Therapeutic utility of human umbilical cord-derived mesenchymal stem cells-based approaches in pulmonary diseases: Recent advancements and prospects
2024-03-24MinMengWeiWeiZhangShuangFengChenDaRuiWangChangHuiZhou
Min Meng,Wei-Wei Zhang,Shuang-Feng Chen,Da-Rui Wang,Chang-Hui Zhou
Abstract Pulmonary diseases across all ages threaten millions of people and have emerged as one of the major public health issues worldwide.For diverse disease conditions,the currently available approaches are focused on alleviating clinical symptoms and delaying disease progression but have not shown significant therapeutic effects in patients with lung diseases.Human umbilical cord-derived mesenchymal stem cells (UC-MSCs) isolated from the human UC have the capacity for self-renewal and multilineage differentiation.Moreover,in recent years,these cells have been demonstrated to have unique advantages in the treatment of lung diseases.We searched the Public Clinical Trial Database and found 55 clinical trials involving UC-MSC therapy for pulmonary diseases,including coronavirus disease 2019,acute respiratory distress syndrome,bronchopulmonary dysplasia,chronic obstructive pulmonary disease,and pulmonary fibrosis.In this review,we summarize the characteristics of these registered clinical trials and relevant published results and explore in depth the challenges and opportunitiesfaced in clinical application.Moreover,the underlying molecular mechanisms involved in UC-MSC-based therapy for pulmonary diseases are also analyzed in depth.In brief,this comprehensive review and detailed analysis of these clinical trials can be expected to provide a scientific reference for future large-scale clinical application.
Key Words: Pulmonary diseases;Mesenchymal stem cells;Human umbilical cord;Cell therapy;Clinical trials
INTRODUCTION
Pulmonary diseases across all ages are mainly caused by trauma,air pollution,long-term smoking,population aging,and various respiratory virus infections,such as coronavirus disease 2019 (COVID-19),and exert tremendous negative impacts on health status,quality of life,and socioeconomic costs[1,2].In the last decade,the increasingly high rates of morbidity and mortality due to acute and chronic lung diseases have led to ongoing burdens on public health and health care systems worldwide[3].According to the systemic analysis for Global Burden of Study 2017,chronic respiratory diseases,including asthma,chronic obstructive pulmonary disease (COPD),idiopathic pulmonary fibrosis (IPF),pulmonary arterial hypertension,and occupational diseases,have affected more than 500 million people globally[4].Acute respiratory distress syndrome (ARDS) is recognized as the most severe form of acute lung injury (ALI) according to the 2012 Berlin definition[5].ARDS is commonly caused by sepsis,smoke inhalation injury,near-drowning,severe pneumonia,or pulmonary contusion and is present in approximately 10% of all patients in intensive care units worldwide[6,7].The mortality rate for ARDS patients has remained high,at 30%-40%,in most clinical studies[8,9].Regardless of the pathophysiology of chronic respiratory disease or ALI,these diverse conditions are usually associated with inflammatory cell infiltration,inflammation-induced disruption of the alveolar epithelial and endothelial barrier,a decrease in alveolar fluid clearance,associated cytokine release,airway inflammation and remodeling,and pulmonary fibrosis development[3].Currently available therapeutic approaches (e.g.,antibiotic/anti-inflammatory drugs,corticosteroids,specific cytokine inhibitors,bronchodilators,artificial respiratory support,mechanical ventilation,and restricted fluid input) are focused on alleviating clinical symptoms and delaying disease progression[10].Hence,the development of novel therapeutic approaches for pulmonary diseases is of paramount significance for attenuating immune responses and fostering tissue regeneration.
Mesenchymal stem cells (MSCs) have unique immunomodulatory,regenerative and differentiation properties,and MSC-based therapies have received increasing attention for the treatment of pulmonary diseases,including COVID-19,ALI/ARDS,bronchopulmonary dysplasia (BPD),COPD,IPF and silicosis[11].MSCs are nonhematopoietic stem cells with multilineage differentiation capacities and can be isolated from bone marrow (BM),umbilical cord (UC),adipose tissue (AT),placenta,peripheral blood (PB),lung,and other tissues[12,13].Although MSCs have numerous potential therapeutic applications,they can also have detrimental effects depending on the microenvironment,and the tumorigenicity of transplanted MSCs is a current concern that has been well documented through the use of single-cell transcriptomes[14].In addition,the heterogeneity of MSCs is determined by multiple factors,such as donors,tissue sources,cell populations,culture conditions,cell isolation techniques,and cryoprotective and thawing protocols,and can also lead to inconsistent clinical application efficacy[15].All these factors,to some extent,constrain the clinical efficacy and application of MSCs.BM-derived MSCs (BM-MSCs) were first discovered and are considered the main source for clinical application;however,they eventually degrade,exhibiting a loss of proliferation and senescence[16].Among these sources,UC-MSCs have emerged as a promising candidate due to their easy collection,noninvasive isolation methods,rapid proliferation ability,low immunogenicity,few ethical concerns,superior immunological regulation potential and anti-inflammatory effects[17-21].More importantly,UC-MSCs are superior for standardization and large-scale production for disease treatment.MSCs from these neonatal tissues possess increased proliferative capacityin vitro[22].Moreover,the number of MSCs obtained from UC specimens is far greater than that obtained from BM or AT and is not limited by donor age,which partially eliminates the impact of cell heterogeneity on clinical treatment and outcome analysis[23,24].In terms of the therapeutic benefit of UC-MSCs in patients with pulmonary diseases,an increasing number of clinical studies have demonstrated the safety and efficacy of UC-MSCs in regulating the function of immune cells,alleviating the inflammatory response,improving pulmonary function,enhancing lung tissue regeneration and repair,and attenuating lung fibrosis[3].Therefore,considering these advantages,UC-MSCs are recommended to be considered as appropriate sources of MSCs for the management of pulmonary diseases in both pediatric and adult populations.In this review,we provide a detailed summary of clinical trials and results related to the use of UC-MSCs in the treatment of lung diseases and explore in depth the challenges and opportunities faced in the clinical application of these cells.
UNDERLYING MOLECULAR MECHANISMS OF UC-MSCS IN PULMONARY DISEASES
UC-MSCs are located mainly in the umbilical vein subendothelial,subamnion and perivascular regions and in Wharton’s jelly (WJ);these cells are composed mainly of sponge-like structures woven with collagen fibers,proteoglycans and embedded stromal cells[25,26].In recent years,there has been enormous progress in understanding the similarities and differences between MSCs derived from various human tissues[27].Compared to AT-MSCs and BM-MSCs,UC-MSCs are easier to obtain and culture due to the noninvasive collection method used after birth,the ease ofin vitroexpansion and ethical access[28].In addition,UC-MSCs exhibit lower immunogenicity,greater proliferation and differentiation potential,a slower senescence rate,and greater anti-inflammatory and immunomodulatory effects than AT-MSCs and BM-MSCs,suggesting that UC-MSCs might be a better alternative for the treatment of pulmonary diseases,especially during the COVID-19 pandemic[13,19-21].UC-MSCs have shown safety and efficacy in clinical trials for a variety of pulmonary diseases.Furthermore,UC-MSCs have been demonstrated to inhibit inflammation and fibrosis and accelerate the regeneration of functional lung tissue,representing a relatively effective therapy with promising results[29].The potential mechanisms of action of UC-MSCs in patients with lung-related diseases include immunomodulatory and antiinflammatory effects,regenerative and differentiation properties,and antimicrobial effects (Figure 1).
