The mangled upper extremity: a principled approach to management
2024-05-18EthanSongJesseMeaikeHannahLangdellSuhailMithani
Ethan Y.Song, Jesse D.Meaike, Hannah C.Langdell, Suhail K.Mithani
1Division of Plastic, Oral, and Maxillofacial Surgery, Duke University School of Medicine, Durham, NC 27710, USA.
2Division of Hand Surgery, Duke University School of Medicine, Durham, NC 27710, USA.
Abstract A mangled upper extremity often involves injury to soft tissue, bone, nerves, and vessels and presents a unique challenge to hand surgeons.The complexity of such injuries requires a multidisciplinary approach to achieve an optimal functional outcome.After obtaining a thorough history and performing a secondary survey, initial management is built upon a strong understanding of the likelihood of limb salvage.Initiation of antibiotics upon presentation, timely and thorough surgical debridement, and early revascularization efforts should be pursued.The surgical team should create a long-term plan involving skeletal stabilization and soft tissue reconstruction along with postoperative rehabilitation and social support.This article reviews current concepts of upper extremity limb salvage and recommendations for surgical management of the mangled extremity.Keywords: Mangled upper extremity, soft tissue reconstruction, revascularization
INTRODUCTION
The definition of a mangled extremity is a limb with an injury to at least three out of four components - soft tissue, bone, nerves, and vessels[1].Mangling injuries to the extremity present a significant challenge to the hand surgeon.Optimal outcomes require capability of all the levels of the reconstructive elevator as well as bony fixation strategies, and secondary surgeries.At the time of initial evaluation in the emergency department, it is imperative to adhere to Advanced Trauma Life Support (ATLS) guidelines[2].A mangling injury to the extremity can often be distracting from other serious, potentially life-threatening, injuries.It is crucial to have a thorough and systematic evaluation of the patient prior to addressing the injury to the extremity, adhering to the “life over limb” mantra.Initial evaluation of the extremity should include a thorough understanding of the history and mechanism of the injury, assessment of the injury, including the soft tissue deficit, degree of bony injuries, presence of contamination, and vascularity of the digits.Radiographs of the injured limb should be obtained in circumstances without hard signs of hemorrhage or ischemia[3].If the injury does not require an urgent operative intervention, wounds should be thoroughly irrigated and dressed in the emergency room as a temporizing measure prior to operative debridement and reconstruction.
The senior author has developed an algorithm to help conceptualize and guide the management of these injuries.
(1) Is it salvageable?
(2) Secondary survey
(3) Early reperfusion in the dysvascular extremity
(4) Have a long-term plan
(5) Build from a stable base
(6) Think outside the box
(7) Recognize the limits
IS IT SALVAGEABLE?
There are many variables to consider when determining whether an injury is deemed salvageable.The treating surgeon should consider patient characteristics, injury characteristics, and defect characteristics.Several scoring systems have been devised to aid in decision-making for the management of the mangled extremity, including the Mangled Extremity Severity Score (MESS) and Mangled Extremity Syndrome Index (MESI)[4,5].These have been developed based upon lower extremity trauma, and therefore, their application to upper extremity injuries has been questioned[6-8].A systematic review by Nayaret al.evaluating outcomes of primary amputation versus limb salvage in upper limb trauma found MESS scores to be neither specific nor sensitive in determining the need for amputation[8].The MESS and MESI scores are also not useful in predicting functional outcomes for patients with upper extremities[9].This is possibly due to physiologic and anatomic differences between the upper and lower extremities.Physiologic distinctions such as lower muscle mass of upper extremities compared to lower extremities may limit the effects of crush syndrome after a mangling injury[6].Unlike injuries to the popliteal artery in the lower extremity which can lead to significant ischemia distally, the rich collateral vascularization of the upper extremity may contribute to higher tolerated ischemic times[10].
