Measurement properties of assessment tools of Kinesophobia in patients with cardiovascular disease: A systematic review
2024-02-27YingyingJiaNianqiCuiTingtingJiaHammzaJabbarAblSattarHamouiJianpingSong
Yingying Jia ,Nianqi Cui ,Tingting Jia ,Hammza Jabbar Abl Sattar Hamoui ,Jianping Song
a Nursing Department,The Second Affi liated Hospital of Zhejiang University School of Medicine,Hangzhou,China
b Nursing Department,Zhejiang University School of Medicine,Hangzhou,China
c School of Nursing,Kunming Medical University,Kunming,China
d General Surgery Cadre Ward,Gansu Provincial People’s Hospital,Lanzhou,China
e Faculty of Clinical Medicine,Zhejiang University School of Medicine,Hangzhou,China
Keywords:
ABSTRACT Objectives: This study aimed to evaluate the measurement properties and methodological quality of assessment tools for Kinesophobia among patients with cardiovascular disease and provide a reference for healthcare professionals in selecting high-quality assessment tools.Methods:A systematic search was performed on specific databases: Embase,the Cochrane Library,PubMed,Web of Science,China National Knowledge Infrastructure,Wanfang database,China Biological Medicine disc,CINAHL,and China Science and Technology Journal Database,from inception to April 1,2023.The researchers retrieved studies on the measurement attributes of the exercise fear scale in patients with cardiovascular diseases.They also traced back the references of the included studies to supplement relevant literature.According to the inclusion and exclusion criteria,screening and data extraction were independently undertaken by two reviewers.Two researchers individually used the Consensus-based Standards for the selection of health Measurement Instruments (COSMIN) Risk of Bias Checklist to assess the methodological quality of the scale,applied the COSMIN criteria to evaluate the measurement properties of the scale,and used a modified Grading,Recommendations,Assessment,Development,and Evaluation system to assess the certainty of evidence.Results:Seventeen studies were identified that reported the psychometric properties of six patient reported outcome measurement tools (included different language versions).The methodological quality of content validity was adequate in only two studies,the remaining patient-reported outcome measures demonstrated doubtful content validity.Limited information on cross-cultural validity/measurement invariance,measurement error,and responsiveness was retrieved.The Swedish version and the Chinese version of the Tampa Scale for Kinesiophobia Heart were graded “A.” The remaining instruments were graded “B.”Conclusions: The methodological and measurement attributes of the Swedish and Chinese versions of the Tampa Scale for Kinesiophobia Heart are relatively high quality and can be tentatively recommended.The measurement properties of the remaining scales remain to be verified.
What is known?
· Fear of exercise is a common phenomenon in patients with cardiovascular disease.
· Exercise is central to cardiac rehabilitation,and lack of exercise may lead to demoralization in patients,decreased quality of life,and increased risk of cardiovascular adverse events.
· There is limited evidence on the measurement properties of fear of movement scales,and more research is needed to evaluate their effectiveness rigorously.
What is new?
· Six scales have been identified for assessing Kinesiophobia in individuals diagnosed with cardiovascular disease.
· The methodological and measurement quality of the Swedish and Chinese versions of the Tampa Scale for Kinesiophobia Heart is relatively high,supporting their temporary recommendation for use.
1.Introduction
Cardiovascular disease (CVD) is the leading cause of death among patients and is characterized by high morbidity and mortality rates [1,2].From 1990 to 2019,the prevalence of CVD increased from 271 million to 523 million cases,and the number of CVD deaths rose from 12.1 million to 18.6 million [3,4].This trend significantly burdens patients,their families,and communities[3].Exercise-based cardiac rehabilitation,a crucial component in maintaining and enhancing cardiovascular health,can improve maximal oxygen uptake and endurance,consistently reduce the risk of cardiovascular adverse events,and alleviate symptoms of depression and anxiety[5].However,adherence to physical activity is generally low among patients with CVD [6-9].Most of their motor activity falls short of guideline standards[10,11].Insufficient exercise increases the risk of readmission,adverse cardiovascular events,and death [12].
Kinesiophobia,an irrational fear of movement due to concerns of pain,injury,or reinjury,was first addressed in 1993 when Waddell,G.et al.[13-15] developed the initial motor fear assessment scale.Since then,“fear of exercise”has increasingly gained the attention of healthcare professionals.It is common among patients with CVD[16-18],with studies indicating that over 70%of people with CVD exhibit high levels of exercise phobia[19,20].Risk factors for kinesiophobia in patients with CVD are not fully understood.However,researchers[17,21,22]suggest potential links to biological factors such as age,fatigue,and disease severity,as well as psychosocial factors including education level,depressive symptoms,cardiac anxiety,social support experience,fear of pain,and subjective social status.