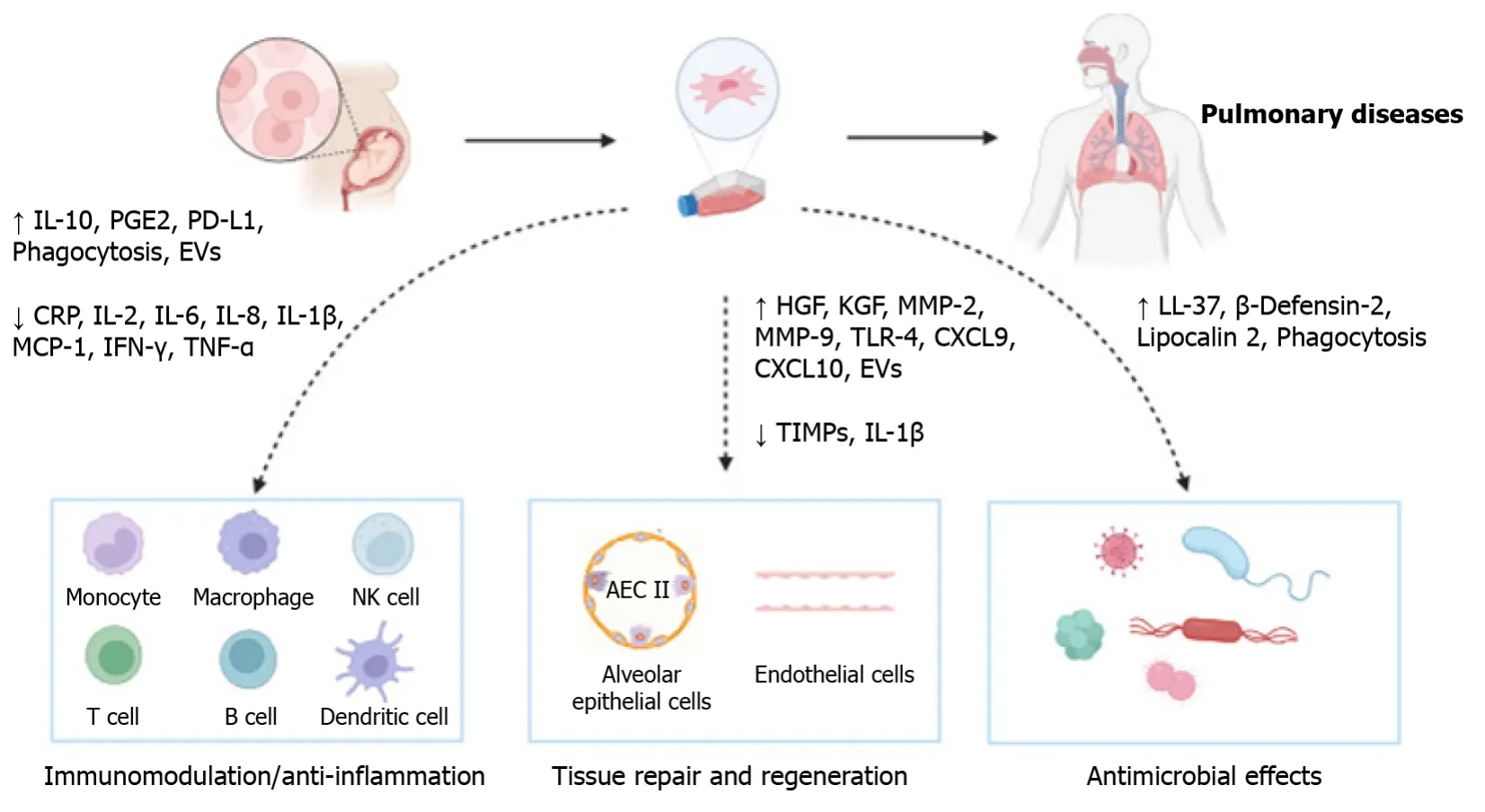
Figure 1 Potential mechanisms of umbilical cord-derived mesenchymal stem cells therapy in pulmonary diseases.The therapeutic effects of umbilical cord-derived mesenchymal stem cells in treating pulmonary diseases involve multiple mechanisms,such as the immunomodulatory and anti-inflammatory functions,the regenerative and differentiation properties,and the antimicrobial effects.IL: Interleukin;PGE2: Prostaglandin E2;PD-L1: Programmed cell death protein ligand 1;EVs: Extracellular vesicles;CRP: C-reactive protein;MCP: Monocyte chemoattractant protein;IFN: Interferon;TNF: Tumor necrosis factor;HGF:Hepatocyte growth factor;KGF: Keratinocyte growth factor;MMP: Matrix metalloprotease;TLR: Toll-like receptor;CXCL: C-X-C motif chemokine ligand;TIMP:Tissue inhibitor of matrix metalloproteinase;NK: Natural killer;AEC: Alveolar epithelial cell.
