Giant dedifferentiated liposarcoma of the gastrocolic ligament: A case report
2023-12-05AssamoiBrouFulgenceKassiKacouSebastienYenonFianMarcHerveKassiAdjaJacobAdjemeKhaderMorelDiarraCynthiaBombetKouameMarcellinKouassi
Assamoi Brou Fulgence Kassi,Kacou Sebastien Yenon,Fian Marc Herve Kassi,Adja Jacob Adjeme,Khader Morel Diarra,Cynthia Bombet-Kouame,Marcellin Kouassi
Abstract BACKGROUND Dedifferentiated liposarcoma (DDLS) has a worse prognosis and occurs most commonly in the retroperitoneal region and rarely in the intraperitoneal region.Histological diagnosis was revolutionized by the combined contributions of histoimmuno-chemistry and molecular biology.Aside from surgery,there is no consensus on the optimal treatment for this chemoresistant cancer.CASE SUMMARY A thirty-year-old black female presented with a large painful abdominal mass occupying nearly the entire abdomen and progressive weight loss was admitted for surgery.Abdominal computed tomography showed a large heterogeneous mass of the mesentery that was sized 18 cm × 16 cm in size and had heterogeneous contrast enhancement.During laparotomy,en bloc excision of the large and multilobulated gastrocolic ligament mass was performed.The initial postoperative histopathological diagnosis was undifferentiated sarcoma.Finally,the results of immunohistochemistry and molecular biology allowed us to confirm the diagnosis of DDLS.The tumour followed an aggressive evolution with diffuse metastasis,causing the death of the patient less than 5 mo after the operation.CONCLUSION Dedifferentiated liposarcomas are rare tumours that typically originate in the retroperitoneum but may arise in unexpected locations.
Key Words: Dedifferentiated liposarcoma;Gastrocolic ligament mass;En bloc excision;Immunohistochemistry;Molecular biology;Worse prognosis;Case report
INTRODUCTION
Liposarcoma is a rare malignant tumour of mesodermic origin that derives from adipose tissue[1,2].Well-differentiated and dedifferentiated liposarcomas (DDLSs) are the most common retroperitoneal types[3].Liposarcoma is one of the most common soft-tissue sarcomas that mostly affects adults in their 50s or 60s[4,5].
DDLS,a variant of malignant adipocytic tumours,has a worse prognosis and occurs most commonly in a retroperitoneal location but rarely in an intraperitoneal location[6,7,8,9].Typically in these locations,the tumour is paucisymptomatic or even asymptomatic until it becomes large enough to compress the surrounding organs[10].The challenges of histological diagnosis and the lack of consensus on the optimal therapy complicate the management of this cancer[8,11].Histological diagnosis was revolutionized by the combined contributions of histo-immuno-chemistry and molecular biology[12].When the tumour is still localized,complete surgical excision with a negative microscopic margin (R0)remains the ideal treatment[10,13].Additional surgery,chemotherapy,radiotherapy and targeted therapies are also useful in the treatment of advanced or metastatic forms[11,14,15].
Herein,we report the case of a thirty-year-old black female with a giant DDLS of the gastrocolic ligament.To the best of our knowledge,DDLS originating from this unusual location has not been reported.
CASE PRESENTATION
Chief complaints
A thirty-year-old black female was admitted to our surgical unit with a large painful abdominal mass occupying nearly the entire abdomen.
History of present illness
This abdominal mass appeared eight months earlier.A gradual increase in its volume had been associated with the onset of abdominal pain,constipation and progressive weight loss.
History of past illness
The patient had a good health history.
Personal and family history
No notable events were mentioned in her personal and family history.
Physical examination
The patient was visibly underweight.She presented with an irregular and painful hard abdominal mass with a diameter of approximately 28 cm.
Laboratory examinations
Blood analysis revealed severe nutritional impairment and anaemia.The total protein level was 4.2 g/dL (normal range:5.8-6.5 g/dL),the albumin level was 2.8 mg/dL (normal range: 3.5-5.5 mg/dL) and the haemoglobin level was 10.5 g/dL(normal range: 12-16 mg/dL).
Imaging examinations
Abdominal computed tomography (CT) showed a large heterogeneous mesentery mass measuring 18 cm × 16 cm × 10.4 cm,and it was compressing the third part of the duodenum with heterogeneous contrast enhancement (Figure 1).
