Quality of life and depression among patients with high myopia in Nigeria: a cross sectional study
2023-12-14UchechukwuLeviOsuagwuKelechukwuEnyinnayaAhaiweNnaemekaMeribeElizabethDennisNkangaBernadineNsaEkpenyongAffiongAndemIbangaPiwunaChristopherGosonDennisGeorgeNkanga
Uchechukwu Levi Osuagwu, Kelechukwu Enyinnaya Ahaiwe, Nnaemeka Meribe, Elizabeth Dennis Nkanga, Bernadine Nsa Ekpenyong, Affiong Andem Ibanga, Piwuna Christopher Goson, Dennis George Nkanga
1Bathurst Rural Clinical School (BRCS), School of Medicine,Western Sydney University, Bathurst, NSW 2795, Australia
2African Vision Research Institute, University of KwaZulu-Natal Durban, Durban 4001, South Africa
3Department of Ophthalmology, University of Calabar Teaching Hospital, Calabar, Cross River State 540281, Nigeria
4Department of Politics, Media and Philosophy, La Trobe University, Melbourne, Victoria 3086, Australia
5Department of Ophthalmology, Faculty of Clinical Sciences,University of Calabar, Cross River State 540281, Nigeria
6Department of Public Health, University of Calabar, Calabar,Cross River State 540281, Nigeria
7Department of Psychiatry, College of Health Sciences,University of Jos, Jos, Plateau 930001, Nigeria
Abstract
● KEYWORDS: myopia; uncorrected refractive error;vision impairment; low vision; quality of life; Africa
INTRODUCTION
Myopia occurs when the image of a distant object of regard falls in front of the retina with accommodation relaxed resulting in a blurred image[1].Global myopia prevalence has been reported to be about 23% with an estimated increase to about 50% of the world’s population by 2050 with about 10% expected to have high myopia(≤-5.00 D)[2-3].High myopia, which is reported to affect about 2.7% of the world’s population[2], increases the risk for blinding conditions such as myopic macular degeneration,glaucoma and retinal detachment[4-5].In Africa, the overall crude prevalence of childhood myopia and high myopia was estimated at 4.7% [95% confidence intervals (CI), 3.9-5.7] and 0.6% (95%CI: 0.2%-1.1%)[6-7]among children aged 5-16y, and for adults, the prevalence is higher reaching 33.5%[8].
Uncorrected refractive error is a major cause of low vision,globally[6,9-11]and in Nigeria[12].Low vision is defined as an impairment of visual functioning with a distance visual acuity of less than 6/18, or visual field of equal to or less than 20 degrees, in the better eye, even after refractive correction and medical or surgical treatment[13-14].Myopia related complications pose even more danger since those affected are exposed to a high risk of blindness[5].For under corrected myopes, myopia progression is higher compared to those who are adequately corrected[7,15-16].Uncorrected myopia has social and economic implications[17]with impacts including low quality of life, poor academic performance among students, low work output, reduced employability as well as high financial cost[17-18].In 2015, the global potential loss of productivity from visual impairment due to uncorrected myopia was estimated at $244 billion[19].
The impacts of vision impairment (VI) and blindness are wide-reaching, including an increased risk of falls, cognitive impairment and dementia, depression, disability, and loss of independence[20-21]as well as, an increased risk of mortality[22].According to the world report on vision, vision loss and blindness resulted in 26.5 million global years of healthy life lost due to disability (YLDs) in 2019, 3.1% of total global YLDs from blindness due to VI[23].Impaired vision and poor eye health have a negative impact on the quality of life measured using generic, vision-specific, or disease-specific tools[24].Assessment of the quality of life (QOL) has become an important measure of the impact of eye health on the daily activities, well-being, and visual function of individuals with vision problems[25].
Depression is a common disease that limits psychosocial functioning[26].It is associated with painful mental and physical symptoms, and diminishes quality of life[27].Additionally, loss of QOL has been reported among people with major depressive disorders even with mild symptoms[28], hence barriers to meeting the sustainable development goals of equitable access to and achievement in education and the workplace[29].