The immunomodulatory and anti-inflammatory properties of UC-MSCs have been extensively studied.The modulation of host innate and adaptive immune responses by UC-MSCs is mediated by direct cell-to-cell contact and paracrine effects.Briefly,the majority of exogenous UC-MSCs can migrate to the injured lung after intratracheal administration and directly interact with immune cells,such as monocytes,macrophages,natural killer (NK) cells,T cells,B cells,and dendritic cells.A previous study demonstrated a short survival period of infused MSCs and a lack of distribution of viable MSCs beyond the lungs[30].The rapid clearance of infused UC-MSCs from the lungs is largely mediated by phagocytosis by monocytes,which induces phenotypic and functional changes in monocytes and triggers an immunomodulatory response[31].UC-MSC administration in lipopolysaccharide (LPS)-induced ALI mice inhibits the expression of proinflammatory cytokines [interleukin (IL)-1β,tumor necrosis factor (TNF)-α,monocyte chemoattractant protein (MCP)-1,IL-2,and interferon (IFN)-γ],enhances the expression of the anti-inflammatory cytokine IL-10,and reduces macrophage infiltration into injured lung tissue through prostaglandin E2 (PGE2)-dependent reprogramming of host macrophages to promote their expression of programmed cell death protein ligand 1[8].IL-10 overexpression in UCMSCs has been demonstrated to attenuateEscherichia coli(E.coli)-induced lung injury and increase macrophage functionviathe enhancement of macrophage phagocytosis and elimination ofE.coli[32].Anin vitromodel of PB mononuclear cell(PBMC) coculture with UC-MSCs demonstrated an immunomodulatory effect on PBMCs,namely,an increase in neutrophil activation,phagocytosis and leukocyte migration;activation of early T-cell markers;and a decrease in effector T cells and the senescent effector CD4.UC-MSCs exert their potent immunomodulatory effects through a PGE2-mediated mechanism,and a large amount of PGE2 produced by inflammatory cytokine-activated UC-MSCs is the principal mediator of immunosuppressive activities[33].UC-MSC infusions significantly reduce the secretion of inflammatory biomarkers such as C-reactive protein (CRP),IL-6,IL-8,and TNF-α in COVID-19-induced ARDS patients[20].MSCs interact with dendritic cells,regulating the balance between proinflammatory T-helper 1 (Th1) cells and anti-inflammatory Th2 cellsviaa shift toward the Th2 phenotype[34,35].UC-MSC therapy has an inhibitory effect on overactive Tlymphocyte populations (CD8-CXCR3 and CD56-CXCR3) associated with cytokine storms,but the increase in CD4-CXCR3 in the UC-MSC group indicates the proliferation of these Th1 populations[36].Recent studies have shown that UC-MSC transplantation leads to a decrease in inflammatory markers,such as the erythrocyte sedimentation rate and CRP level;more rapid recovery of blood lymphocytes;and reduced surfactant D,one of the main markers of lung injury.On the other hand,the production of proinflammatory cytokines,such as induced protein 10 kDa,macrophage inflammatory protein-1α,and granulocyte colony-stimulating factor,could suggest a greater immunomodulatory effect of MSCs than immunosuppression in COVID-19 patients[37].Additionally,UC-MSC-derived extracellular vesicles (EVs) could mitigate the inflammatory response,restore the viability of cells and reduce the production of proinflammatory cytokines such as IL-8 and IL-1β in both LPS-andE.coli-induced lung injury models[38].MSC-derived EVs can interact with immune cells and enhance macrophage phagocytosis through EV-mediated mitochondrial transfer[39].
MSCs,including UC-MSCs,possess regenerative and differentiation properties that contribute to tissue repair and regeneration.MSCs have been shown to stimulate local tissue regeneration by secreting paracrine factors associated with angiogenesis,antifibrosis effects and remodeling responses[40].UC-MSCs secrete many molecules with paracrine effects that promote pulmonary alveolar regeneration and endothelial cell migration and proliferation,including angiopoietin-1,hepatocyte growth factor (HGF),epidermal growth factor,keratinocyte growth factor (KGF),vascular endothelial growth factor,MCP-1,C-X-C motif chemokine ligand (CXCL) 5 and matrix metalloprotease (MMP)[41].UC-MSCs are more effective at restoring alveolar fluid clearance and protein permeability in influenza A (H5N1)-associated ALI and possess functional and practical advantages over conventional BM-MSCs[42].In terms of their differentiation functions,UCMSCs can be induced to differentiate into type II alveolar epithelial cells (AEC II),which are regarded as the progenitor cells of pulmonary epithelium and the target cells of pulmonary fibrosis[43].Inin vitroexperiments,UC-MSC-derived AEC II were reported to be able to alleviate pulmonary fibrosis through regulating apoptosis mediated by β-catenin[44].A recent study demonstrated that UC-MSCs ameliorate lung injury in ARDS and regulate Yes-associated protein to facilitate AEC II differentiation[45].Furthermore,microvesicles derived from UC-MSCs were able to enhance alveolar development by promoting AEC II proliferation and ameliorating lung inflammation in an antenatal rat model of BPD[46].In addition,UC-MSCs have antifibrotic properties and can secrete a variety of cytokines that effectively reverse pulmonary fibrosis[47].UC-MSCs can alleviate bleomycin-induced pulmonary fibrosis in mice,and the overexpression of HGF has been proven to augment the antifibrotic effect of UC-MSCs by interacting with IL-17-producing cells in fibrotic lungs[48].By demonstrating the reduction in inflammation and fibrosis induced by bleomycin-induced lung injury induced by UC-MSCs,a study showed that UC-MSCs increased MMP-2 levels and downregulated lung cytokine and tissue inhibitor of matrix metalloproteinase expression[49].In coculture system studies,UC-MSCs elevated MMP-9 levels in pulmonary macrophages,released hyaluronan into the medium and promoted the expression of toll-like receptor-4(TLR-4) in the lung for alveolar regeneration[50].In the context of the molecular and cellular behavior of UC-MSCs,a subcluster of IFN-sensitive macrophages,which were identified by using cell sequencing after infusion,increased their expression of CXCL 9 and CXCL 10,which recruited more regulatory T cells into the injured lung;this indicated that UCMSCs can attenuate pulmonary fibrosisviamacrophages[51].Moreover,a human UC mesenchymal cell-conditioned medium was shown to decrease the level of oxidative stress,proinflammatory cytokines,and malondialdehyde,which caused restorative and prophylactic effects against pulmonary fibrosis in a model of IPF[52].
In addition to their immunomodulatory and differentiation abilities,UC-MSCs also exhibit antimicrobial effects in patients with bacterial or viral pneumonia and the ensuing ALI.In anin vitrostudy,paracrine mediators such as KGF,antimicrobial polypeptides,defensins,and lipocalin 2 secreted by MSCs were found to enhance bacterial clearance[53,54].Alternatively,the soluble paracrine factors released by MSCs,such as IL-10,PGE2,TNF-α-stimulated gene 6 and IL-6,also had preventive effects against microorganisms[54,55].Antimicrobial peptides,such as the human cathelicidin hCAP-18/LL-37,exhibit direct antimicrobial activity against a series of related pathogens,including fungi,viruses,and both gram-positive and gram-negative bacteria[56].Furthermore,β-defensin-2 (BD-2),which is secreted by UC-MSCs through the TLR-4 signaling pathway,is a critical paracrine factor that mediates the antibacterial and anti-inflammatory effects of these cells againstE.coli-induced ALI in mice[57].Anin vitrostudy demonstrated that UC-MSCs possessed direct antimicrobial effects against bacteria and could alleviate antibiotic resistance,which was mediated partly by secretion of cathelicidin LL-37 and BD-2 and upregulation of outer membrane protein expression during bacterial infection[58].In terms of the therapeutic effects of UC-MSCs onE.colipneumonia,UC-MSCs were effective at reducing ALI,decreasing the bacterial load,improving oxygenation,reducing histological injury,and ameliorating the level of inflammatory markers[59].On the other hand,the enhancement of macrophage phagocytosis and macrophage killing ofE.coliwas proposed as another main mechanism of the antimicrobial effects of IFN-γ-primed UC-MSCs[60].