FINAL DIAGNOSIS
The final diagnosis of the presented case was DDLS of the gastrocolic ligament.
TREATMENT
At laparotomy,a large multilobulated mass that was sized 30 cm × 20 cm × 12 cm and arose from the gastrocolic ligament was found (Figure 2A).In addition,many other smaller synchronous lesions were discovered in the liver,small bowel mesentery and peritoneum.An en bloc excision of the giant mass of the gastrocolic ligament was carried out,and associated biopsies of the small lesions were taken.The other smaller lesions virtually ruled out any possibility of curative excision.
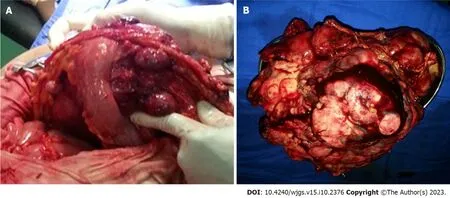
Figure 2 Operatives images of this case report. A: Intraoperative procedure found multi-lobulated mass of gastrocolic ligament;B: Macroscopic aspect of removed giant mass of gastrocolic ligament.
OUTCOME AND FOLLOW-UP
Symptomatic treatment,such as nutritional support,was given postoperatively.After two days,the patient was gradually redirected to a normal diet.The patient was discharged 8 d after surgery without any complications.The patient did not undergo any adjuvant treatment for economic reasons.Three months later,follow-up abdominal CT studies revealed multiple peritoneal and vascular implants.The tumour followed an aggressive evolution with diffuse metastasis,causing the death of the patient less than 5 mo after the operation.
Macroscopic examination showed a large yellowish,nodular and myxoid mass with focal areas of haemorrhage and necrosis (Figure 2B).
The histological examination revealed tumorous nodules that were poorly limited,often haemorrhagic,and located in fibrous or fibro-adipose tissue or in the peritoneum.The tumour proliferation was made up of masses with some fusiform cells (Figure 3A),which were sometimes more epithelioid (Figure 3B) and sometimes had pleomorphic nuclei.The mitotic rate was 10/10 per high power field.The tumour was not differentiated and was largely vascularized without necrosis.Immunohistochemical staining revealed that the tumour cells were negative for actin,desmin,calretinin,PS100,melana A,ERG,P63,AE1/AE3,EMA,chromogranin A and CDK4.BAP1 and P16 were partially positive in the neoplastic cells,while MDM2 was strongly expressed.The histo-pathological diagnosis was initially an undifferentiated sarcoma with fusiform and pleomorphic cells.The tumour was reclassified as DDLS according to the histopathological report and immu-nohistochemical test results.
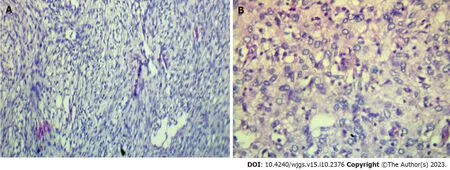
Figure 3 Histopathological analysis. Immunohistochemical results show that the tumours cells are positive for Bap1 (A),p16 (A) and MDM2 (B) and negative for actin,desmin,calretinin,PS100,melana A,ERG,p63,cytokeratin AE1/AE3,EMA,chromogranin A and CDK4.A: A population of fusiform cells (× 200);B: A population of epithelioid cells and atypical adipose cells in a myxoid and vascularized matrix (× 200).