Vision loss has many causes that require promotional, preventive,treatment, and rehabilitative interventions including measures to appropriately address the needs of our communities[30].Past review study[31]found that most studies on QOL of people with visual impairment have focused on eye diseases such as glaucoma, cataract, age-related macular degeneration, and diabetic retinopathy[32-36]while the few studies that investigated the QOL and depressive symptoms among individuals with myopia were mostly from Asia[37-38].They concluded that despite substantial differences in methodological approach, the studies agreed that VI significantly affects QOL[31].Considering that myopia is projected to be the highest cause of VI in Africa,similar studies are needed to understand the impact of myopia on QOL and life satisfaction.
At the time of this study, no study has investigated the QOL or depression among people with myopia especially high myopia in Nigeria, even though high prevalence of depression[36]and significantly reduced QOL[36,39]have been reported among individuals with vision impairment and blindness due to ocular diseases.Given the recent and projected continued rise in prevalence of myopia across Africa, myopia has become a public health concern[6-7], and this present study aims to investigate the QOL and burden of high myopia among adults in Nigeria.
SUBJECTS AND METHODS
Ethical ApprovalEthical approval for this study was obtained from the Health Research Ethics Committee, University of Calabar Teaching Hospital (NHREC/07/10/2012).Written informed consent was obtained from all participants.Study was conducted in line with the awarding Ethics Committee Board and Helsinki Declaration requirements in studies involving human participants.
Study Setting and DesignThe study was conducted in Calabar, at the Out-Patients Department of Benita Eye Clinic;Zerah International Eye hospital and Laser Centre; and the Eye Clinic of the University of Calabar Teaching Hospital,representing primary, secondary, and tertiary levels of eye care respectively.Calabar has a population of 371 022 as at 2006 census[40-41].Administratively, the city is divided into Calabar Municipal Council and Calabar South Local Government Areas.
This was a cross sectional survey study conducted among adult participants living with vision impairment due to high myopia in Calabar Nigeria.Each participant completed a QOL and depression questionnaire using the World Health Organization QOL (WHOQOL-BREF) and the Beck Depression Inventory(BDI) scale, respectively to access the impact of their visual impairment on QOL and performance of activities of daily living.
ParticipantsParticipants were recruited through convenient sampling from adults with high myopia who registered and presented for appointment in the selected eye clinics in Calabar.Though there is absence of consistent standard grading for myopia[42], this study recruited participants with myopia of ≤-5.00 D and worse[43], uncorrected visual acuity less than 6/18 in the better seeing eye, and known regular spectacle prescription wearers.
Inclusion and Exclusion CriteriaParticipants were eligible to take part in this study if they provided informed consent,aged 18y and above; attended the participating clinics between 2ndOctober 2021 and 31stAugust 2022; were diagnosed and/or treated with high myopia ≤-5.00 D and had uncorrected Snellen visual acuity poorer than 6/18 in the better seeing eye, but are known regular spectacle prescription wearers over the last one year.Exclusion criteria for this study include those who had corneal defects such as keratoconus or any other anterior surface eye disease; had underlying ocular complications; and individuals with any other complication which hinders their ability to recall any experience such as Alzheimer’s disease,dementia.Pathological myopes were excluded from the study since such high myopia is associated with degenerative macular and extensive chorioretinal changes.
Data CollectionParticipants who consented to participate in the study completed self-administered hardcopy questionnaires at the clinic on their appoints during the study period from 2ndOctober 2021 to 31stAugust 2022.Preceding the study, the questionnaire was piloted among cohort of patients with high myopia who are known spectacle prescription wearers (data excluded from the final analysis) to familiarize with questions as well as ensure its suitability for the target population.
QuestionnairesThe brief version of the WHO’s QOL scale(WHOQOL-BREF)[44]derived from the WHOQOL-100 and have been used in various disease conditions[45]was utilized in this study.The questionnaire contains two items from the overall QOL and general health and another 24 items on satisfaction which is divided into four domains including seven items on physical health, six on psychological health,three on social relationships and the other eight items on environmental health.Each questionnaire item is rated on a 5-point Likert scale with scores ranging from 1 to 5 on a response scale.Using the guidelines[46], the raw domain scores were transformed to a 4-20 score and are scaled in a positive direction such that higher scores indicate higher QOL.The mean score of items within each domain was used to calculate the domain score.For comparison between domain, the scored are then transformed linearly to a 0-100-scale.