Fear of exercise diminishes patients’ adherence to exercise,consequently impairing cardiac function and heightening the risk of cardiovascular events and death.It has been recognized as a substantial barrier to participation in and adherence to activity programs in patients with CVD [16].However,its prevalence may be underappreciated and underreported owing to the absence of a recognized tool for assessing fear of exercise and its severity.Given the extensive number of patients with CVD and the detrimental effect of fear of exercise on their physical function,it is imperative to accurately screen for the degree and causes of anxiety of exercise in patients with CVD and to provide tailored interventions.
Accurate,reproducible,and reliable evaluation instruments are crucial for dependable results [23-26].Currently,there are multiple scales available for assessing fear of exercise in patients with CVD.However,the quality of these scales needs to be evaluated,which makes it inconvenient for clinical workers to select and apply the scale.
The Consensus-based Standards for Selecting Health Measurement Instruments (COSMIN) guidelines,formulated and updated by psychometricians from multiple countries,aim to evaluate the efficacy of patient-reported outcome measures (PROMs) and the quality of research studies [27].This will guide researchers and health professionals in selecting appropriate scales.According to the COSMIN guideline standards,this study systematically evaluated assessment tools for fear of movement in patients with CVD.The objective was to identify high-quality assessment tools that can serve as a reference for future evaluations and empirical research on fear of movement in patients with CVD.
2.Methods
The systematic evaluation has been registered in PROSPERO under registration number CRD42022380281.
2.1.Literature search strategy
The PROMs of interest in this study were assessment tools for Kinesophobia in patients with CVD.The measured construct was exercise fear,with the target population being patients with CVD and high-risk individuals for CVD,and all measurement properties would be evaluated.The research team conducted a thorough literature search across several databases,including Embase,the Cochrane Library,PubMed,Web of Science,China National Knowledge Infrastructure,Wanfang database,CINAHL,China Biological Medicine disc(CBMdisc),and China Science and Technology Journal Database.This search aimed to identify studies evaluating the measurement properties of fear of exercise scales in patients with CVD.Searches were performed from the inception of each database until April 1,2023.A combination of MeSH terms and free-text words was employed in the literature search.To ensure comprehensiveness,the methodology followed the COSMIN search strategy recommendations,incorporating a mix of “interest structure,” “target group,” “tool type,” and “measured characteristics.”The following search terms were used: “fear,” “fear of activity,”“fear of movement,” “fear of physical activity,” “fear of exercise,”“movement phobia,” “coronary heart disease,” “coronary artery disease,” “cardiovascular diseases,” “myocardial infarction,” “cardiac rehabilitation,” “cardiovascular rehabilitation*,” “angina pectoris,” “atrial fibrillation,” “heart transplantation,” “structural validity,” “content validity,” “measurement error,” “criterion validity,” “responsiveness,” “patient-reported outcome measure*,”“surveys and questionnaires,” “PROMs,” “measure*,” and other related terms.See Appendix A for the remaining search strategy.To further enhance the breadth of the literature search,references were manually reviewed and included.
2.2.Literature inclusion and exclusion criteria
The inclusion criteria for the literature encompassed original studies focused on developing instruments to measure fear of exercise in patients with CVD or those at high risk.Additionally,studies must describe one or more psychometric properties in validating the developed tool for measuring fear of movement.The search strategy did not impose any language restrictions.
Literature exclusion criteria were as follows: studies were excluded if the full text was unavailable,if they were duplicate or overlapping publications,or if they were reviews,integrative evidence studies,conference abstracts,editorials,research protocols,or cross-sectional studies conducted during the early stages of scale development.Instruments employed solely as outcome measurement tools were also excluded from the review.
2.3.Study selection and data extraction
The research team,composed of individuals with substantial experience in cardiovascular nursing and evidence-based medicine,conducted a meticulous literature screening and data extraction.Two researchers (Y.Jia and N.Cui) independently reviewed the literature,extracted data,and performed crosschecks.Any disagreements during this process were resolved through consultation with a third researcher (T.Jia).In instances where the data obtained was incomplete,the creators of the instruments were contacted for additional pertinent information.
The initial phase of literature screening involved reviewing titles and abstracts to exclude irrelevant studies.Following this,two researchers (Y.Jia and N.Cui) conducted a full-text review to determine the final inclusion of studies.
Data extraction was carried out according to a standardized template,which included the following details:first author,sample size,year of publication,geographic region of study,age of participants,number of scale dimensions and items,description of scale dimensions,scoring method for each item,time required to complete the scale,and the measurement properties of the scale.These properties encompass content validity,structural validity,internal consistency,hypothesis testing,criterion validity,reliability,crosscultural validity,measurement error,and responsiveness.All psychometric property indicators were defined and measured by the established guidelines set by prior work[27-29].