More recently, the Mangled Upper Extremity Score (MUES) has been developed to specifically address upper extremity injuries.Based upon a retrospective review of 76 patients, eight injury characteristics were identified: patient age > 40, need for fasciotomy, need for bony fixation, bony defect present, need for revascularization, crush injury mechanism, degloving or avulsion present, and soft tissue defect > 50 cm2,with scores of 6 or more favoring primary amputation over salvage[11].MESI and MUES were more accurate measures compared to MESS, but both are based upon single, retrospective studies[10,11].There were few studies comparing long-term functional and psychological outcomes of primary amputation versus limb salvage, highlighting the need for studies analogous to the Lower Extremity Assessment Project (LEAP) for lower extremity trauma, to better inform these complex decisions[12].The authors identified three categories to consider - (1) global patient factors (namely uncontrollable hemodynamic instability); (2) limb-specific factors (extensive and concurrent soft tissue, bone, vascular, and/or nerve injuries and prolonged ischemia time); and (3) mechanism of injury factors (blunt arterial trauma and crush injuries).Amputation was generally performed when 2 of 3 factors were present.In the author’s experience, surgeons should be especially wary of degloving injuries with extensive zones of injury and those with extensive contamination,which carry a higher risk of invasive infections[13].Distal and sharp injuries have better prognoses than proximal traction and crush injuries[14,15].Industrial injuries may involve additional chemical damage, burns,and high-pressure injection injuries[16,17].
Clinical decision making is often left to the judgment and experience of the surgeon, though shared decision making involving the patient should be employed whenever possible.Limb salvage is a lengthy and complex journey, stretching over months to years, and complications may necessitate further surgery.Hansen argued that substantial morbidity would incur if multiple salvage attempts were made when success was unlikely[18].Furthermore, multiple revision surgeries may negatively impact the patient’s social environment of employment, family, and self-image[19].In some cases, primary amputation may achieve a better functional result and psychological recovery in a shorter period of time.Advances in prostheses and adjuvant surgical techniques to optimize prosthetic fit and control, such as regenerative peripheral nerve interfaces, targeted muscle reinnervation, and osseointegration, may eventually make primary amputation more appealing than multi-stage complex limb salvage attempts[20].However, revision surgeries after amputation may still be needed for heterotopic ossification, infection, neuromas, and contractures.
Overall, whenever possible, salvage should be attempted rather than proceeding with a primary amputation.Neumeister and Brown argue that salvaging sensate digits, even with minor restoration of movement, is preferred over the use of prosthetics[15].Current upper limb prosthetics fail to provide the same aesthetic and functional results compared to lower limb prostheses[15,21-23].A retrospective review by Tennentet al.of limb amputees in the military revealed that upper extremity amputees had significantly greater combined disability ratings than did lower extremity amputees[24].Up to 79% of patients with upper extremity have persistent pain and over 30% of amputees may abandon their prostheses[23,25,26].Only in select cases where patients suffer disabling injuries with significant soft tissue and neurovascular injury should primary amputation be indicated.
Oftentimes, an attempt at salvage is warranted, and in the acute setting, patients are not often able to have an informed discussion or are ready to cope with the possibility of an amputation.Assessment of viability is a dynamic process.Occasionally, salvage is attempted at the initial operation, only for the injured part to declare itself nonviable in the coming days, necessitating an amputation in a delayed setting.Heroic efforts at limb salvage are often attempted in mangling upper extremity injuries, but a realistic endpoint should be established.
SECONDARY SURVEY
The importance of the secondary survey cannot be overstated.Mangling injuries to the upper extremity are often severe and may distract the remainder of the team from other potentially life-threatening injuries.Standard ATLS algorithms should be followed when evaluating these patients to ensure that additional injuries are not overlooked[2].The secondary survey should include a detailed examination from head to toe.A relevant history should also be obtained, including the mechanism of injury and time of injury.Time since the injury is considered warm ischemia, and early revascularization attempts are critical to prevent continued tissue necrosis and reduce the risk of reperfusion injury[27].The mnemonic “AMPLE” is a useful reminder of the pertinent information and includes the patient’s allergies, medications, past medical history/pregnancy status, last meal, and events surrounding the injury.Coordinated teamwork and communication with the various surgical teams regarding the management of concomitant injuries is critical for a successful outcome.