The validated BDI-II was used to assess level of depression since this tool has the highest sensitivity and specificity,due to its dimensionality focussing on symptom severity in major depressive disorder (MDD) patients as demonstrated in previous study[28].The BDI is a well-established instrument used for the quantification of depressive symptoms.The questionnaire consists of 21 self-administered items that are primarily derived from clinical practice[47]to assess the cognitive, affective, and somatic symptoms of depressive disorders.Each item is answered with a series of four or five statements.These statements are arranged according to the severity of the symptom—from absent to very severe—and assigned a numerical value of zero to three, respectively.The total score ranges from 0 to 63 points and is obtained by adding up the scores for each item to reflect the severity levels.A researcher (Ahaiwe KE) administered the questionnaires to all patients before their vision assessment.
Dependent and Independent VariablesFour domains of WHOQOL-BREF questionnaire and depression score were considered as dependent variables.Data for age groups in years (16-29, 30-59, and 60 and over), sex, highest level of education, marital status, working status (not working included retired/student/unemployed, and working included public servants and self-employed), work type (skilled or unskilled),income level (per month based on the current minimum wage in Nigeria), residence (urban/semi-urbanvsrural) were taken as independent variables.
Statistical AnalysisThe information collected was organized with the SPSS software, version 27.Data were presented using descriptive statistics including proportion, means(standard deviations, SD) where appropriate and for the mean difference between comparisons, the 95%CI of the means were reported.Cronbach’s alpha (internal consistency index) was used to estimate the reliability of the WHOQOL-BREF.The Cronbach’s alpha coefficient was adequate (0.89) for all 26 questions[48]and the values for each domain was as follows:physical health domain (0.68), psychological health domain(0.72), social relationship domain (0.60) and environmental health domain (0.77).Pearson’s correlation coefficient (r)was used to determine the level of agreement between four domains of WHOQOL-BREF.Pairedt-test was used to compare difference between score means of different domains of WHOQOL-BREF.Although different cut-off scores have been proposed in studies with different objectives using the BDI and with samples having different characteristics, Becket al[49]advised that the cut-offscore adopted for a diagnosis of depression using the BDI tool should be based on the objectives and characteristics of the study sample.For this study, we used 0-10 points for “not depressed”, 11-17 points for“mild to moderately depressed”, and 18-63 points for “clinically relevant depression”[47].To investigate the association between participants’ characteristics and the dependent variables (QOL and depression scales), independentt-test and Fishers exact test were used, where relevant.Multivariable analysis using general linear model was performed to control confounding effects.Transformed scores for QOL scales were used forstatistical analyses in four domains.In this study, the level of significance was set atP<0.05 for all analyses.

Table 1 Characteristics of study population
RESULTS
A total of 100 participants with high myopia, mostly aged 16-29y (53%) completed the study.There was no missing data for the WHOQOL-BREF questionnaire, so all data were included in the study.Table 1 presents the characteristics of study population, showing that the participants were mostly women(77%), majority were employed (61%), not married (62%)and more than two thirds (82%) had a tertiary qualification(university or postgraduate degree).Although the average salary of the participants was 86 505±11 (range 3000-500 000)Naira, about one in three persons earned below the minimum wage of 30 000 Naira at the time.
Analysis of the Quality-of-Life ScoresTable 2 presents the mean scores and standard deviations (SD) for each of the items.Except for the overall QOLitem, the maximum score for other items was 5.There were reductions in the mean QOL scores for financial support, mobility and overall health score of 3.13±1.02 out of 5.00, but good score was observed for overall QOL (2.79±0.46) out of 3.00.

Figure 1 Percentage of mean scores for health satisfaction among participants with high myopia WHOQOL-BREF: The World Health Organization Quality of Life Brief Version.