2.4.Quality evaluation methods
2.4.1.Methodological quality assessment
The COSMIN risk of bias inventory,a comprehensive tool,is employed to assess the methodological quality of scale studies.It comprises ten modules: development of PROMs-crucial for evaluating content validity though not a measurement characteristic-content validity,structural validity,internal consistency,hypothesis testing,criterion validity,reliability,cross-cultural validity,measurement error,and responsiveness.To determine the risk of bias in each study,the inventory utilizes a five-point scale:“very good,” “adequate,” “doubtful,” “inadequate” and “not applicable.”The overall risk of bias score for each module is based on the lowest score of all items within that module,following the minimum scoring principle [27,30].
2.4.2.Evaluating the quality of psychometric properties
The COSMIN quality criteria developed by Terwee et al.[29]are primarily used for evaluating nine measurement characteristics of a scale: content validity,structural validity,internal consistency,hypothesis testing,criterion validity,reliability,cross-cultural validity,measurement error,and responsiveness.Each characteristic is assessed and assigned a rating: sufficient (+),insufficient (-),or uncertain (?).In cases where different studies provide varying evaluations of a specific psychometric property of a scale and the reasons for this inconsistency remain unclear,the overall rating for that psychometric property is classified as “inconsistent.” If highquality evidence suggests poor content validity of PROMs,further evaluation of the scale’s measurement properties may be bypassed,allowing for a direct recommendation for or against the use of the scale.
2.4.3.Assessing the quality of evidence and recommendations for evidence
Under the COSMIN framework,each measurement characteristic of a scale is initially considered “high quality.” This quality is then downgraded based on four factors:risk of bias,inconsistency,indirectness,and imprecision.The quality of evidence is categorized into four levels: “high,” “medium,” “low,” and “very low.”Subsequently,the research team thoroughly assesses the interpretability and applicability of the included scales,providing recommendations for their selection and usage.
For a scale to be recommended for use (with a strength of recommendation at Level A),its content validity must be at least“adequate”(regardless of the level of evidence),and the evidence of its internal consistency should not be rated lower than “low.”Conversely,if there is “high quality” evidence indicating “inadequate” content validity,the scale is advised against use (with a strength of recommendation at Level C).Scales with a strength of recommendation other than A or C are deemed to have potential for use;however,further research is required to assess their measurement properties more comprehensively (strength of recommendation: Level B) [27].
3.Results
3.1.Search process
A preliminary search yielded 1,642 articles.After removing duplicates,1,390 articles were excluded.Subsequent evaluation of titles and abstracts led to the exclusion of 1,350 articles.A full-text review resulted in the discard of 23 articles.In the end,17 articles were selected for analysis (Fig.1).

Fig.1. The literature screening process.
3.2.Characteristics of the included studies
Six instruments,specifically developed or translated for assessing fear of exercise in patients with CVD,were identified [14,15,23-26,31-41].Table 1 presents the basic characteristics of these studies,published between 1993 and 2023,with study sites in countries including the United Kingdom,Poland,Sweden,Turkey,and China.Three PROMs (The Tampa Scale for Kinesiophobia Heart [TSK Heart],Exercise Sensitivity Questionnaire [ESQ],Fear of Activity in Patients with Coronary Artery Disease [FACT-CAD]) were available in multiple languages [14,23,24,26,32-41].Lei et al.[34] and Tang [36] independently translated the TSK Heart into Chinese version (TSK-CV Heart) and conducted tests of its validity and reliability.Hu [37],Chen et al.[39],and Gao et al [40].independently translated the FACT-CAD scale into Chinese version (FACT-CV CAD) and conducted tests of its validity and reliability.Keessen et al.[24] and Ter Hoeve et al.[38] independently translated the TSK Heart into Dutch version (TSK-DV Heart) and conducted tests of its validity and reliability.
