Paradoxical systemic toxicity by inhaled paraquat poisoning:A case report
2024-03-05TulikaGargJaspreetKaurYuvrajSinghCheema
Tulika Garg,Jaspreet Kaur,Yuvraj Singh Cheema
Department of General Medicine,Government Medical College and Hospital,Chandigarh,India
ABSTRACT Rationale:Multi-organ failure is a symptom of paraquat poisoning,resulting in high mortality and morbidity rates.Though paraquat is widely available,poisoning through inhalation is rare.Patient’s Concern:A 37-year-old male reported to the emergency department with complaints of vomiting after an alleged history of inhalation of paraquat while at work.Diagnosis:Paraquat poisoning.Interventions:Supportive management along with multiple sessions of hemodialysis.Outcomes:Renal complications caused by paraquat were improved after multiple sessions of hemodialysis.However,the patient developed respiratory complications and later due to persistent hypoxemia and non-responsive to supportive therapy,he succumbed to his illness.Lessons:Acute kidney injury is a complication of paraquat poisoning.However,kidney involvement with the inhalational mode is rare.It is caused by reduction and oxidation cycles,as well as the formation of reactive oxygen species,necessitating hemodialysis as the treatment.Without a clear history,a specific clinical trait,or a diagnostic test,diagnosis can be difficult.Our case thus highlights the inhaled paraquat poisoning,presenting with acute kidney injury with late respiratory impairment as a consequence.
KEYWORDS: Paraquat poisoning;Pesticide;Acute kidney injury;Respiratory insufficiency;Hemodialysis
1.Introduction
Paraquat is a frequently used herbicide among farmers.It is a fastacting,nonselective,quaternary nitrogen herbicide that is sprayed on weeds and other vegetation before planting crops which helps to destroy plants by translocation.This leads to the formation of singlet oxygen,superoxide anion,and hydroxyl radicals.Paraquat can achieve rapid weeding because it prevents the photosynthesis-related conversion of oxidized coenzyme II (NADP) into reduced coenzyme II (NADPH) in plant cells,resulting in the accumulation of reactive oxygen species and cell death[1].Acute paraquat intoxication has no known antidote,and the fatality rate is significantly high[2].Although multiple organ failure and acute lung injury are common clinical characteristics of paraquat intoxication,acute kidney injury (AKI) can also happen after acute large-dose exposure to this hazardous pesticide[3].We report an unusual case presenting with AKI,with only mild pulmonary involvement in the case of inhalational paraquat poisoning.
2.Case report
A proper informed consent was obtained from the patient.A 37-year-old male,after being admitted to one other healthcare center for 5 days with complaints of vomiting for an alleged history of inhalation of paraquat while he was working in the fields,was referred to our emergency department.The patient showed the photograph of paraquat herbicide which he was spraying in the fields.The total duration for which he was exposed to the herbicide was around 2 hours.The vomitus consisted of ingested food particles,non-blood stained,non-bilous,and non-projectile.No associated pain in the abdomen,loose stools,fever,shortness of breath,or decreased urine output was present.Family and past medical history were not significant.The gastric lavage was not done due to his late presentation to our hospital.
The patient was conscious and oriented to time,place,and person.His Glasgow coma scale was 15/15.The vitals were stable with a blood pressure of 128/84 mmHg (normal:<120/80 mmHg),respiratory rate of 24/min (normal:12-18/min),heart rate of 86/min (normal:60-100/min),and room air saturation of 95% by finger pulse oximeter (normal:95%-100%).Systemic examination was unremarkable.
The complete blood investigations of the patient are summarized in Supplementary Table 1.The high-resolution computed tomography chest done at the other healthcare center was normal (Figure 1A).The chest X-ray done at our hospital was normal.Electrocardiogram was suggestive of normal sinus rhythm.In view of deranged renal function tests and anuria,the patient was hemodialysed.He underwent six cycles of hemodialysis during his hospital stay.Otolaryngologist examination revealed oral ulcers with whitish slough.The neck X-ray showed no subcutaneous emphysema (Supplementary Figure 1).After 14 days of admission to our hospital,the patient started complaining of shortness of breath.His pulse oximetry readings were 85%-90% recorded under room air (normal:95%-100%).Arterial blood gas analysis was suggestive of hypoxemia (pH:7.34,pCO2:34,pO2:65,HCO3:15.1) (normal:pH:7.35-7.45,pCO2:35-45,pO2:75-100,HCO3:22-28).Repeat high-resolution computed tomography chest revealed ground glass opacities with inter/intralobular septal thickening consistent with acute lung injury with no evidence of pneumomediastinum (Figure 1B).