OVERVIEW OF CLINICAL TRIAL REGISTRATIONS OF UC-MSCS FOR PULMONARY DISEASES
As of November 2023,when we searched for the keywords “human umbilical cord-derived mesenchymal stem cells” or“umbilical cord mesenchymal stem cells” or “UC-MSCs” and “pulmonary disease” or “coronavirus disease 2019” or“COVID-19” or “acute respiratory distress syndrome” or “ARDS” or “bronchopulmonary dysplasia” or “BPD” or“chronic obstructive pulmonary disease” or “COPD” or “pulmonary fibrosis” or “PF” in the Public Clinical Trial Database (https://ClinicalTrials.gov/),55 clinical trials of pulmonary diseases worldwide were systematically reviewed;these diseases included COVID-19 (n=17),ARDS (n=14),BPD (n=18),COPD (n=3),and PF (n=3).The geographical location and distribution of these clinical trials are shown in Figure 2.The clinical trials were conducted in 13 countries.Twenty-four clinical trials were conducted in China,followed by the United States,which hosted 9 trials.Korea was in third place with 7 trials.Clinical trials of pulmonary diseases have been increasingly conducted in developed and developing countries.

Figure 2 The geographical location and distribution of the clinical trials in pulmonary diseases.
The characteristics of the clinical trials,including study design,status and phase,were analyzed and counted(Figure 3).Thirty-two clinical trials were open-label;1 was single-blinded for the participants;3 were double-blinded for the participants and care providers;11 were triple-blinded for the participants,care providers,and investigators;7 were quadruple-blinded for the participants,care providers,investigators,and outcome assessors;and 1 was not described.Twenty-nine clinical trials were randomized,7 were nonrandomized,and 19 did not provide relevant information.The intervention models included single-group assignment (n=17),parallel assignment (n=33),and sequential assignment(n=2),while 3 were not described.The recruitment statuses of the clinical trials were as follows: Recruiting (n=16),completed (n=11),active but not recruiting (n=5),not yet recruiting (n=4),withdrawn (n=4),or unknown (n=15).The majority of clinical trials were mainly in the early phases,such as phase I studies evaluating safety (n=24),phase II studies evaluating efficacy (n=11),or combined phase I/II studies (n=12).Additionally,only a very small number of clinical trials were phase III studies to determine pragmatic effectiveness (n=2);1 study was a combined phase II/III trial,and there were no phase IV trials to monitor long-term effects.Five trials did not specify the phase.The specific content and results are described as follows.
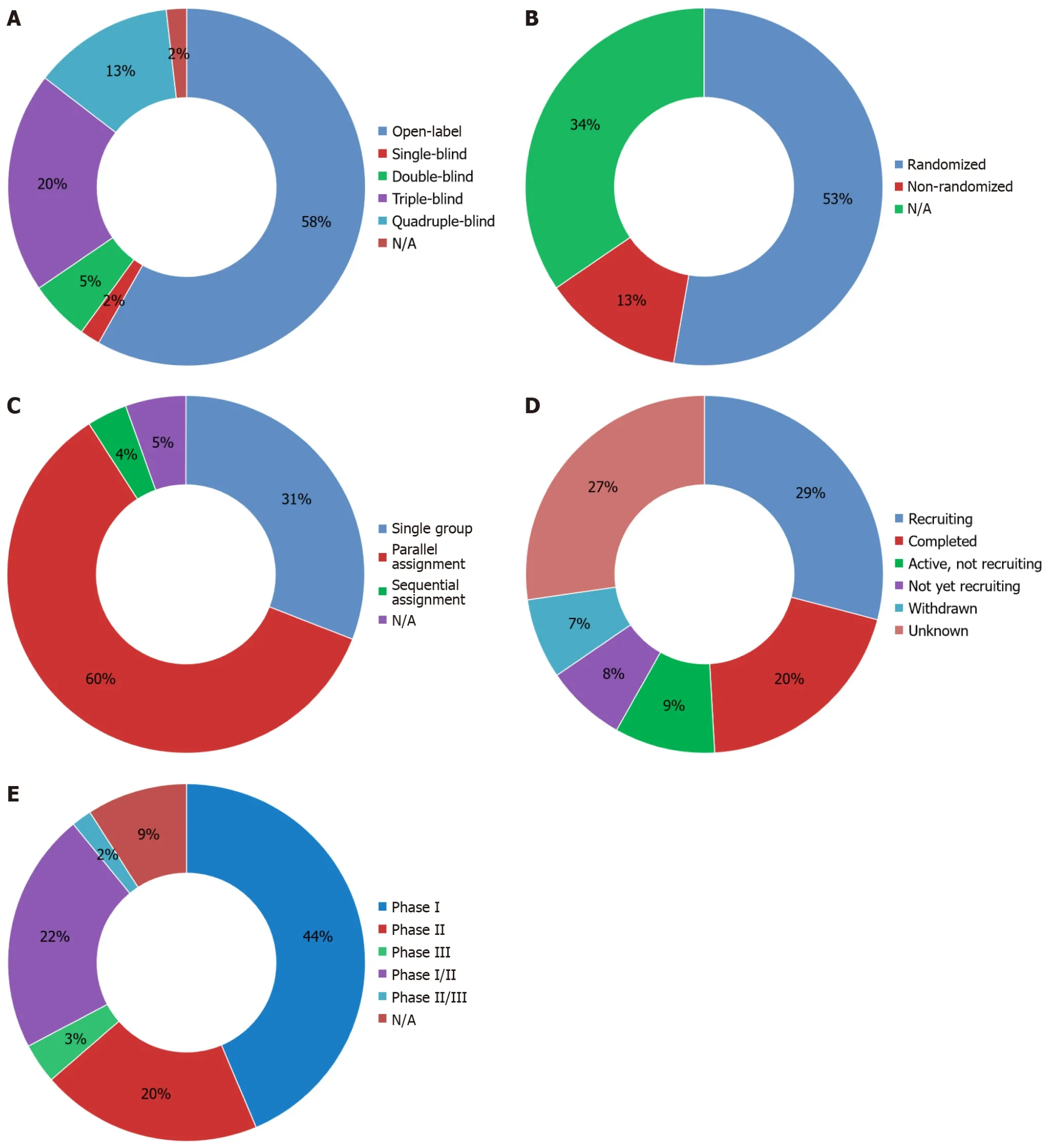
Figure 3 Characteristics of clinical trials involving umbilical cord-derived mesenchymal stem cells therapy for pulmonary diseases. A:Masking of clinical trials;B: Allocation of clinical trials;C: Intervention model of clinical trials;D: Status of clinical trials;E: Phase of clinical trials.N/A: Not available.