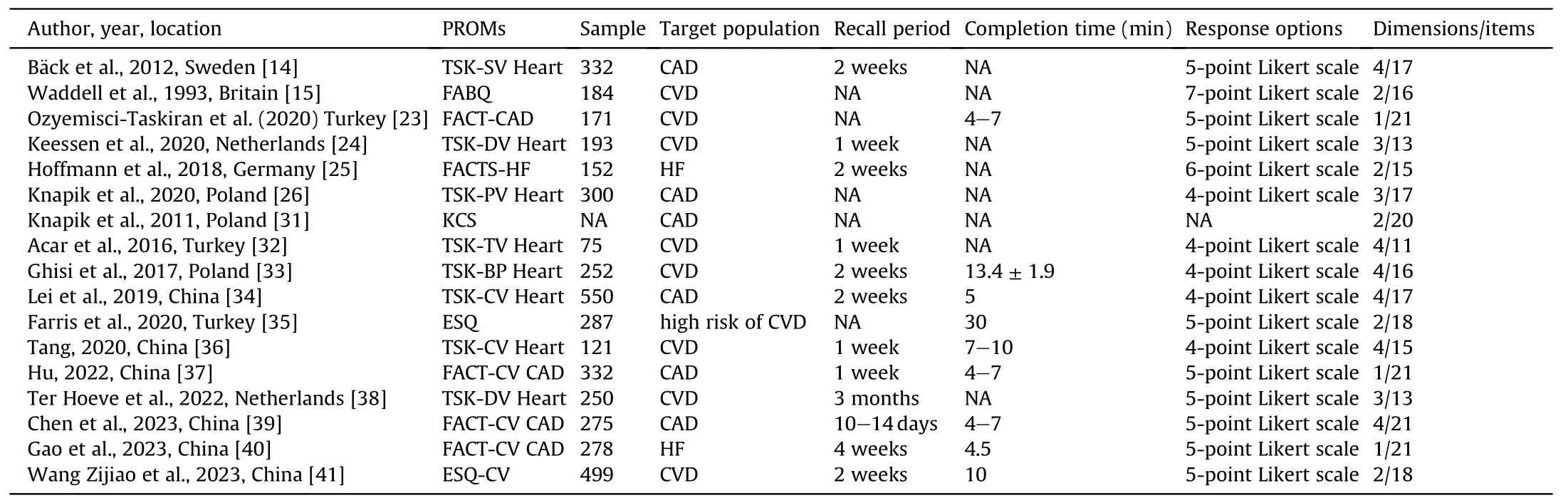
Table 1 Basic characteristics of the included literature(n=17).
3.2.Evaluation of the methodological quality of the included assessment tools and the quality of the measured attributes
Table 2displays the methodological and measurement attribute quality ratings.Regarding PROMs development,six studies did not adequately report the development process of the scale in terms of relevance,comprehensiveness,and understanding,leading to a“doubtful” assessment of their methodological quality [15,25,31,33,35,38].
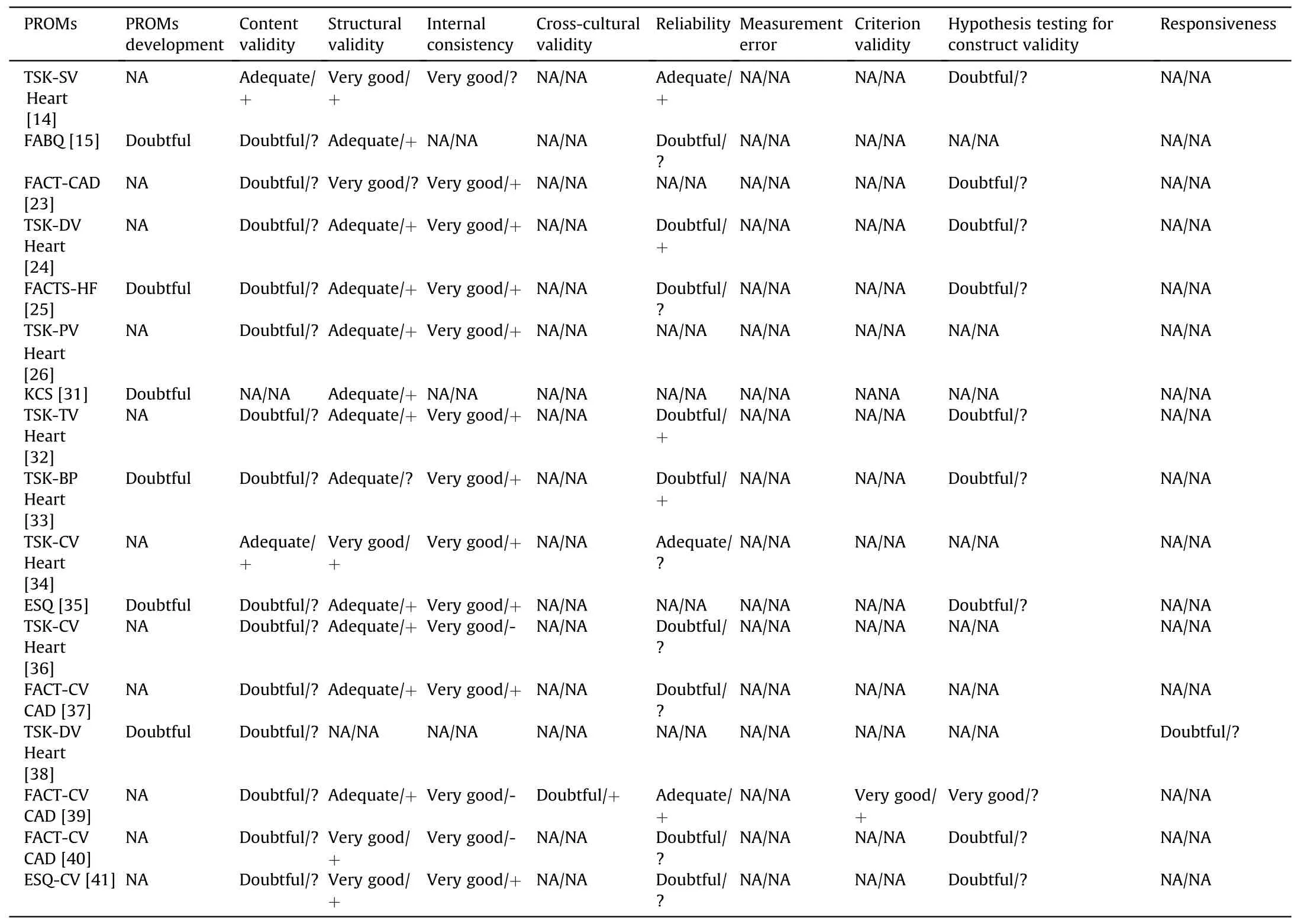
Table 2 Incorporate evaluation of the methodological quality of assessment tools and the quality of measurement attributes(n=17).
3.2.1.Validity
3.2.1.1.Content validity.The Swedish and Chinese versions of the TSK Heart demonstrated good content validity,as the research team consulted with panels of experts and patients regarding the relevance,comprehensiveness,and comprehensibility of the scales,rendering the methodological quality of the content validity “adequate” [14,34].One study did not mention content validity [31].The remaining studies had limitations such as relying solely on surveys to assess content validity,lacking qualitative analysis,and insufficiently specific and detailed descriptions of research processes/statistical methods.Thus,their methodological quality was rated as “ambiguous,” and the content validity of the evaluated scales was “uncertain.”
3.2.1.2.Structural validity.According to the COSMIN guidelines,validated factor analysis is recommended for evaluating structural validity.Eleven studies used only exploratory factor analysis and were rated “adequate” in methodological quality[15,24-26,31-33,35-37,39].All other studies,except for Ter Hoeve’s,performed validated factor analyses with adequate sample sizes and were thus rated very good.The cumulative variance contributions of the scales in the fourteen studies ranged from 52.15% to 73.73%,all exceeding 50%,and therefore,their measurement properties were evaluated as “adequate”[14,15,24-26,31,32,34-37,39-41].Two studies did not report necessary information like fit indices for the scales,making theirmeasurement attributes “questionable” [23,33].