Table 2 Response pattern for each item mean±SD
The correlation coefficients and the results of pairedt-test comparisons between the four domains of WHOQOL-BREF are shown in Table 3.All the domains were statistically significantly correlated.The mean percentage scores were significantly different between three different domains of WHOQOL-BREF, but the scores were similar between psychological health and social & relationship domains (-2.21,95%CI -5.10-0.68,P=0.132).
As seen in Table 2 and Figure 1, among the different domains,the highest and the lowest mean percentage of satisfaction were found for psychological [mean percentage=67.0 (95%CI 64.1-68.9)] and physical health [mean percentage=55.3 (95%CI51.8-58.8)] respectively, which were significantly different(P<0.0001).

Table 3 Comparison between the four different domains of the WHOQOL-BREF questionnaire
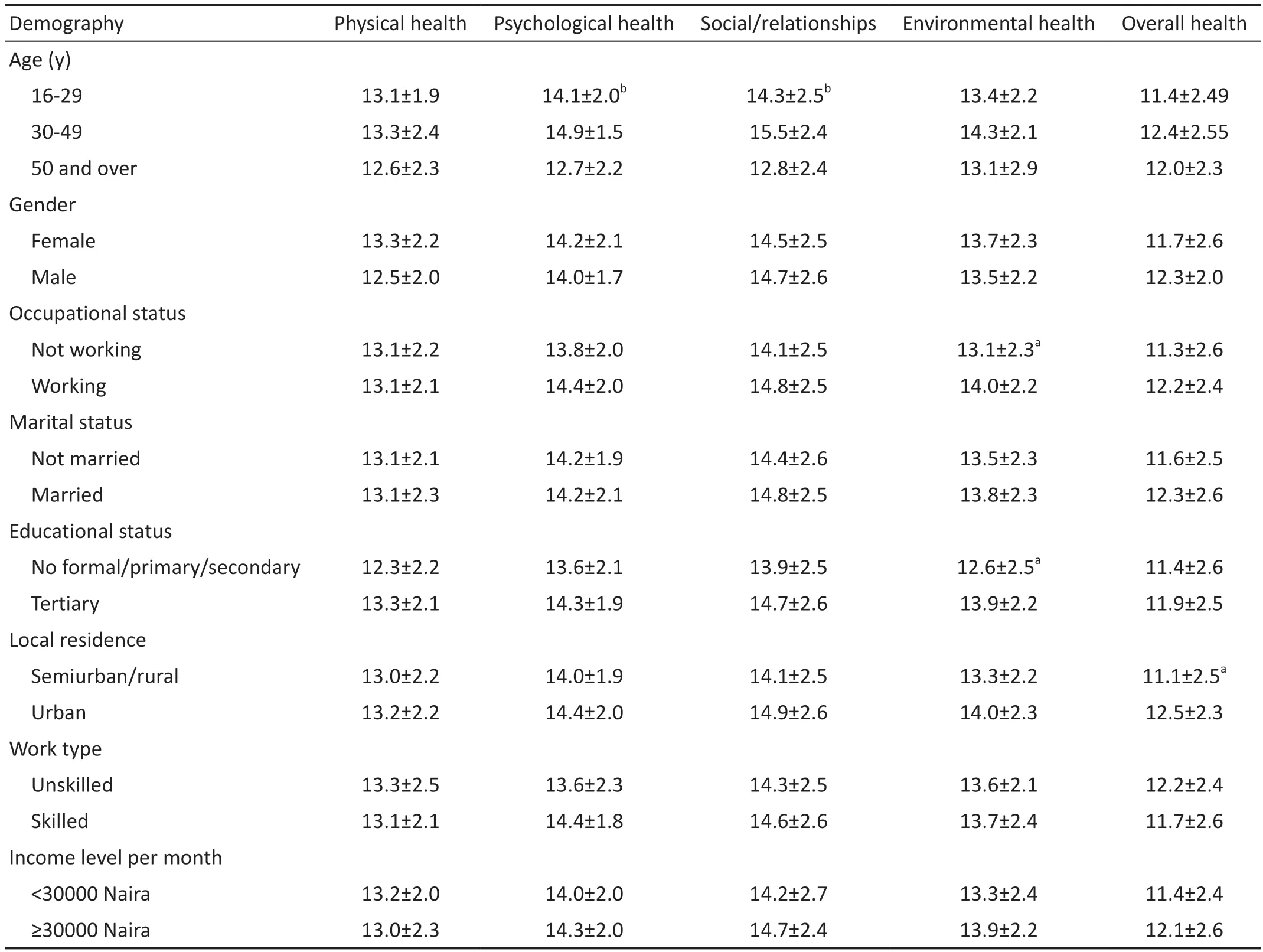
Table 4 Comparison of the WHOQOL-BREF scores in four domains according to the demographic variables mean±SD
The mean score of the four domains and total of WHOQOLBREF according to sex, age, education years, marital status,employment type, income level, job background, chronic disease existence and local residence separately are presented in Table 4.The mean scores for psychological health and social/relationship domains were statistically significantly different between age groups, while that for environmental health domain varied significantly by occupational and educational status of the participants.Those who lived in the urban region had significantly higher mean scores for overall health compared with those who lived in the semiurban/rural regions (12.5±2.3vs11.1±2.5,P<0.05).