CURRENT RESEARCH ADVANCEMENTS IN THE USE OF UC-MSCS FOR PULMONARY DISEASES
UC-MSCs for COVID-19
COVID-19,caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2),has developed into a global pandemic and become the greatest public health threat in the 21stcentury[61].People infected with SARS-CoV-2 have a wide range of clinical manifestations,ranging from asymptomatic or mild to severe respiratory symptoms,such as ARDS or multiple system organ failure,and death[62].The host’s innate and adaptive immune responses associated with SARS-CoV-2 infection play a critical role in controlling virus replication[63].Cytokine storms and excessive inflammation are considered the major causes of ARDS and multiple-organ damage,and they play important roles in the process of disease aggravation,especially in patients with severe COVID-19[64].As of November 11,2022,more than 630 million people were infected with COVID-19,and the number of deaths exceeded 6.6 million[65].The serious sequelae of COVID-19 have a significant impact on health and quality of life[48].At present,different potential treatment options for COVID-19,such as Paxlovid,recombinant soluble angiotensin-converting enzyme 2,monoclonal antibodies,antiviral molecules,IFN therapy,corticosteroids,herbal medicines,and vaccines,have been explored[66].Considering the high impact that critical cases of COVID-19 still have on health and their complex pharmacological management,the search for new therapeutic approaches is urgent[67].Research shows that MSCs have strong immunomodulatory and anti-inflammatory properties and can resist ARDS and cytokine storms in patients with COVID-19[68,69].Since the outbreak of the pandemic,a series of clinical trials of MSC therapy have been conducted in an effort to resolve immune dysfunction caused by severe inflammation due to COVID-19.
To date,17 clinical trials of UC-MSC treatments for COVID-19 have been registered in the Clinical Trial Database(Table 1).Consequently,9 clinical trials were open-label;1 clinical trial was single-blinded for the participants;5 were triple-blinded for the participants,care providers,and investigators;and 2 were quadruple-blinded for the participants,care providers,investigators,and outcome assessors.Among all the eligible clinical trials,14 were randomized,1 was nonrandomized,and 2 did not provide relevant descriptions.The vast majority of clinical trials (n=12) were in phase I,phase II or combined phase I/II,accounting for 70.5% of the total.Remarkably,only a small portion of the patients were in phase III (n=2 or 11.8%).Therefore,most trials were in the early phases,and the results from these trials need to be further tested in advanced-phase trials.Among the 17 enrolled trials,2 were completed;1 was active but not recruiting;3 were still recruiting;2 were not yet recruiting;2 were withdrawn;and 7 had an unknown status.The clinical trials were conducted in 6 countries.China hosted the largest number of clinical trials (n=9),followed by the United States (n=3)and Indonesia (n=2).All 17 clinical trialsweredesigned specifically for adults or older adults.UCM-SCswere usually administered intravenously once ormultiple tmies,and thedoses ranged from 0.5× 106/kg to 1× 106/kgper injection.

Table 1 Clinical trials of umbilical cord mesenchymal stem cells therapy for patients with coronavirus disease 2019
Many registered clinical trials have reported these findings.Shiet al[62] conducted a randomized,double-blind,and placebo-controlledphase II trial in which 65 severeCOVID-19patientswith lungdamage receivedUCM-SC treamtent on days 0,3,and 6 and 35patients (control group) receivedplacebo N(CT04288102).That study showed that,comparedwith the placebo,UCM-SC administration significantly miproved the whole-lung lesion volume from baseline today 28.The distance traveled in the 6m-inwalk test (6M-WT)was increased in patients treatedwith UCM-SCs.These results suggested thatUCM-SC administration is a potentially safe and effective therapeutic treamtent forCOVID-19 patients with lung damage.To evaluate the effects of these interventions on reducing them ortality rate andpreventing long-term pulmonary disability,a phase III trial is necessary in the future.In Jakarta,Indonesia,a double-blind,multicenter,randomized controlled trial at four COVID-19 referral hospitals was conducted by Dilogoet al[36] (NCT04457609).Forty randomly allocated critically ill patients with COVID-19 were included in this study;20 patients were given a single intravenous infusion of 1 × 106cells/kg body weight (BW) UC-MSCs in 100 mL of saline solution,and 20 patients received a placebo (100 mL of saline solution) as a control group.UC-MSC treatment significantly improved the survival rate of critically ill patients with COVID-19 by modulating the immune system toward an anti-inflammatory state.The survival rate in the UC-MSC group was 2.5 times greater than that in the control group,and the survival rate of patients with comorbidities was 4.5 times greater than that of the controls.Moreover,the intravenous administration of UC-MSCs was safe and well tolerated and did not cause life-threatening complications or acute allergic reactions.A randomized,double-blind phase II study involving 17 patients with COVID-19 also yielded encouraging results[70].Compared to those in the placebo group,the levels of ferritin,IL-6,MCP1-CCL2,CRP,D-dimer,and neutrophil levels were lower,and the numbers of CD3+and CD4+T lymphocytes and NK cells were greater in the treatment group.These findings indicate that UC-MSC infusion plays an important role in the early prevention of severe complications and the reduction of sequelae in critically ill patients with COVID-19.Our research team also performed considerable work during the COVID-19 epidemic[71-74].One of our previous studies reported the case of a 54-year-old patient with severe COVID-19 who receivedWharton’s jelly (WJ)-MSCs[75].The pulmonary function and symptoms of the patient significantly improved 2 d after WJ-MSCs transplantation,and the patient recovered and was discharged 7 d after treatment.During the treatment period,the inflammatory indices and immune status of the COVID-19 patients significantly improved,which suggested that WJ-MSC transplantation may improve the prognosis of patients with COVID-19 by regulating the inflammatory response and promoting the recovery of antiviral immune cells and organs.
UC-MSCs for ARDS
ARDS,an acute respiratory condition in critically ill patients,is characterized by acute and refractory hypoxemia,noncardiogenic pulmonary edema,diffuse alveolar-capillary membrane damage,and reduced compliance (or increased lung stiffness)[5].Patients with severe pneumonia induced by SARS-CoV-2 rapidly develop ARDS and die of multiple-organ failure[76].The outbreak of COVID-19 has led to a significant increase in the number of ARDS patients worldwide.Despite advances in supportive therapies,ARDS still has very high mortality and long-term morbidity.In the United States,the incidence of ARDS ranges from 64.2 to 78.9 cases/100000 person-years[77].Despite decades of basic and clinical research,there is still no safe and effective pharmacotherapy for ARDS.Therefore,there is an urgent need for new therapeutic methods to minimize lung tissue damage caused by inflammation and reduce the mortality rate in patients with ARDS.An increasing number of early clinical trials have verified the therapeutic potential of UC-MSC therapy,and the results of phase I/II clinical studies have demonstrated its feasibility,preliminary safety and efficacy in patients suffering from ARDS[78-80].
To date,14 clinical trials assessing the safety and efficacy of UC-MSC therapy in ARDS patients have been registered(Table 2).These clinical trials were mainly conducted in the United States (n=5) and China (n=3) and accounted for 57%of the total.The main intervention models were single-group,parallel and sequential assignment.Among all the included clinical trials,3 clinical trials involved single-group assignment,8 involved parallel assignment,2 involved sequential assignment,and 1 did not provide relevant information.Eight clinical trials were randomized,2 were nonrandomized,and 4 did not report the allocation.Most trials (n=12) were in the early phases,with the exception of 2 trials that were not described.All the clinical trials included adults and elderly individuals.Six clinical trials were open-label.In terms of the blinding design,1 was double-blinded for the participants and care providers;4 were triple-blinded for the participants,care providers,and investigators;and 2 were quadruple-blinded for the participants,care providers,investigators,and outcome assessors.
