(5): 482-487. DOI: 10.12200/j.issn.1003-0034.20220753.
[15] 姜卜维, 马凤丹, 黄瑾, 等. 超声引导下髂腰肌平面阻滞对髋关节置换术患者术后恢复质量的影响[J]. 临床麻醉学杂志, 2024, 40(2): 133-138. DOI: 10.12089/jca.2024.02.005.
JIANG B W, MA F D, HUANG J, et al. Effect of ultrasound-guided iliopsoas plane block on quality of postoperative recovery in patients un-dergoing hip arthroplasty[J]. J Clin Anesthesiol, 2024, 40(2): 133-138. DOI: 10.12089/jca.2024.02.005.
[16] ANTANI M R, DATTILO J B. Varicose Veins [M]. Treasure Island (FL): StatPearls Publishing, 2023.
[17] BISSACCO D, CALLIARI F M, SETTEMBRINI A M. Great saphenous vein idiopathic dissection[J]. J Vasc Surg Venous Lymphat Disord, 2023, 11(6): 1286. DOI: 10.1016/j.jvsv.
2023.05.007.
[18] LI Y H, WANG T, QIAN C, et al. Application of femoral nerve block in treating great saphenous vein insufficiency by endovenous radiofrequency ablation combined with punctate stripping[J]. Clin Appl Thromb Hemost, 2023, 29: 10760296231220054. DOI: 10.1177/10760296231220054.
[19] 李振兴, 吴秀玲. 股神经联合坐骨神经阻滞麻醉在大隐静脉曲张剥脱术中的应用[J]. 上海医学, 2019, 42(5): 269-272. DOI: CNKI: SUN: SHYX.0.2019-05-003.
LI Z X, WU X L. Application of femoral nerve combined with sciatic nerve block in great saphenous vein stripping[J]. Shanghai Med J, 2019, 42(5): 269-272. DOI: CNKI: SUN: SHYX.0.2019-05-003.
[20] WITAYAKOM W, SUKHONTHAMARN K, KOSUWON W, et al.
An anatomic consideration of the femoral nerve during direct anterior hip approach: a cadaveric study[J]. Surg Rad3BzQ3nlQ6N77dzE9hsp4CV4w7gLv8n3/RwJFSBy44Kc=iol Anat, 2024, 46(6): 733-738. DOI: 10.1007/s00276-024-03364-3.
[21] PU M, XU J, XU X, et al. Comparative analysis of analgesic effect of iliac fascial block with vertical and horizontal inguinal approach for total hip arthroplasty[J]. Am J Transl Res, 2021, 13(8): 9593-9599.
[22] VERGARI A, FRASSANITO L, TAMBURELLO E, et al. Supra-inguinal fascia iliaca compartment block for postoperative analgesia after Acetabular fracture surgery[J]. Injury, 2020,
51(12): 2996-2998. DOI: 10.1016/j.injury.2020.10.001.
[23] ZHENG T, HU B, ZHENG C Y, et al. Improvement of analgesic efficacy for total hip arthroplasty by a modified ultrasound-guided supra-inguinal fascia iliaca compartment block[J]. BMC Anesthesiol, 2021, 21(1): 99. DOI: 10.1186/s12871-021-01314-9.
[24] BANSAL K, SHARMA N, SINGH M R, et al. Comparison of suprainguinal approach with infrainguinal approach of fascia iliaca compartment block for postoperative analgesia[J]. Indian J Anaesth, 2022, 66(Suppl 6): S294-S299. DOI: 10.4103/ija.ija_823_21.
[25] 刘绪华, 谢珏, 袁从旺, 等. 超声引导下髂筋膜间隙阻滞在老年患者全髋关节置换术中的应用[J]. 临床麻醉学杂志, 2022, 38(4): 356-360. DOI: 10.12089/jca.2022.04.004.
LIU X H, XIE J, YUAN C W, et al. Application of ultrasound-guided fascia iliaca compartment block in elderly patients undergoing total hip arthroplasty[J]. J Clin Anesthesiol, 2022, 38(4): 356-360. DOI: 10.12089/jca.2022.04.004.
[26] ASLANLAR E, ASLANLAR D A, DOĞANAY C, et al. The validity and reliability of the Turkish version of the quality of recovery-15 (QoR-15) questionnaire[J]. Medicine, 2024,
103(16): e37867. DOI: 10.1097/MD.0000000000037867.
[27] CHHABRA A, DAVE M, JEENGER L, et al. Comparison of Quality of Recovery (QoR-15) following the administration of intravenous lignocaine and fentanyl in patients undergoing septoplasty under general anaesthesia: a double-blinded, randomised, controlled trial[J]. Indian J Anaesth, 2023,
67(4): 388-393. DOI: 10.4103/ija.ija_479_22.
[28] BRAMLEY P, MCARTHUR K, BLAYNEY A, et al. Risk factors for postoperative delirium: an umbrella review of systematic reviews[J]. Int J Surg, 2021, 93: 106063. DOI: 10.1016/j.ijsu.2021.106063.
[29] ZHU Q, JIANG G, ZHENG Y, et al. The effect of cognitive impairment based on Mini-Mental State Examination (MMSE) on suicidal tendency in patients with schizophrenia: a large cross-sectional study[J]. Schizophr Res, 2024, 269: 48-55. DOI: 10.1016/j.schres.2024.05.004.
[30] 孙倩倩, 余健, 程震. 连续髂筋膜间隙阻滞对老年患者髋部手术后认知功能及应激反应的影响[J]. 临床麻醉学杂志, 2021, 37(6): 603-606. DOI: 10.12089/jca.2021.06.010.
SUN Q Q, YU J, CHENG Z. Effects of continuous fascial iliac compartment block on postoperative cognitive function and stress in elderly patients undergoing hip surgery[J]. J Clin Anesthesiol, 2021, 37(6): 603-606. DOI: 10.12089/jca.2021.06.010.
(责任编辑:郑巧兰)