At the time of presentation to the emergency department, antibiotic therapy should be initiated based on existing guidelines of open fracture treatment[28,29].According to the Eastern Association for the Surgery of Trauma (EAST) practice management guidelines, patients should be started on gram-positive coverage, and addition of gram-negative coverage (e.g., aminoglycoside) for Gustilo and Anderson type-III open fractures[29].Metronidazole can be added if there is suspicion of anaerobic bacterial contaminant[30].A retrospective study by Lacket al.in 137 patients with open fractures revealed that infection rates were increased if antibiotics were delayed > 1 h after injury[31].Tetanus status should also be updated in the emergency department.
The majority of bleeding in the upper extremity can be controlled with direct pressure or a pressure dressing.It is important to communicate with the initial evaluating emergency department team regarding immediate ligation of bleeding vessels, as this may complicate microsurgical repair.Any skeletal deformity or malalignment should be reduced as this can improve peripheral circulation.Careful timing of tourniquets is important, as prolonged use or overtightening can cause further ischemic or nerve injury[32].Pulse oximetry is a useful adjunct to assess the perfusion of the hand/digits if the clinical examination is unclear.In a retrospective study of twenty patients presenting with digital lacerations, injured digits ranged in pulse oximetry values from 53% to 92%, and all digits with a SpO2< 84% required operative intervention[33].Computed tomography (CT) or CT angiography imaging of the injured limb should be obtained in circumstances without hard signs of hemorrhage or ischemia warranting emergent operative intervention[3].Early imaging can also assist with surgical planning for future reconstruction.
EARLY REPERFUSION IN THE DYSVASCULAR EXTREMITY
Mangling extremity injuries with major vascular disruption deserve special attention.Increasing time without return of blood flow is associated with progressive tissue necrosis, neurologic impairment,compartment syndrome, and limb loss[34].This is especially true for vascular disruption at the forearm level and proximal.Digits can withstand warm ischemia times up to 12 h and cold ischemia up to 94 h with reports of successful digital replantation[35].However, with a more proximal vascular injury, more muscle is at risk of necrosing.Therefore, in these scenarios, minimizing the duration of muscle ischemia is imperative.

Figure 1.Demonstration of temporary vascular shunt placement (white arrow) to allow for early reperfusion of the left upper extremity in the setting of a conveyor belt injury.
In cases of an avascular, mangled upper extremity with an open fracture, the question arises as to whether to address the vascular injury or bony stabilization first.Particularly for proximal injuries, we recommend temporary vascular shunting as the first step.This can be achieved by securing a heparin irrigated 6-Fr suction catheter between the proximal and distal ends of the transected artery[36][Figure 1].This allows the team to focus on the other extensive bony and soft tissue injuries that often accompany these injuries while the muscle reperfuses, and definitive vascular repair or reconstruction can be safely performed at the end of the case[37].In situations with prolonged warm ischemia time > 4 h resulting from brachial artery disruption,it is wise to perform prophylactic fasciotomies in anticipation of ischemia-reperfusion related swelling and avoid a devastating compartment syndrome, especially in the setting of intra-operative blood loss > 100 mL,multiple arterial injuries, and open fracture[17,38].
Surgical debridement is warranted within the first 24 hours of the injury to prepare a clean wound bed and reduce the risk of infection[34].The full extent and degree of the injury can only be adequately assessed after a controlled wound exploration[39,40].Excisional debridement should involve skin, soft tissue, and even devitalized bone.Muscle viability may be tested via contractility[41].Structures that should be considered for conservative treatment are nerves and vessels[17,42].Debridement for vascularized mangled extremities can be performed under a tourniquet to enhance visualization of structures and lower the risk for iatrogenic injury,although it may also limit inspection of tissue viability due to lack of circulation[43].It is seldom possible to debride all necrotic tissue at the initial surgery, and additional trips to the operating room should be planned as the full extent of the wound declares itself.It is recommended for patients undergoing serial debridements to take culture specimens at each debridement and to repeat debridement until cultures become negative prior to wound closure[44].Barring any exposed critical structures, the wound can be managed in the interim with negative pressure wound therapy (NPWT), which has been shown to accelerate granulation, reduce swelling, decrease inflammatory mediators, and decrease deep infection rates of open fractures[45,46].