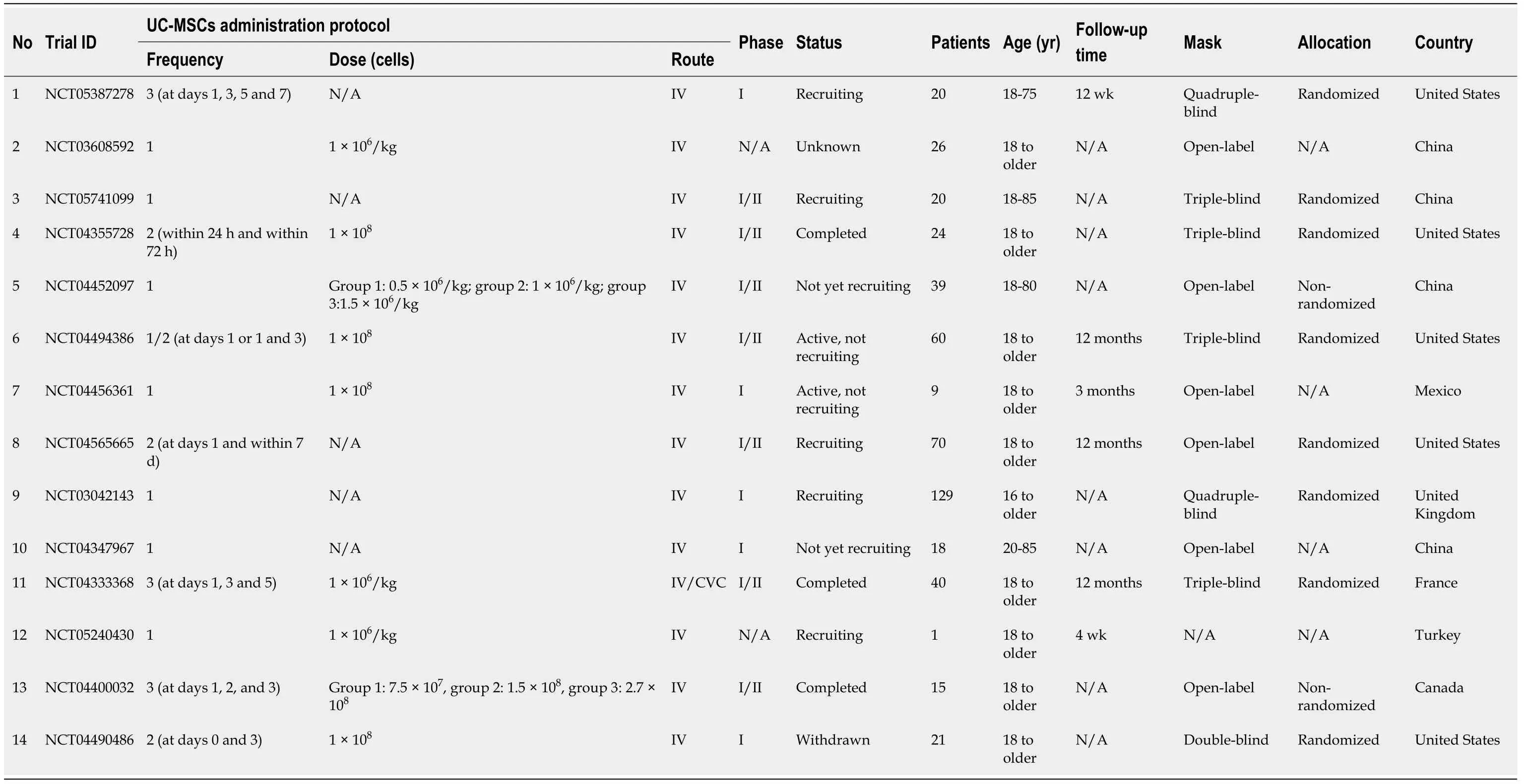
Table 2 Clinical trials of umbilical cordmesenchymal stem cells therapy for patients with acute respiratory distress syndrome
To evaluate the safety and explore the possibility of three injections of UC-MSCs in patients with mild-moderate ARDS induced by COVID-19,a single-center,open-label,phase I clinical trial with a placebo-control group was conducted at Imam Reza Hospital[81].Ten patients in the intervention group received three intravenous infusions of UC-MSCs (1 × 106cells/kg BW per injection) on days 1,3 and 5,and 10 patients in the placebo-control group were administered normal saline.The follow-up period in this clinical trial was 17 d.According to their results,the SPO2/FIO2ratio and serum CRP levels were significantly improved,and the serum inflammatory cytokines (IL-6,IFN-γ,TNF-α and IL-17A) were also significantly reduced after UC-MSC intravenous infusion,which demonstrated that multiple transplantations of UCMSCs can decrease cytokine storms and ameliorate respiratory functions.Monselet al[82] conducted a double-blind,multicenter trial for the treatment of SARS-CoV-2-induced ARDS (NCT04333368).Among these patients,21 patients were randomly assigned to receive 3 rounds of intravenous infusions of UC-MSCs (1 × 106/kg per infusion) over 5 d after recruitment,and 24 patients received saline (0.9%) solution as the control.There was no significant difference in the incidence of infusion-associated adverse events (AEs) between these two groups,and no serious AEs linked to UC-MSC infusion were observed.These findings suggest that intravenous administration of UC-MSCs is safe for patients with SARS-CoV-2-induced ARDS.A phase I/II randomized,double-blind,placebo-controlled trial of 24 patients was conducted in the UHealth System/Jackson Health System in Miami,Florida (NCT04355728)[21].In this study,12 ARDS patients received two intravenous infusions (at days 0 and 3) of UC-MSCs;controls received two infusions of vehicle solution.The results showed that the 31-d mortality rate was 9% in the UC-MSC treatment arm and 58% in the control arm.After UC-MSC treatment,lung inflammation in ARDS patients was alleviated,and this change was accompanied by a significant decrease in inflammatory factor levels.In addition,the UC-MSC-treated group exhibited a shorter recovery time than the control group.Severe UC-MSC infusion-related AEs were not observed in either group.Therefore,UC-MSC infusion may be a safe and effective treatment option for ARDS patients.To explore the maximum tolerable dose of infused UC-MSCs,Yipet al[83] administered different doses of UC-MSCs (1.0 × 106cells/kg,5.0 × 106cells/kg,1.0 × 107cells/kg) intravenously to 9 patients with moderate to severe ARDS.Their results demonstrated that a single intravenousUCM-SC infusion of up to 1.0 × 107cells/kgwas excellently tolerated inARDS patientswithout seriousAEs.Interestingly,several inflammatory indicators (i.e.,CD11b+/CD16+,CD11b+/MPO+,CD16+/MPO+,andCD14+CD33+)substantiallydecreased on the firstday after cell infusion,followed by a significant gradual increase from day 3 today 7,and then a significant decrease compared to baseline treamtent on the 30thd after cell infusion.Therefore,the anti-inflammatory effect of single-dose UC-MSC reinfusion in the human body may have a certain timeliness.