3.2.1.3.Hypothesis testing for construct validity.One study used a control instrument with sufficient measurement properties in a similar population,leading to a “very good” rating for the methodological quality of its hypothesis test for validity [39].Nine studies employed control instruments with adequate measurement properties,but it was uncertain if these properties applied to their study populations,resulting in a “doubtful” rating for their methodological quality [14,23-25,32,33,35,40,41].
3.3.Reliability
3.3.1.Internal consistency
Fourteen studies reported internal consistency for each unidimensional scale or subscale,resulting in a“very good”rating for the methodological quality of internal consistency [14,23-26,32-37,39-41].The subscales in three studies had a Cronbach’s α coefficient lower than 0.7.Their measurement properties were evaluated as “inadequate” [36,39,40].
3.3.2.Stability
According to the COSMIN guidelines,intragroup correlations should be calculated,indicating patient stability during the retest period and the similarity of retest conditions.Only three studies adequately described patients in the retesting transition period;hence,their methodological quality was rated as “adequate”[14,34,39].The remaining studies were considered “questionable”methodological quality due to the lack of reported information on appropriate measurement intervals and the similarity of conditions under which measurements were taken.Only five studies reported the Intraclass Correlation Coefficient range of the scale,earning a “+” rating[14,24,32,33,39].
3.4.Other measurement properties
None of the studies reported measurement errors.Two studies respectively addressed the responsiveness and cross-cultural validity of the scale[38,39].Only one study used the TSK Heart as a gold standard and calculated correlation coefficients between the scales.Therefore,its methodological quality was rated“very good”[39].