Debate exists over the utilization of high- or low-pressure pulse lavage for debridement.In vitro studies show that high pressure irrigation can cause bony and soft tissue injury, as well as driving bacteria and contaminants into tissue[47,48].However, clinical studies have not found any difference in outcomes.The fluid lavage of open wounds (FLOW) trial was a prospective, single-blinded randomized trial of 2,551 patients with open fractures which were irrigated with high, low, and very low-pressure pulse lavage with either saline solution or Castile soap.While there were higher re-operation rates for patients who were irrigated with Castile soap, there were no significant differences found in re-operation rates for wound healing or wound infection reasons between high and low pressures[49,50].
HAVE A LONG TERM PLAN
The management of these severe mangling injuries frequently involves multiple operations over the course of many months.It is crucial to begin by assessing which parts are missing and what needs to be replaced.The surgeon should diagram all steps of the anticipated reconstruction so as not to burn any bridges for subsequent steps.These are challenging cases, and the patient should be counseled on appropriate goals,expectations, and timelines.This is a shared decision and the patient specific functional goals and desire to undergo a complex, multistage procedure should be understood before embarking on this long journey.Psychological support, cognitive behavioral therapy, and social support for patients are critical in the longer postoperative period, as post-traumatic stress disorder and depression are common[51,52].Group therapy can also be another helpful method to encourage patients during their recovery[53].
BUILD FROM A STABLE BASE
It is wise to restore the bony relationships at the index operation.If there is instability, the surgeon should work to create a stable platform.Fixation options for the upper arm include the external fixator or plate fixation, for the forearm, external fixator or bridge plate, and in the hand and fingers, Kirshner wires or internal fixation [Figure 2].In the hand and fingers, soft tissue coverage may be tenuous at the initial stages,so the authors prefer the judicious use of K-wires.Rigid fixation enables early active motion when possible.If an external fixator is used, it is recommended to place the pins outside the zone of injury in a configuration that does not interfere with future wound exploration[43].While external fixator placement warrants the need for a second surgery, additional operations are often needed regardless for further debridement and soft tissue reconstruction.Therefore, the authors give their best effort to restore bony relationships without agonizing over perfection in the initial stages, knowing revisions can be performed later after soft tissues have stabilized.
The minimal requirements for the hand are a stable wrist and two opposing sensate digits.If the wrist is unstable, all flexion and extension forces generated by the forearm muscles will be dissipated across the wrist, making finger motion ineffective.Only one digit requires motion, while the other can be a stable post.However, both digits must be stable to withstand the force required to generate pinch.A cleft must be present between the digits to accommodate larger objects and allow for prehensile movement.Most importantly, the digits must be sensate (two-point discrimination less than 10-12 mm) and pain-free;otherwise, they provide little benefit over a prosthesis[54].
In the hand, one can typically find stability from the carpus or an intact ray and build outward.In combined hand and wrist trauma, one needs to restore stability across the wrist.This can be achieved with either an external fixator or a bridge plate.In the setting of high-energy injuries with complete carpal loss, the author’s strategy is to prepare the wrist for an eventual arthrodesis.The wrist can be initially stabilized with an external fixator and transitioned to spanning hardware.In the setting of gross contamination or tenuous soft tissue coverage, the authors prefer a staged approach with initial external fixation followed by placement of an antibiotic spacer with bridging fixation, with subsequent bone graft to complete the fusion.Elbow and upper arm injuries are rarely amenable to initial internal fixation, only if it is a clean injury.Oftentimes, external fixators are the primary mode of fixation.One should shorten the humerus as needed to achieve bony apposition.At this level, shunting in the setting of a dysvascular limb is critical.

Figure 2.(A, B) A volar shear distal radius fracture with radiocarpal dislocation, multiple CMC joint dislocations, and 4th and 5th metacarpal neck fractures; (C) The CMC dislocations and metacarpal fractures were stabilized with multiple Kirschner wires; (D) The radius was addressed with a volar plate and stability about the wrist was obtained with a spanning dorsal plate.CMC:Carpometacarpal.