UC-MSCs for BPD
BPD is a chronic lung disease in premature infants that is characterized by the arrest of alveolarization,fibroblast activation,and inflammation.Many risk factors can increase a baby’s risk of developing BPD,including premature birth,oxygen poisoning,intrauterine growth delay,smoking,ventilation support,infection,inflammation,patent ductus arteriosus,congenital factors,and immature lung development[84-88].The pathogenesis of BPD involves a variety of pathophysiological factors,including abnormal angiogenesis,inflammation,oxidative stress,and impaired lung repair[89].Epidemiological studies have shown that the incidence of BPD in very preterm infants increases with decreasing gestational age and birth weight and reaches as high as 40%[90,91].BPD can affect the nervous,circulatory and respiratory systems and has a serious impact on the survival rate and quality of life of premature infants[92].Despite major advances in understanding disease pathologies,there is no single treatment or combination therapy available for preventing or treating BPD.As a more promising novel therapeutic option,MSCs have been widely used in clinical practice due to their anti-inflammatory and paracrine effects.MSCs can also contribute to the repair of lung injuries by restoring the integrity of lung epithelial/endothelial cells,which provides a new approach for the application of MSCs in BPD[93,94].
There were 18 registered clinical trials using UC-MSCs for the treatment of BPD (Table 3).These clinical trials were mainly conducted in five countries,namely,China,South Korea,Vietnam,Canada and the United States.In terms of grouping design,6 clinical trials used single-group assignment,10 used parallel assignment,and 2 did not describe the grouping design.Only 10 trials,including randomized (n=7) and nonrandomized (n=3) studies,provided necessary descriptions of random allocation.There were 10 phase I clinical trials,4 phase II trials,and 3 phase I/II trials,accounting for 56%,22%,and 17%,respectively.Twelve clinical trials were open-label;1 was double-blinded for the participants and care providers;3 were triple-blinded for the participants,care providers,and investigators;and 3 were quadrupleblinded for the participants,care providers,investigators,and outcome assessors.

Table 3 Clinical trials of umbilical cordmesenchymal stem cells therapy for patients with bronchopuml onary dysplasia
Moreiraet al[95] studied the feasibility and effectiveness of nasal administration of UC-MSCs in the treatment of hyperoxia-induced BPD in a rat model.Lung alveolarization,vascularization,and pulmonary vascular remodeling were restored in BPD rats receiving UC-MSC treatment.The results of the gene and protein analyses indicated that the beneficial effects of UC-MSCs were partially attributed to collaborative efforts targeting angiogenesis,immune regulation,cell survival,and wound healing.Gene and protein analyses suggest that the beneficial effects of UC-MSCs are due in part to concerted efforts targeting immune regulation,angiogenesis,cell survival,and wound healing.Therefore,nasal administration of UC-MSCs for BPD treatment is a noninvasive,feasible route of administration with potential for widespread clinical application.Many registered clinical trials have also published their research findings.A study conducted by Changet al[96] included 9 patients with preterm infants at high risk for BPD (NCT01297205).The first three patients received a low dose of UC-MSCs intratracheally administered at a concentration of 1 × 107cells/kg BW,while the subsequent six patients received a high dose of UC-MSCs intratracheally administered at a concentration of 2 × 107cells/kg BW.No AEs related to infusion were observed.The levels of IL-6,IL-8,MMP-9,TNF-α,and transforming growth factor-β1 in tracheal aspirate fluid were significantly decreased after UC-MSC transplantation.Among the 9 infants who received UC-MSC transplantation,only 3 developed moderate BPD,which showed that UC-MSCs could significantly lower BPD severity.The intratracheal transplantation of UC-MSCs was found to be safe and feasible for preterm infants.In a phase I dose-escalation trial involving 2 dosing regimens,Powell and Silvestri[97] investigated the safety and efficacy of intratracheal administration of UC-MSCs (NCT02381366).In this trial,12 preterm infants at the highest risk for BPD were randomized into two groups.In this study,12 premature infants with BPD received two doses of UC-MSCs (low dose,1 × 106cells/kg;high dose,2 × 107cells/kg)viaendotracheal administration.All patients completed the 84-d followup.The 12 patients tolerated the treatment well,with no reports of dose-limiting toxicity within the first 72 h.Additionally,no serious AEs related to the drug were observed during the 84 d in this study.Based on the above studies,UC-MSCs may be a safe and effective treatment method for BPD.
UC-MSCs for COPD
COPD is a chronic inflammatory lung disease caused by airway and alveolar abnormalities,and irreversible airway limitation is a common feature[98].According to the World Health Organization,COPD will become the third leading cause of death by 2030 and represents a considerable burden on the health-care system[99].At present,the pathogenesis of COPD is mainly the result of interactions between genetic factors and acquired factors,but the exact pathological mechanism is still unclear[100].Some studies have suggested that smoking is the main environmental factor triggering COPD,but other factors also include airway hyperresponsiveness,sex,genetics,occupation,lung growth,and development[101,102].Currently available treatment methods for COPD,which mainly focus on treating the symptoms and slowing the progression of these disorders,include anti-inflammatory drugs,corticosteroids,long-acting muscarinic antagonists,and β2-adrenergic receptor agonists[103,104].These treatments may help minimize airflow limitation and future exacerbations but cannot reverse lung damage or improve quality of life in patients with COPD.Recent advances in cell therapy have demonstrated that MSCs are safe and effective at improving quality of life and clinical conditions and are potential candidates for clinical use in the treatment of COPD[105].
Currently,the use of a total of 3 UC-MSC transplantations is being verified in clinical trials for the treatment of COPD(Table 4).These clinical trials are being conducted in China,Vietnam,Antigua,and Barbuda,all of which are in early phases.Ríoet al[106] conducted a preclinical study using UC-MSC cellular therapy for COPD.They tested the therapeutic effects of different routes of administration (intravenously and intratracheally) on COPD mice and analyzed the relevant molecular changes through protein array analysis.The results showed that UC-MSCs can effectively reduce lung emphysema regardless of the administration route and modify the inflammatory profile in elastase-treated mice,which is most likely due to mitochondrial transfer, immunomodulation, and homing to the injured areas. In the clinical study conducted by Le Thi Bich et al[19], 20 patients with COPD (9 at stage C and 11 at stage D according to the Global Initiative for Obstructive Lung Disease classification) were infused with 1 × 106 cells/kg of expanded allogeneic UC-MSCs. After 6 months of follow-up, the COPD incidence, Modified Medical Research Council score, and number of exacerbations were significantly lower in patients who underwent UC-MSC transplantation than in those who did not. No UC-MSC infusionrelated toxicity or death occurred during the administration process. However, there were no significant decreases in the forced expiratory volume in 1 s, CRP, or 6-MWT values after treatment (at 1, 3, and 6 months, respectively) compared to the corresponding values before treatment. In summary, in vitro and in vivo research results suggest that UC-MSCs may be a safe and effective treatment method for moderate-to-severe COPD and are worthy of further clinical promotion

Table 4 Clinical trials of umbilical cord mesenchymal stem cells therapy for patients with chronic obstructive pumlonary disease
UCM-SCs forPF
PF is a chronic progressive lung disease that eventually leads to death and respiratory failure and is characterized by inflammation and fibrosis of the interstitium and destruction of the alveolar histoarchitecture[48,107]. There are various risk factors that initiate lung tissue damage and PF, including smoking, virus or bacterial infections, autoimmune reactions, air irritants, chemotherapy, ionizing radiation, and pollutants[108-110]. IPF, regarded as the most common type of pulmonary fibrosis, is a progressive disease of the lower respiratory tract with an incidence of 4.6 to 16.3 cases per 100000 worldwide[111]. Despite decades of scientific research, the factors involved in the onset of the histopathological cascade in PF have not been identified. Currently, there are no effective therapeutic approaches for preventing pulmonary fibrosis development. Emerging MSC-based therapy has been shown to be a new and promising therapeutic strategy due to its anti-inflammatory and antifibrotic effects, and accumulating evidence indicates that MSC transplantation potentially alleviates and ameliorates PF[112-114]. Many studies have revealed the beneficial treatment effects of MSC administration in patients with PF[115,116].