3.5.Evaluation of the level of evidence for incorporating assessment tools and recommendation of evidence
Combining the four downgrading factors of the GRADE evidence grading from the modified version of the COSMIN guidelines,different levels of downgrading were applied to the measurement properties of each scale.The Chinese and Swedish versions of the TSK Heart provided high-quality evidence on psychometric properties [14,34].The remaining instruments were graded “B.”
In terms of risk of bias,the methodological quality of the content validity of the Swedish Version of the TSK Heart(TSK-SV Heart)[14]and the TSK-CV Heart[34]was adequate,and the rating of the level of evidence was moderate,while the methodological quality of the content validity of the remaining scales was ambiguous and the rating of the level of evidence was low.The methodological quality of the structural validity of the TSK-SV Heart [14],TSK-CV Heart [34],Chinese Version of the ESQ(ESQ-CV)[41],FACT-CAD[23],and the FACT-CV CAD [40] was very good,with a rating of high on the level of evidence,and the methodological quality of the structural validity of the rest of the scales was adequate,with a rating of medium on the level of evidence.The methodological quality of internal consistency for all scales was very good,and the level of evidence rating was high.The methodological quality of the crosscultural validity of the FACT-CV CAD [39] was ambiguous,with a low rating on the level of evidence.The methodological quality of the reliability of the TSK-SV Heart [14],TSK-CV Heart [34],and FACT-CV CAD [39] was adequate,and the rating of the level of evidence was medium,while the methodological quality of the reliability of the rest of the scales was ambiguous,and the rating of the level of evidence was low.The methodological quality of the criterion validity of FACT-CV CAD[39]was very good,and the rating of the level of evidence was high.The methodological quality of the hypothesis testing for construct validity of FACT-CV CAD [39] was very good,and the rating for the level of evidence was high.The quality of the responsiveness of the TSK-DV Heart [38] was ambiguous,and the rating for the level of evidence was low.The content validity,structural validity,and reliability of the TSK-CV Heart [34,36] were inconsistent,and each was downgraded by one level.There was no inconsistency in each measured characteristic of the TSK-DV Heart [24,38],and it was not downgraded.The FACT-CV CAD’s [37,39,40] structural validity,reliability,and hypothesis testing were inconsistent,and each was downgraded by one level.Regarding imprecision,the Turkish Version of the TSK Heart (TSK-TV Heart) [32],with a sample size of 75,had an insufficient sample size and was downgraded one level.Regarding indirectness,the ESQ [35] had differences between the study population and the original target population,down one level.Table 3 details the specific grading results of the scale.