Multivariate analysis using general linear model revealed significant associations between educational status and physical health (higher among those with tertiary qualification:mean difference was 0.9, 95%CI -0.2, 2.1), working status and psychological health (higher among those who were working 1.2, 95%CI 0.3-2.1), marital status and environmental health(higher among non-married: 1.7, 95%CI -0.9, 2.3) and between place of residence and the overall health (higher in urban areas:2.3, 95%CI 1.2-3.5).No other significant association was observed between the QOL domains and other demographic variables.

Figure 2 Distribution of participants by level of depression A Beck Depression Inventory (BDI) score of 0–10 points: not depressed; 11–17 points: mild to moderately depressed, and 18–63 points: clinically relevant depression.

Table 5 Associations of depression with individual characteristics of people with high myopia
Associations with DepressionFigure 2 shows the distribution of the participants by their levels of depression from the BDI scale.About one in every six individuals with high myopia reported mild depressive symptoms whereas one in every nine persons reported clinically relevant depressive symptoms in this study.
There were significant negative correlations between the depression scores and all the domains of the QOL scale in people with myopia (Figure 3) as well as the overall QOL score (Figure 4).Pearson correlation coefficient revealed moderate correlations for psychological health (Figure 3B),social and relationship (Figure 3C), environmental (Figure 3D) and a weak but significant correlation with physical health(r=-0.29,P=0.032; Figure 3A).Similarly, the mean score for depression was negatively correlated with the overall health of the participants as shown in Figure 4.
Table 5 presents the results of Fishers exact text for the associations between individual characteristics and depression in this study.Significant association was found between participants’ age and their level of depression (P=0.019), and the association with gender was approaching significance(P=0.064).There were significantly more women than men who reported symptoms of clinically relevant depression.
DISCUSSION
The increasing prevalence of myopia across the globe particularly in developing countries, and the lack of literature on prior studies investigating the mental health challenges associated with high myopia, necessitated this comparative study.To the best of our knowledge, this is the first study to investigate the impact of high myopia on the QOL and depression of adults in Nigeria, and the factors associated with both outcomes.Our study found that individuals with high myopia experienced moderate reduction in QOL, mostly in their physical health while the environmental health was the least affected.Consistent with previous study[39,50], the myopic participants in this study reported significant reductions in financial support, mobility and overall health scores.Unlike the present study which focussed on high myopia, the previous studies[36,39]included participants with more severe visual impairments including blindness and reported significantly poorer QOL in all domains (psychological, social, and physical) among the blind participants than those with normal vision.