Scenarios with bone loss or severe comminution in contaminated wounds may require bone shortening to create a better contact surface of healthy tissue.Bone shortening may also help facilitate the approximation of other injured structures such as nerves, vessels, and tendons, thereby reducing the need for grafts[43].However, care should be taken to avoid excessive bony shortening as it can lead to mechanical insufficiency,particularly in the forearm[9].The maximum amount of shortening that is functionally tolerated is 5 cm in the humerus, 4 cm in the forearm, and 1-1.5 cm in the phalanges and metacarpals[43,55].Bone grafting can be considered for spanning bony defects.It is recommended that for defects > 4 cm and < 6 cm, nonvascularized bone graft from the iliac crest can be utilized[9].For defects > 6 cm, a free vascularized fibula bone flap with or without a soft tissue skin paddle for monitoring is often chosen.However, these forms of bony reconstruction should only be pursued when the wound is clean, and the risk of infection is minimal.Antibiotic cement spacers and NPWT are viable temporizing options in the interim.
Tendon reconstruction should adhere to the primary goal of improved function and early range of motion.Primary repair of tendons is the preferred first-line management.Frayed ends of tendon should be freshened prior to primary repair, and the two ends should be repaired without excessive tension or subsequent gapping.Tendon grafting can also be utilized where there are gaps, with common autologous sources being the palmaris longus, extensor indicis proprius, and flexor digitorum superficialis tendons.Silicone tendon rods can be used to reduce the problems associated with scar tissue when one needs to perform delayed or staged reconstructions[56].Tendon transfers are employed in situations with multiple tendon injuries or significant loss of muscle mass[43].Lastly, tenodesis is an option when there is a complete loss of muscle mass and no local options available for tendon transfer.Current recommendations for the timing of tendon reconstruction are when soft tissue coverage of the repair or reconstruction can be guaranteed.Otherwise, the risk of rupture from desiccation, adhesions, and tendon necrosis increases[57].
Nerve repair and reconstruction follow similar management principles as with tendons.If possible, nerves should be primarily repaired without tension after sharp debridement.Nerves sustaining crush injury or contamination need to be trimmed further to healthy tissue outside the zone of injury, which often leads to widened nerve gaps.Small nerve gaps < 3 cm may be managed with nerve conduits, which have been reported to have excellent outcomes for digital nerve injury[58].For gaps up to 5 cm, nerve allografts can be utilized.For larger spanning defects, the gold standard is the usage of nerve autografts.Donor sources include the sural nerve, given its length and low donor site morbidity.Other less common choices include medial and lateral antebrachial cutaneous nerves.Fibrin glue application can augment the coaptation as it has been shown to reduce inflammation, improve axonal regeneration, and reduce operative time[59,60].Nerve transfer can also be considered in special cases with end-to-side repair; however, this can be challenging at the index presentation due to the altered anatomy and contamination of the mangled extremity.
In a mangled extremity, restoring a durable soft tissue envelope over critical structures poses a unique challenge.However, utilization of the armamentarium within the reconstructive ladder provides a principled approach for soft tissue coverage.Collaboration and communication between the orthopedic and plastic and reconstructive surgery teams for planning and staging of reconstruction are vital for favorable outcomes.Local muscle flaps such as the brachioradialis or flexor carpi ulnaris flap can be used to cover small defects[61].However, in avulsion or crush injuries, there likely will not be viable local tissue due to the large zone of injury.In these cases, regional flaps designed outside the zone of injury such as the latissimus muscle flap can be considered for large spanning defects.At the top of the reconstructive ladder are free flaps, which can provide healthy tissue to the injured area.There exists a debate on the choice of muscle or fasciocutaneous flaps for coverage.Historically, muscle flaps have been used for their rich vascularity to combat infection, reduce morbidity, and reduce healing times.Fasciocutaneous flaps, on the other hand,can provide a better gliding surface for tendons than muscle flaps[62].A recent multicenter outcomes analysis by Choet al.of 518 free flaps utilized for limb salvage found that fasciocutaneous free flaps had comparable rates of limb salvage and functional recovery compared to free muscle flaps[63].