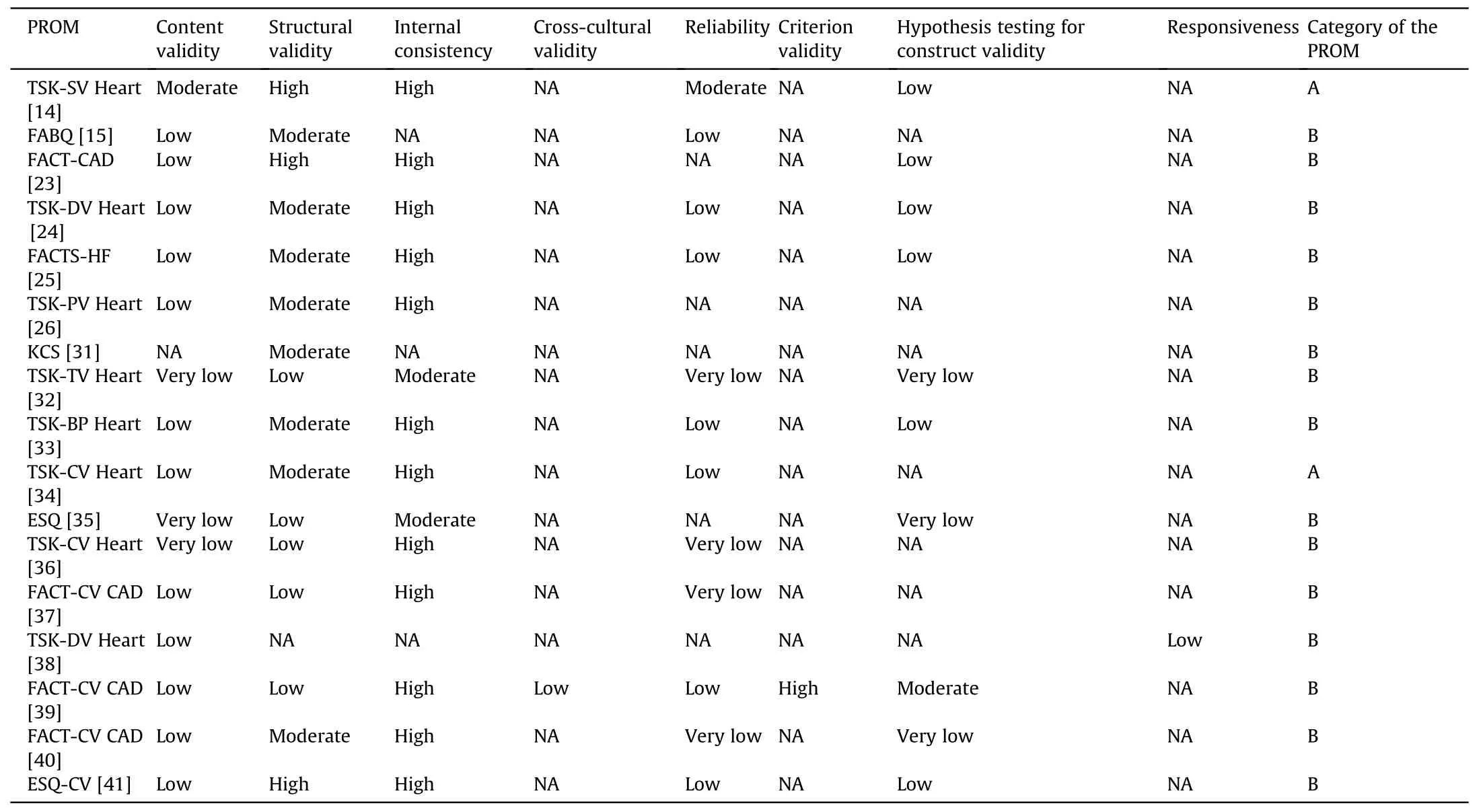
Table 3 The evidence level and recommendation of evidence included in the evaluation tool (n=17).
4.Discussion
This systematic review included 17 articles.According to the COSMIN methodology,six scales assessing fear of exercise in patients with CVD were evaluated for methodological risk of bias,psychometric property ratings,and quality of evidence.The findings provide quantitative evidence for researchers and healthcare professionals to select patient-reported outcome indicators to measure the level of exercise fear in patients with CVD.
4.1.The assessment contents of different exercise phobia scales vary and emphasize different aspects
The assessment tools included in this study assessed the level of exercise fear in patients with CVD from multiple perspectives,but each had its own focus.The TSK Heart measures patients’ fear of sports injuries in four dimensions: danger perception,exercise avoidance,exercise fear,and dysfunction [34].The TSK Heart is available in several languages and can be applied to various clinical conditions.However,the scale entry lacks CVD-specific content on exercise fear [14,24,34].The Fear Avoidance Beliefs Questionnaire (FABQ)focuses on measuring patients’fear avoidance beliefs about physical activity and work,but the scale lacks a recognized threshold for fear avoidance beliefs[15].The Kinesiophobia Causes Scale (KCS) aims to identify the causes of agoraphobia both biologically and psychologically,but it is available in fewer language versions and is not as widely used as scales such as the TSK Heart and FABQ[31].The Fear of Activity in Situations with Heart Failure Questionnaire (FACTS-HF) was used to assess the exercise fear response of heart failure patients with different exercise intensities in different contexts (daily life,exercise training,leisure,and recreation),and it can be used as a reliable tool for assessing exercise fear in symptomatic and stabilized heart failure patients.The scale has been used less frequently in clinical practice,and a largesample study is needed to validate its reliability and validity [25].The FACT-CV CAD assesses the level of exercise fear in patients with coronary artery disease in terms of their feelings,attitudes,beliefs,and physical activity ability,but the scale lacks large-sample,multicenter studies,and its measurement characteristics can be further refined in the future [37,39,40].The ESQ measures the cardiorespiratory and somatic perception of exercise intensity from the dimensions of Pain/Weakness Sensations and Cardiopulmonary Sensations to reflect the patient’s fear of exercise.The scale also lacks a large sample size of studies and is less commonly used in clinical settings [35,41].The above tools have different evaluation contents and differences in focus.In the future,researchers can develop an exercise fear scale for patients with CVD that meets China’s national conditions and combines the needs of patients with CVD.