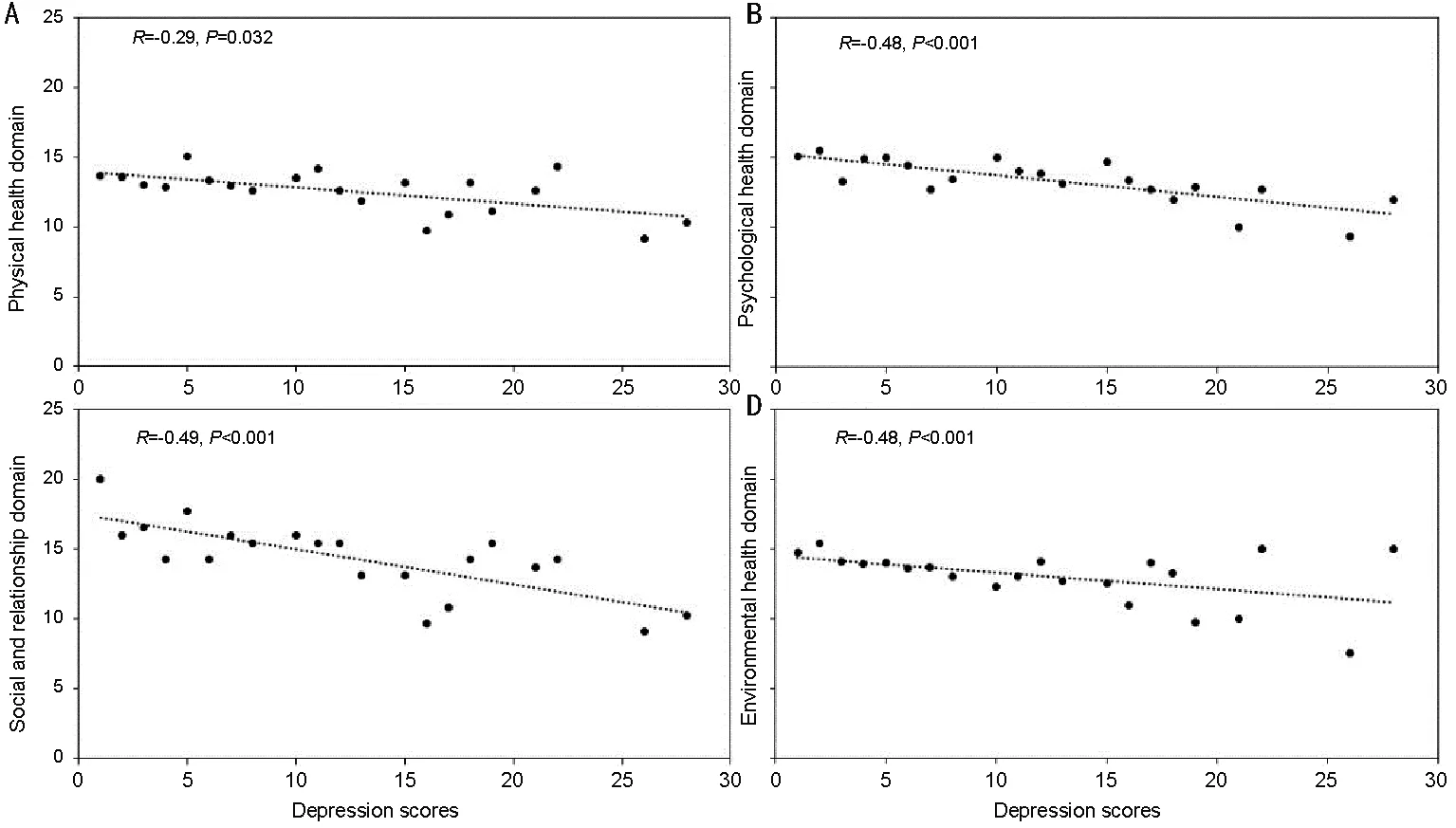
Figure 3 Correlation between physical health (A), psychological health (B), social and relationship (C) and environmental health domains (D),with depression in people with high myopia.

Figure 4 Correlation between overall health and depression in people with high myopia.
Other studies that investigated QOL among myopes were heterogeneous in their study population and the tool used, yet their findings corroborated the findings of this study that high myopia is associated with poorer or reduced outcomes for vision and health related measures of QOL[51-53].Nevertheless,the degree of reduction of the QOL of high myopes varied among the studies but using a different questionnaire, visionrelated QOL was significantly better after correction of high myopia in recent studies[54].For instance, while most studies found moderately reduced QOL, a study among diverse population in the UK considered high myopia from-10.00 D and found significantly poorer QOL in high myopes compared to other myopes, which was similar to the findings in keratoconus patients[53].Poorer QOL was demonstrated for uncorrected vision impairment with high myopia established as an independent risk factor[55].Reduced QOL in high myopes originates from poor vision which began in childhood and inflicted a lifelong disability on the individual[56-57].The reduction in QOL of people with myopia may be attributed to the fact that their employment, educational and personal relationship prospects may be curtailed, seriously affecting their psychological state and QOL[58].Even in those with mild visual impairment, negative outcomes on health, economic and social outcomes, have been reported which is due to the burden related to cost of correction[59], reduced confidence, loss of productivity and independence, leading to a reduced quality of life[60].
