Maternal weight,blood lipids,and the offspring weight trajectories during infancy and early childhood in twin pregnancies
2023-12-02WeiZhengKeXinZhangXianXianYuanJinYingLuoJiaWangWeiSongShengNanLiangXiaoXinWangCuiMeiGuoGuangHuiLi
Wei Zheng · Ke-Xin Zhang · Xian-Xian Yuan · Jin-Ying Luo,3 · Jia Wang · Wei Song · Sheng-Nan Liang ·Xiao-Xin Wang · Cui-Mei Guo · Guang-Hui Li
Abstract Background The intrauterine environment has a profound and long-lasting influence on the health of the offspring.However,its impact on the postnatal catch-up growth of twin children remains unclarified.Therefore,this study aimed to explore the maternal factors in pregnancy associated with twin offspring growth.Methods This study included 3142 live twin children born to 1571 mothers from the Beijing Birth Cohort Study conducted from 2016 to 2021 in Beijing,China.Original and corrected weight-for-age standard deviation scores of the twin offspring from birth to 36 months of age were calculated according to the World Health Organization Child Growth Standards.The corresponding weight trajectories were identified by the latent trajectory model.Maternal factors in pregnancy associated with the weight trajectories of the twin offspring were examined after adjustment for potential confounders.Results Five weight trajectories of the twin children were identified,with 4.9% (154/3142) exhibiting insufficient catch-up growth,30.6% (961/3142),and 46.8% (1469/3142) showing adequate catch-up growth from different birth weights,and 15.0% (472/3142) and 2.7% (86/3142) showing various degrees of excessive catch-up growth.Maternal short stature [adjusted odds ratio (OR)=0.691,95% confidence interval (CI)=0.563–0.848,P =0.0004] and lower total gestational weight gain(GWG) (adjusted OR=0.774,95% CI=0.616–0.972,P =0.03) were associated with insufficient catch-up growth of the offspring.Maternal stature (adjusted OR=1.331,95% CI=1.168–1.518,P <0.001),higher pre-pregnancy body mass index(BMI) (adjusted OR=1.230,95% CI=1.090–1.387,P <0.001),total GWG (adjusted OR=1.207,95% CI=1.068–1.364,P =0.002),GWG rate (adjusted OR=1.165,95% CI=1.027–1.321,P =0.02),total cholesterol (TC) (adjusted OR=1.150,95% CI=1.018–1.300,P =0.03) and low-density lipoprotein-cholesterol (LDL-C) (adjusted OR=1.177,95% CI=1.041–1.330) in early pregnancy were associated with excessive growth of the offspring.The pattern of weight trajectories was similar between monochorionic and dichorionic twins.Maternal height,pre-pregnancy BMI,GWG,TC and LDL-C in early pregnancy were positively associated with excess growth in dichorionic twins,yet a similar association was observed only between maternal height and postnatal growth in monochorionic twins.Conclusion This study identified the effect of maternal stature,weight status,and blood lipid profiles during pregnancy on postnatal weight trajectories of the twin offspring,thereby providing a basis for twin pregnancy management to improve the long-term health of the offspring.
Keywords Maternal weight · Multifetal · Offspring growth · Twin pregnancy
Introduction
With the development of assisted reproductive technology,the multifetal gestation rate has risen dramatically over the past decades,95% of which are twins [1,2].The incidence of twin pregnancies has reached 3.26% of all births in the United States [2],2.3% in Brazil,and 3.3% in China [3].Multiple gestations usually present considerable health challenges,including elevated risks of maternal complications and adverse offspring health outcomes,compared with singleton pregnancies [2,4].The primary consequential offspring outcomes are preterm birth and low birth weight(LBW),followed by resultant infant growth and development retardation [2].
The reported preterm birth rate and LBW rate in twin gestations were up to 60% and 50%,respectively [1,3].Preterm birth and LBW have been associated with higher risks of infant morbidity and mortality [5],impaired growth and cognitive development [6],and long-term health consequences,including poor school performance and higher incident cardiovascular disease [7–9].Postnatal catch-up growth is a common compensatory mechanism for twin infants with intrauterine growth restriction,usually occurring in early infancy.Optimum catchup growth has been associated with a reduced risk of hospitalization [10] and is favorable for neurodevelopment [11,12].However,recent studies have challenged the benefits of catch-growth by proposing that it did not improve long-term health outcomes [10,13–15].One plausible explanation for this paradox is that excessive catch-up growth in LBW neonates increases the risk of overweight/obesity [10],thus leading to insulin resistance [13],high total cholesterol levels [10],and elevated blood pressure in adulthood [14–16].
Huang et al.identified divergent catch-up growth patterns in smallforgestationalage (SGA) children and suggested that maternal weight before and during pregnancy substantially affected the growth velocity of the offspring [17].The theory of the developmental origins of health and disease(DOHaD) has revealed that the intrauterine environment profoundly affects offspring fitness [18].However,current evidence on the association between maternal factors and offspring growth trajectories is limited to singleton pregnancies.Whether the catch-up growth trajectories in twin children that experience a considerably different intrauterine environment diverge from singleton children is unclear,and the maternal influencing factor in pregnancy also remains unclarified.
Therefore,this study aimed to identify the latent class of growth trajectories of twin children and to explore the associated maternal factors during pregnancy,thus providing insight into early intrauterine environmental interventions to improve the optimum growth of twin children.
Methods
Study design and participants
The study population was pregnant women with twin pregnancies and their offspring selected from the ongoing Beijing Birth Cohort Study (ChiCTR220058395) conducted from January 1,2016 to December 31,2021 in Beijing,China.Pregnant women aged between 18 and 44 years of the Han ethnic group were recruited during their visit to the Beijing Obstetrics and Gynecology Hospital for prenatal examination during the gestational age of 6–13 weeks.Women with singleton pregnancies,stillbirths,miscarriages,or neonatal death in one or both offspring and women without offspring anthropometric information were excluded.