The optimal timing of soft tissue coverage remains unclear and should be evaluated on a case-by-case basis.Ideally, soft tissue reconstruction should only be attempted in a clean wound bed.Historically, based on the original work of Gustiloet al.on open fractures, wounds were left open for up to 7 days with serial debridements before coverage[64].More recently, it has been observed that earlier soft tissue coverage is associated with improved limb salvage outcomes[65-67].Godina showed that coverage of wounds < 72 h from injury compared to delayed reconstruction would significantly lower infection rates[67].Derderianet al., in a retrospective review of 133 patients undergoing free tissue transfer for traumatic upper extremity defects,recommended coverage between 6 and 21 days as they found a decrease in flap failure, recipient site infection, and osteomyelitis[66].As a whole, the data suggest that the most important factor in reducing complication rates from infection is not strict adherence to a time for wound closure, but rather obtaining a clean wound bed.
THINK OUTSIDE THE BOX
No two mangling extremity injuries are the same, and these injuries challenge the surgeon to come up with unique solutions to optimize outcomes.Three salient points have consistently arisen in the author’s treatment of these injuries: (1) flow-through flaps; (2) spare parts surgery; and (3) nonmicrovascular options for salvage.
Complex injuries with severe soft tissue deficits and arterial defects are well suited for reconstruction with flow-through flaps.For large soft tissue deficits, the authors prefer using the lateral circumflex femoral system as it provides a long pedicle length of good caliber and can be combined with skin, fascia, and/or muscle that can be tailored to address the soft tissue deficit.Flow-through flaps allow the surgeon to reconstitute axial blood flow by reconstructing the arterial gap, and can bridge the artery and concomitant vein simultaneously.Additionally, flow-through flaps are combined with another free flap depending on the defect[68].For small volar defects on the digits, the authors have found venous flow-through flaps useful to simultaneously resurface the volar skin defects and reconstruct the segmental digital artery defect[69].
Peng and Lahiri define spare-part surgery as “scavenging tissue components from nonsalvageable parts of the injured extremity to reconstruct more-critical parts of the hand”[70].
They list 5 prerequisites for spare-parts surgery:
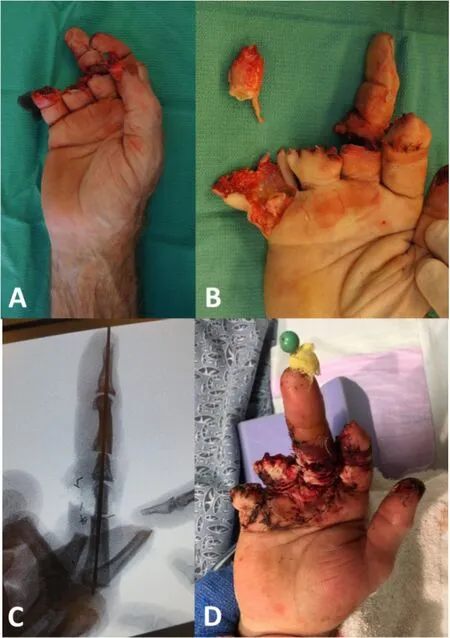
Figure 3.(A) Industrial accident with complete amputation of the small and ring fingers with partial amputations of the index and long fingers.The small, ring, and index fingers were not salvageable.The long finger was perfused, but there was destruction of the PIP joint;(B) A revision amputation of the small finger was performed with isolation of its vascular pedicle; (C, D) The PIP joint of the small finger was transferred to the long finger as a free vascularized joint to replace the long finger PIP joint and restore length.
(1) The spare parts need to have anatomical integrity and should preferably lie outside the zone of direct trauma.
(2) Ischemia time should be within salvageable limits for revascularization for composite spare parts.
(3) Reconstruction should offer better global function than primary amputation.
(4) The spare part should serve a greater function when used for reconstruction of other parts than when replanted in its anatomical location.