DISCUSSION
The patient’s young age,unlike the cases usually reported and the rarity of its location at the gastrocolic ligament,makes our observation peculiar.Liposarcoma is the most common soft-tissue sarcoma in adults,with a peak incidence in the 5th-6thdecade of life[4,5].According to the World Health Organization,liposarcoma is classified into five main subtypes:Well-differentiated,dedifferentiated,myxoid,pleomorphic,and myxoid pleomorphic[6,14].DDLS is a higher grade,often nonlipogenic,sarcoma with metastatic potential that is genetically similar to well-differentiated liposarcoma[16].However,DDLS arisesde novoin more than 90% of cases[17] and can exist without any well-differentiated cells[18].Usually,DDLS are rare,located in the retroperitoneum and occasionally in the peritoneal cavity[6].Localizations in the ascending colon,sigmoid colon,mesentery of the small bowel and oesophagus have been described,but no localization in the gastrocolic ligament has been reported to our knowledge[7,19,20,21].Well-differentiated liposarcoma is typically associated with an adipose mass containing nonlipomatous components on abdominal CT and magnetic resonance imaging;the additional presence of a focal,nodular nonlipomatous region greater than 1 cm in size suggests DDLS[22].Histo-pathological diagnosis is difficult;initially,this case was diagnosed as an undifferentiated sarcoma with fusiform and pleomorphic cells.In fact,tumours are generally diagnosed as an undifferentiated pleomorphous sarcoma on histology;the diagnosis is suspected in the presence of a well-differentiated liposarcoma[23].It should be noted,however,that this well-differentiated component may be missing,as noted above.It has been reported that many cases of histological diagnosis of undifferentiated or poorly differentiated sarcoma located in the retroperitoneum were in fact DDLS[8].The molecular features of DDLS overlap with well-differentiated liposarcoma[24,25].In immunohistochemistry,both express MDM2 and CDK4 amplifications;MDM2 overexpression confirmed by fluorescencein situhybridization helps distinguish it from pleomorphic liposarcoma and myxoid liposarcoma[16].Radical surgery with R0 en bloc resection when possible,seems to offer longer survival and disease-free interval[14,18,26].In all reported cases,radical surgery was performed as the first-line treatment.However,surgically,it is difficult to distinguish the well-differentiated components of healthy fat,which complicates complete excision surgery[16].The most important prognostic factor for DDLS is the anatomic site,with retroperitoneal sites having an overall worse prognosis.In our observation,the numerous small lesions did not allow for curative excision,suggesting relapse,as seen three months later.Chemotherapy and radiotherapy remain poorly codified,and their therapeutic benefit has not yet been demonstrated[18].DDLS is not very sensitive to chemotherapy,so new molecular targets are based on an understanding of disease biology,usually targeting a specific,aberrant genetic or molecular pathway[27,28].Pazopanib,a tyrosine kinase inhibitor,may provide clinical benefit for patients with DDLS according to recent data[29].
The patient did not undergo any adjuvant treatment for economic reasons.Approximately 40% of DDLS will have local recurrence,17% will metastasize,and 28% will have tumour-related mortality[6].Three months later,follow-up abdominal CT studies revealed multiple peritoneal and vascular implants with necrotic areas.The patient died less than five months after surgery.
CONCLUSION
DDLSs are rare tumours that typically originate in the retroperitoneum but may arise in unexpected locations.The extremely rare primary gastrocolic liposarcoma presented here is an example.Immunohistochemistry and molecular biology are essential to confirm histological diagnosis.Surgical excision with oncologically appropriate margins is the gold standard of treatment.
FOOTNOTES
Author contributions:Kassi ABF proposed the idea,analyzed the literature,wrote and revised the manuscript according reviewers suggestions;Yenon KS supervised and revised the manuscript;Kassi FMH collected the data;Adjemé AJ and Diarra KM assisted with data collection;Kassi ABF,Yenon KS,Bombet-Kouamé C and Kouassi M were the patient’s surgeons and participated in the entire operation;All the authors have read and approved the revised manuscript.
Informed consent statement:Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Conflict-of-interest statement:All authors report no relevant conflicts of interest for this article.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Cote d'Ivoire
ORCID number:Assamoi Brou Fulgence Kassi 0009-0001-2060-0703.
S-Editor:Lin C
L-Editor:A
P-Editor:Wu RR
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Gastric adenosquamous carcinoma with an elevated serum level of alpha-fetoprotein: A case report
- Hereditary hemorrhagic telangiectasia involving portal venous system: A case report and review of the literature
- Mucocutaneous ulcer positive for Epstein-Barr virus,misdiagnosed as a small bowel adenocarcinoma: A case report
- Three-dimensional computed tomography reconstruction diagnosed digestive tract perforation and acute peritonitis caused by Monopterus albus: A case report
- Postpolypectomy syndrome without abdominal pain led to sepsis/septic shock and gastrointestinal bleeding: A case report
- Bariatric surgery reduces colorectal cancer incidence in obese individuals: Systematic review and meta-analysis