4.2.Methodological quality of exercise fear assessment tools for patients with CVD needs to be improved
The COSMIN guideline emphasizes evaluating assessment tools’methodological quality in relevance,comprehensiveness,and comprehension.Content validity is deemed the most crucial aspect of this evaluation [27,29,30,42].Thus,the COSMIN risk of bias assessment checklist mandates an assessment of whether the included studies have reported evaluations by patients,experts,developers,and others on the relevance,comprehensiveness,and comprehensibility of the assessment tools through interviews or quantitative surveys.However,most scales in this study assessed content validity solely through expert consultation,largely overlooking the perspectives of study participants on the relevance,comprehensiveness,and clarity of the scale items.This oversight resulted in a “questionable” methodological quality rating for content validity in only two studies.Future research endeavors need to understand the COSMIN criteria when developing or translating scales comprehensively.Researchers should also consider incorporating qualitative interviews and quantitative surveys to gather insights from patients and experts,enhancing the methodological quality of assessment tools [27].
4.3.TSK-SV Heart and TSK-CV Heart can be tentatively recommended for use
Measurement error was not reported for any assessment instruments included in this study,and only two studies [38,39] reported scale responsiveness and criterion validity.Measurement error encompasses systematic and random errors when scoring the scales.If the minimum detectable change exceeds the standard measurement error,it suggests that any change in scale scores is due to a random error rather than a systematic one.Responsiveness,on the other hand,refers to a scale’s ability to detect small but meaningful changes in characteristics,such as differentiating between various groups or the same group at different stages [30].
Currently,the development and validation of fear of exercise assessment tools for patients with CVD are in a nascent stage.Future research should focus on examining measurement error,responsiveness,and other measurement characteristics in patients with CVD to enhance the scientific validity of these assessment tools.
Despite the assessment tools requiring significant improvement,the Swedish and Chinese versions of the TSK Heart show promise.They comprise four dimensions,possess an appropriate number of items,and can be completed within 5-15 min.The methodological quality of these scales is sufficiently robust,and they can be tentatively recommended for use.
4.4.Limitations of this study and suggestions for future research
This research underscores the strengths and limitations of existing scales for assessing kinesiophobia in patients with CVD,offering medical practitioners a baseline for evaluation and guiding future improvements in these scales.However,there are notable limitations in this study.Firstly,while the COSMIN checklist and measurement characteristic evaluation criteria are relatively mature,their interpretative outcomes can be subject to subjective biases.Secondly,the infrequent reporting of cross-cultural validity and measurement error by developers of PROMs limits the scope of the review’s findings to the currently available evidence.
Suggestions for future research include a more holistic approach to evaluating the quality of methodology and measurement properties.Additionally,the appropriateness of assessment tools for the intended population should be a key consideration.For example,the TSK Heart,initially developed for persistent musculoskeletal pain,has been adapted for patients with CVD.While it demonstrates good reliability and validity,it lacks specificity and targeted applicability for CVD,underscoring the need for disease-specific considerations in future research tool selection.
Furthermore,differing criteria for identifying high levels of motor phobia,as evidenced in Keessen andresearch[14,24],present a challenge.The absence of a unified criterion for identifying high levels of kinesiophobia impedes the timely detection and intervention in severe cases.Future research should focus on establishing a standardized criterion for identifying high levels of motor fear,enhancing the clinical applicability of the scale.
5.Conclusion
The Swedish and Chinese versions of the TSK Heart are tentatively recommended for assessing kinesiophobia in patients with CVD,owing to their robust methodological quality and superior measurement properties.For scales categorized as Level B,healthcare providers are advised to adhere to the COSMIN guidelines for further psychometric evaluation of the Kinesiophobia Scale.Special attention should be given to the infrequently assessed characteristics,with necessary adjustments based on these evaluations.This approach will help ensure that the scales used are scientifically valid and tailored to the specific needs and characteristics of the patient population being assessed.
Funding
This work was supported by the Project Supported by Scientific Research Fund of Zhejiang Provincial Education Department[Y202352490].Funding organizations played no role in the design,implementation and analysis of the survey.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
CRediT authorship contribution statement
Yingying Jia:Conceptualization,Methodology,Data curation,Writing -review &editing.Nianqi Cui:Validation,Methodology,Writing -review &editing,Supervision.Tingting Jia:Methodology,Validation,Formal analysis,Data curation,Writing-review&editing.Hammza Jabbar Abdl Sattar Hamoudi:Methodology,Writing -review &editing.Jianping Song:Supervision,Project administration,Funding acquisition,Writing -review &editing.
Declaration of competing interest
The authors declare that they have no competing interests.
Appendices.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.12.016.
杂志排行

International Journal of Nursing Sciences的其它文章
- Editorial Board of International Journal of Nursing Sciences
- Chinese Abstract
- Corrigendum to “Relationship between nurses’ perception of professional shared governance and their career motivation in Egypt:A cross-sectional study” [Int J Nurs Sci 10/4 (2023) 485-491]
- 《国际护理科学(英文)》进入中科院分区护理类2 区
- 关于翻译量表使用授权的问答
- Summary of Guide for Authors