(5) The use of spare parts should not exclude harvesting healthy tissue if it is necessary to obtain maximal hand reconstruction.If all the digits can be salvaged with the use of tissue from healthy donor sites, then that strategy should be adopted.
Prior to discarding any tissues, one should thoughtfully evaluate whether any of the structures can be repurposed.If these components are within the zone of injury, they should be scrutinized prior to the use,especially vascular and nerve grafts.Nonsalvageable components can be used as skin grafts, nerve grafts,arterial or vein grafts, and bone grafts for reconstruction of the remaining hand or the limb[71].The nonsalvageable components may also provide vascularized tissues, such as pedicled fillet skin flaps, pedicled joint flaps, or heterotopically transplanted digits to reconstruct more important digits[72][Figure 3].
Surgeons proficient in microvascular techniques should also consider non-microvascular solutions in their armamentarium as this may provide a better reconstructive solution for a variety of reasons.The authors have had great success utilizing dermal regeneration templates (DRT) both as a temporary dressing that greatly simplifies wound care between reconstructive stages and as a bridge to definitive coverage with skin grafting, especially to resurface the dorsum of the hand [Figure 4].Similarly, Valerioet al., in a retrospective study of 60 patients with contaminated combat-related upper extremity soft tissue injuries, revealed completed healing without complication with staged debridement with DRT placement followed by fullthickness skin grafting[73].The groin flap is a utilitarian flap that provides thin, supple, soft tissues that can be used to cover large soft tissue deficits on the hands and should be an essential component of every hand surgeon’s armamentarium [Figure 4].
RECOGNIZE THE LIMITS
It is vital to set realistic expectations at the beginning of the journey, and the patient should understand that restoration of normal hand and upper extremity function is not typically achievable.The reconstructive sequence should have multiple exit points at which the patient can walk away.There are multiple secondary surgeries that can be performed to optimize outcomes, including scar revision, tenolysis, corrective osteotomies, and flap thinning.However, the adage “the enemy of good is better” should be kept in the forefront of the surgeon’s mind, and the wise surgeon knows when further attempts at improvement are futile.
CONCLUSION
In summary, the surgeon should be cognizant of the importance of the initial management steps including initiation of antibiotics, thorough irrigation and debridement, provisional bony fixation, and inventory of damaged parts.These injuries often require multistage reconstructions, so appropriate long-term planning is paramount to success.Bony relationship should be restored to the best of one’s ability in the first stage with either external fixation or bridge plating.Tendon, nerve, and soft tissue reconstruction should follow the reconstructive ladder.It is important to know when to stop operating, and plans should allow the patient to walk away at multiple points in the journey.Lastly, one may need to go down, rather than up, the reconstructive ladder to achieve successful results.

Figure 4.(A, B) A complex circumferential degloving injury with gross contamination after a motor vehicle collision; (C) An external fixator was placed to stabilize the carpus and the volar soft tissue deficit was reconstructed with a pedicled groin flap; (D) The dorsal soft tissue deficit was addressed with placement of a dermal regeneration matrix; (E, F) 3 weeks later, the groin flap was divided and inset, and split-thickness skin grafting was performed on the dorsum of the hand.
DECLARATIONS
Authors’ contributions
Contributed to the writing, editing, and review of the manuscript: Song EY, Meaike JD, Langdell HC,Mithani SK
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
Dr.Suhail Mithani serves as a consultant for Integra LifeSciences.
Ethical approval and consent to participate
In accordance with the Duke University Institutional Review Board ethics policies, an ethical review was not required to undertake this research.All participants provided written consent for their information to be used in this study.
Consent for publication
Written informed consent was obtained from patients.
Copyright
© The Author(s) 2024.
杂志排行
Plastic and Aesthetic Research的其它文章
- Early lymphaticovenous anastomosis in lymphedema management: a pilot study
- The emerging role of sentinel lymph node biopsy in oral cavity and oropharyngeal carcinomas
- Therapeutic management of the painful nerve: a narrative review of common rehabilitation interventions
- Role of transoral robotic surgery in the salvage setting: pitfalls and challenges
- Systematic review on the centrocentral anastomosis technique for the surgical treatment of traumatic neuromas