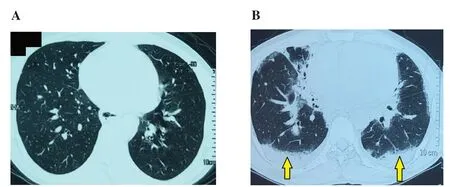
Figure 1.High-resolution computed tomography (HRCT) chest of a 37-year-old male patient.(A) Normal HRCT done at the time of admission and (B) HRCT done after two weeks of the admission showing ground glass opacities and inter/intralobular septal thickening (arrows) in the bilateral lung fields suggestive of acute lung injury.
The patient was managed conservatively for his symptoms with oxygen supplementation and steroids.In view of his respiratory distress and persistent hypoxemia the patient was intubated and was put on mechanical ventilation.However,he succumbed to his illness.
3.Discussion
The renal elimination of paraquat is biphasic,with an early,rapid elimination phase and a late,slow elimination phase,due to the development of renal tubular damage.The kidneys are the key target organs after being poisoned,according to the toxicokinetic process of paraquat.Within 12 to 24 hours,90% of paraquat is eliminated in its natural form from the kidneys[4].Our case of renal failure which occurred without respiratory insufficiency in the early phase,was resolved following six cycles of hemodialysis.
AKI lowers paraquat clearance even more,increases paraquat buildup in lung tissue,and promotes pulmonary interstitial fibrosis.As a result,early detection and treatment of AKI are critical for lowering the fatality rate of acute paraquat poisoning.The mechanism behind AKI is unknown;however,it is known to accumulate within renal tubular cells leading to the generation of reactive oxygen species and eventually damaging the proximal tubules[5].Inflammatory response,apoptosis,oxidative stress,and renal hemodynamic alterations are all involved in paraquat-induced acute kidney damage[6].Paraquat-induced AKI precedes acute lung injury,peaks within 3 to 5 days,and subsequently returns to normal renal function in some individuals within 3 weeks[7].Acute tubular necrosis and ischemic glomerulopathy are the most common pathological symptoms of acute paraquat poisoning.Simple urine abnormalities,such as proteinuria and/or haematuria,may appear in mild instances.Severe cases,on the other hand,may result in acute renal failure and necessitate renal replacement treatment.Dehydration probably exacerbates this condition,underlining the urgent need for fluid replacement.
Apart from the renal involvement,other manifestations of paraquat poisoning include pulmonary hypertension,fibrosis,pneumonitis,metabolic edema,central nervous system involvement,hepatitis,and cardiogenic shock[8].Impaired respiratory function usually occurs in the early stages of paraquat poisoning but in our case,it was a late finding.It is well known that paraquat concentrates in the lungs (pulmonary concentrations can be 10 times higher than plasma).Postmortem examinations in paraquat poisoning patients have revealed alveolitis,bronchiolitis,fibrosis,and edematous brain with marked congestion in the organs[9].Oxygen supplementation,which is usually deferred until PO2is less than 70 mmHg,can aggravate lung injury.Thus,in paraquat poisoning,there are two phases:(1) destructive,with inflammation and edema,and (2) proliferative,with fibroblast proliferation leading to interstitial fibrosis.Paraquat poisoning is associated with high mortality rates but the use of vitamins C,and E silymarin,immunosuppressants like cyclophosphamide,methylprednisolone along with detoxification with hemodialysis and hemoperfusion has shown promising results[10].
Paraquat toxicity has no specific antidote,thus supportive therapy is the mainstay.Acute renal injury is a common side effect that should be recognized and treated as soon as possible.Immediate and appropriate therapies,as well as hemodialysis,play an evident and critical role in the survival of patients who have consumed paraquat.
Conflict of interest statement
The authors report no conflict of interest.
Funding
This study received no extramural funding.
Data availability statement
The data supporting the findings of this study are available from the corresponding authors upon request.
Authors’ contributions
TG and JK:case presentation,data collection,investigations,and writing of original draft.YSC:literature review,writing of original draft including the conclusion,references,and formatting.
杂志排行

Journal of Acute Disease的其它文章
- Inflammation:Complexity and significance of cellular and molecular responses
- Drone systems for delivering defibrillators for sudden cardiac arrests
- Anesthetic consideration in Meigs syndrome with large pleural effusion and lung collapse
- Acute coalescent mastoiditis in a 16-month-old child due to Streptococcus pneumoniae infection
- Clinical profile and risk factors of symptomatic and asymptomatic hypoglycemia in neonates admitted to NICU in a tertiary care center:A cross-sectional study
- Relationship between nutritional therapy and beneficial bacteria ratio in severe disease