Employment, educational status, marital status, and location of residence demonstrated key impact on the mental health of participants in this study.In addition, the overall health of participants residing in urban areas recorded better QOL scores than those in the semi-urban and rural areas.This is understandable with the hindsight that basic amenities including eye care centres are situated more in the urban areas[61], hence giving people in urban areas better access to care and QOL.
Participant with employment showed better psychological health than unemployed as at the time of the study.Fear of vision loss due to inability to afford services may be responsible for this score.The direct health expenses related to myopia is high and inflict enormous economic burden on the individual.It is worse amongst the unemployed.Moreover, one in every three participants in the study earn below the national minimum wage in Nigeria and therefore live well below the poverty level.The national minimum wage of thirty thousand Naira (equivalent of $77) was enacted as a law in 2019 for federal workers in Nigeria[62].Despite limited literature on the economic evaluation of myopia to provide insight on the burden of high myopia.Evidence abounds that high myopia results in significant loss in productivity[63-64].About US $244 billion was estimated as the potential productivity lost from uncorrected myopia in 2015[65].Moreover, the global cost of myopia and direct cost in 2019 were projected to cost USD358.7 billion; and to substantially increase in the future as a result of the rising prevalence of high myopia[60].Contrasting findings to this study was the QOL score among Iranian blind war survivors which was relatively better in the physical component and may be attributed to financial support received from charity[66].
Participants possessing higher educational status had better score for physical health.Higher education has the potential of empowering an individual to make healthy choices as well as attracting additional income which may help reduce the challenging conditions unlike individual with basic education who are probably not skilled and whose productivity and source of livelihood is restricted by their poor vision.Ejiakoret al[39]concurs with this finding and explained that higher education attracts income from established channels which grants financial independence and better QOL.The overall health score for females was lower compared to the male participants.This is expected with the knowledge that high myopic corrections lenses are bulky and a potential source of worry for wearers particularly for young females who cannot afford contact lenses.This claim is supported by evidence that females are more concerned with cosmetic appearances than males[67].Furthermore, research among developed countries highlighted how high myopia exert psychological, cosmetic,practical, and financial impacts on the QOL of an individual as well as restrict activities of daily living including social life and professional activities[63].
Individuals who are married showed better environmental health in this study.This may suggest that sharing burdens associated with myopia have significant impact on health outcomes.Marital closeness has been found to demonstrate a clear association with mental or physical health issues;and the interconnectedness of couples leveraged on for promoting better treatment outcomes[68].The finding by Ejiakoret al[39]corroborated our finding and highlighted that widowed participants with vision impairments scored the lowest score for QOL compared to the married participants who are dependent on their spouses and may be unaware of further reduction in QOL.Another study suggests that marital status is important in the QOL of adults in that being married may provide a protective mechanism against mental health challenges[69].
Interestingly, this study found an association between high myopia and depression.One in every nine persons with high myopia have clinically relevant depressive symptoms.It is established that depression in ophthalmological practice constitute an important mental health problem and possible risk factors for the management and prognosis of the conditions, yet it is often unidentified and untreated[70].In their study, researchers[36]found a significant association between vision impairment and depression.Their study concurs with the findings of this study despite that this study was specific about the type of vision impairment and focussed on high myopia among adults.The finding of this study corroborated another study which found that the presence of myopia has a significant association with depression particularly among those without formal education and has the likelihood of deteriorating with old age[38].Another study highlighted that depression has association with high myopia; and constitute a major public health challenge among older adults with vision impairments[71].Yokoiet al[72]in their study further established a significant association between myopia and depression;and predicted 25% of patients with high myopia are likely to develop depression leading to reduced quality of health.