According to the ClinicalTrials.gov website, a total of 3 clinical trials focused on UC-MSC-based therapy for PF were registered (Table 5). All 3 clinical trials were phase I. Two trials are currently being recruiting, and 1 has been completed.UC-MSCs are usually administered intravenously once, and the doses range from 1 × 106 cells/kg to 1 × 108 cells/kg per injection. Currently, there are no published results corresponding to registered clinical trials. da Silva et al[117] reported a case in which a 30-year-old patient with COVID-19 progressed to PF and received UC-MSCs (5 × 107, 2 doses 2 d apart).After UC-MSC treatment, improvements in the patient’s chest computed tomography scan were observed, with a decrease in ground-glass opacity and pneumonia infiltration, as well as an increase in the PaO2/FiO2 ratio and a reduction in the need for vasoactive drugs. Simultaneously, modulation of different cell populations in the PB was also observed, as indicated by a reduction in inflammatory monocytes and an increase in the frequency of patrolling monocytes, type 2 classical dendritic cells, and CD4+ lymphocytes. These findings suggested that UC-MSC therapy may be a potential treatment option for critically ill patients with fibrosis caused by COVID-19. Unfortunately, considering the limited number of published results, the effectiveness and safety of UC-MSCs for treating PF still require additional highquality multicenter clinical trials for further confirmation.

Table 5 Clinical trials of umbilical cordmesenchymal stem cells therapy for patients with puml onary fibrosis
CONCLUSOIN
With the increasing use of UC-MSC therapy for clinical treatment, UC-MSC-based therapy approaches are continuing toevolve at a rapid pace, especially for treating currently incurable and devastating lung diseases. However, manyproblems remain to be solved, such as the number of cells, transplantation routes, and mechanism of action. To date,however, a comprehensive systematic analysis of clinical trials from the Public Clinical Trial Database has not beenpublished. In this study, 55 clinical trials of pulmonary diseases worldwide were systematically analyzed. These clinicaltrials were widely distributed and conducted in 13 countries. Currently, these clinical trials have several limitations. Forexample, 63.6% of clinical trials are in the early phases, during which safety has largely been demonstrated. The relativelysmall number of recruited subjects has also been a prominent limitation in these clinical trials. There are certaindisparities caused by the different groups of recruited participants, therapeutic regimens and doses and frequencies ofUC-MSCs in previous clinical trials. In addition, among the 55 clinical trials included in this study, 11 trials werecompleted. To date, available data from published clinical studies have proven the safety and efficacy of UC-MSCtherapy for various lung diseases, with few infusion-related reactions and late adverse effects. In particular, the greatmajority of clinical trials were recruiting or active but not recruiting. Therefore, the current positive conclusions about theprevention or treatment of lung diseases by UC-MSCs need to be further validated and evaluated
Although great progress has been made in preclinical and clinical studies of UC-MSC therapy,there are still substantial challenges in the clinical setting.According to the summary analysis of registered clinical trials,factors such as donor selection,culture conditions,cell consistency,dosage of UC-MSCinfusion,long-term therapeutic effects,and potential tumorigenicity remain the bottlenecks in clinical treatment mediated by UC-MSCs.Standardization of the evaluation of UC-MSCs was lacking,which was an important problem for cell viability and homing.The use of UC-MSCs in clinical practice requires a large number of cells;however,long-termin vitroculture and continuous passages of UC-MSCs may exert important influences on phenotypic characterization and biological function.Thus,UC-MSCs require a standard treatment protocol,such as donor sources,cell usage and dosage,manufacturing protocols,quality control,and delivery routes.Before clinical application,a series of tests,including bacteriological tests,viability and phenotype tests,oncogenicity tests,and endotoxin assays,should be carefully performed to ensure cell quality control.These challenging questions regarding UC-MSC therapy need to be addressed,as they could contribute to the translation of cell therapy from bench to bedside for patients suffering from lung diseases.To determine the long-term efficacy of UC-MSC therapy for lung disease,prospective,multicenter,randomized,controlled and long-term follow-up clinical trials with large sample sizes are still necessary.
FOOTNOTES
Co-first authors:Min Meng and Wei-Wei Zhang.
Co-corresponding authors:Chang-Hui Zhou and Da-Rui Wang.
Author contributions:Meng M and Zhang WW contributed equally to this work.Meng M and Zhang WW collected the references,analyzed clinical trials,and drafted the manuscript;Zhou CH andChen SF contributed to the conception and design of the review;Zhou CH andWang DR critically and systemically revised the manuscript;and all authors read and approved the final manuscript.Zhou CH andWang DR contributed efforts of equal substance in the research process.The choice of these researchers as co-corresponding authors acknowledges and respects this equal contribution.In summary,we believe that designating Zhou CH andWang DR as cocorresponding authors of is fitting for our manuscript as it accurately reflects our team’s equal contributions,collaborative spirit,and diversity.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Min Meng 0000-0002-3055-7948;Wei-Wei Zhang 0009-0004-5893-4065;Shuang-Feng Chen 0009-0008-8205-9378;Chang-Hui
Zhou 0000-0002-9573-7966.
S-Editor:Wang JJ
L-Editor:Webster JR
P-Editor:Yuan YY
杂志排行

World Journal of Stem Cells的其它文章
- Multiple pretreatments can effectively improve the functionality of mesenchymal stem cells
- Cellular preconditioning and mesenchymal stem cell ferroptosis
- Unlocking the versatile potential: Adipose-derived mesenchymal stem cells in ocular surface reconstruction and oculoplastics
- Crosstalk between Wnt and bone morphogenetic protein signaling during osteogenic differentiation
- Human pluripotent stem cell-derived kidney organoids: Current progress and challenges
- Recent progress in hair follicle stem cell markers and their regulatory roles