Significantly more women than men exhibit symptoms of depression of clinical relevance.This corroborates the WHO[73]finding that generally depression predominantly affect more women than men.In the USA, depression occurs about twice among women (11%) than men (6%)[74].Young adults (16-29y) have higher levels of depression than other age groups in this study.This is in agreement with a study in the USA which found that individuals aged 18-25 (17.0%) have the highest prevalence of adults with a major depressive episode[74].
This study has some limitations which should be considered when interpreting the results, including that it was conducted among people currently enrolled in an eye clinic for treatment and may have resulted in selection bias since the participants may be patients who are aware, health conscious or have the resources to access eye care services.A population-based study may provide more insight into the study.Also, even though this was a popular eye centre in the region, the use of a single hospital data may limit the generalization of our findings as people attending other centres like public hospitals may reveal different results.Despite these limitations, this study provided data for comparison with future studies to understand whether those attending other facilities or public hospitals have similar experiences.
In conclusion, the findings of this study revealed that high myopia moderately reduces the QOL of patients and this impacts all the domains of QOL especially for financial support, mobility, and overall health.Significant association was established between education and physical health;working status and psychological health; marital health and environmental health; and location of residence and overall health.Reduced QOL in high myopes results from adverse influences from psychological, cosmetic, practical, and financial factors and impacts on productivity, mobility, and other daily living activities.Depression of clinical relevance was significant among people with high myopia with young people and women predominantly affected.Nevertheless, it is recommended that an effective referral pathway is established for early mental health intervention considering that good QOL and stable mental health are important for the effective management and prognosis of myopia and other ocular health issues.
ACKNOWLEDGEMENTS
Authors’ contributions:Osuagwu UL, Meribe N, and Ahaiwe KE were involved in the conceptualization of the study; Nkanga DG, Osuagwu UL, Ahaiwe KE, Nkanga ED,Meribe N, and Ekpenyong BN performed the methodology;Software: Ahaiwe KE, and Osuagwu UL; Validation: Nkanga DG, Osuagwu UL, Ahaiwe KE, Nkanga ED, Meribe N, Goson PC, Ibanga AA, and Ekpenyong BN; Formal analysis: Ahaiwe KE, Meribe N, and Osuagwu UL; Investigation: All authors;Resources: Nkanga DG, Ekpenyong BN, Nkanga ED, and Ahaiwe KE; Data Curation: Ahaiwe KE, Ibanga AA, Nkanga DG, Nkanga ED, and Ekpenyong BN; Writing-original draft preparation: Osuagwu UL and Ahaiwe KE; Writing-review &editing: All authors; Visualization: Nkanga DG, Ekpenyong BN, Nkanga ED, Ibanga AA, Meribe N; Supervision: Ahaiwe KE, Meribe N, Nkanga DG, and Osuagwu UL; Project administration: Ahaiwe KE, Nkanga DG, Nkanga ED, Ibanga AA, and Ekpenyong BN.All authors reviewed the manuscript,read and agreed to the published version of the manuscript.
Conflicts of Interest: Osuagwu UL,None;Ahaiwe KE,None;Meribe N,None;Nkanga ED,None;Ekpenyong BN,None;Ibanga AA,None;Goson PC,None;Nkanga DG,None.
杂志排行

International Journal of Ophthalmology的其它文章
- Dynamic tear meniscus parameters in complete blinking:insights into dry eye assessment
- Effects of diquafosol sodium in povidone iodine-induced dry eye model
- Morroniside ameliorates lipopolysaccharide-induced inflammatory damage in iris pigment epithelial cells through inhibition of TLR4/JAK2/STAT3 pathway
- Role of reactive oxygen species in epithelial-mesenchymal transition and apoptosis of human lens epithelial cells
- Electroacupuncture alleviates ciliary muscle cell apoptosis in lens-induced myopic guinea pigs through inhibiting the mitochondrial signaling pathway
- De novel heterozygous copy number deletion on 7q31.31-7q31.32 involving TSPAN12 gene with familial exudative vitreoretinopathy in a Chinese family