The pregnant women in the cohort were followed by trained researchers until delivery,and their offspring were followed by the primary health care physicians until 36 months of age.The study was approved by the ethics committee of Beijing Obstetrics and Gynecology Hospital,Capital Medical University (2018-ky-009–01),and written informed consent was obtained from all the participants or their legal guardian.
Maternal indicators in pregnancy
Maternal anthropometrics were measured in the Beijing Obstetrics and Gynecology Hospital outpatient clinic.Prepregnancy weight was self-reported.Maternal pre-pregnancy body mass index (BMI) was calculated as pre-pregnancy body weight (kg) divided by height squared (m 2).Gestational weight gain (GWG) was defined as weight at delivery minus the pre-pregnancy weight,and GWG rate was defined as GWG divided by gestational age.Due to the lack of national GWG criteria for twin gestations in China,the adequate GWG and GWG rates were calculated according to the Institute of Medicine (IOM) criteria for twin pregnancies,i.e.,16.8–24.5 kg (0.45–0.66 kg/week) for normal weight/underweight women,14.1–22.7 kg (0.38–0.61 kg/week) for overweight women,and 11.3–19.1 kg (0.31–0.52 kg/week)for women with obesity [19].
Maternal baseline information was collected from electronic medical records.Preterm delivery was defined as gestational age <37 weeks.Hyperglycemia in pregnancy was classified as pre-gestational diabetes mellitus (PGDM)and gestational diabetes (GDM).PGDM refers to women who had diabetes mellitus before pregnancy.GDM refers to glucose tolerance abnormalities that occur in pregnancy by an oral glucose tolerance test (OGTT) during 24–28 weeks of gestation,diagnosed by the International Association of Diabetes and Pregnancy Study Group (IADPSG) Consensus Panel criteria [20].Hypertensive disorder complicating pregnancy includes preeclampsia,eclampsia,and chronic and gestational hypertension diagnosed according to the 2018 European Society of Cardiology (ESC) Guidelines for the management of cardiovascular diseases during pregnancy [21].Hemolysis,elevated liver enzymes,and low platelet (HELLP) syndrome,twin-to-twin transfusion syndrome (TTTS),intrahepatic cholestasis of pregnancy,anemia in pregnancy,and premature rupture of membrane were diagnosed according to the Williams Obstetrics 25th edition.
Maternal fasting blood lipid profiles,including total cholesterol (TC),triglyceride (TG),high-density lipoprotein-cholesterol (HDL-C),and low-density lipoproteincholesterol (LDL-C),were determined at 7–13 weeks and 32–34 weeks of gestation using an automatic biochemical immunoassay system (Architect ci8200;Abbott Laboratories,Chicago,IL,USA).Fasting blood glucose (FBG) levels at 7–13 weeks and 0 hours,1 hours,and 2 hours glucose levels in OGTT at 24–28 weeks of gestation were determined by the glucose oxidase method with a DxC800 automatic biochemical analyzer (Beckman Coulter Company,USA).
Offspring indicators
Offspring anthropometrics were measured in the Beijing Obstetrics and Gynecology Hospital and primary child healthcare.The follow-up time points were at birth,5–6 months,8–9 months,11–12 months,18 months,24 months,and 36 months of age.The feeding style of the offspring at 3–4 months was obtained from their caregivers.SGA and large-for-gestational-age (LGA) were defined as birth weight ≤ 10th percentile and ≥ 90th percentile according to the growth standard curves of Chinese newborns,respectively [22].Macrosomia and LBW were defined as neonatal birth weights ≥ 4000 g and <2500 g,respectively.
Outcome measurements
Weight-for-age (WFA) of the offspring during 0–36 months was classified as <− 2SD,− 2SD–− 1SD,− 1SD–1SD,1SD–2SD,>2SD according to the World Health Organization (WHO) Child Growth Standards [23].Since preterm births account for a substantial portion of twin births,we calculated the corrected age as postnatal age minus the difference between the gestational age and term age (40 weeks)and the corresponding corrected WFA according to the WHO standards.
Statistical analysis
WFA categories of the offspring from birth to 36 months were used for latent weight trajectory modeling.The latent trajectory model assumes that a heterogeneous population is composed of unknown subgroups ofindividuals.Latent class analysis is commonly used to simplify heterogeneous data into more homogeneous clusters,and this approach easily accommodates random missing data [24].The number of classes was determined by the lowest Bayesian information criteria (BIC) value and clinical meaning of each trajectory.A sensitivity analysis was conducted using corrected WFA from 2–36 months of age.
Mothers and their offspring were divided into three groups based on the offspring growth trajectories.Maternal and offspring characteristics were compared across groups.One-way analysis of variance (ANOVA) was used for continuous data conforming to a normal distribution,and the Kruskal–Wallis test was used for continuous data without a normal distribution.Chi-square analysis was used for categorical data,and Fisher’s exact test was used when an expected value was less than five in any cell.
Maternal factors affecting offspring weight trajectories were evaluated using the multivariable logistic model.The odds ratio (OR) for insufficient and excessive catchup growth was calculated with adjustment for other factors in the model,including maternal height,pre-pregnancy BMI,total GWG,GWG rate,TC,and LDL-C in the first trimester (T1).The factors were selected based on results from uni-variable analysis.Considering the multicollinearity between total GWG and GWG rate and TC and LDL-C at T1,the above pairs of variables were not included in the model simultaneously.Total GWG and TC in T1 were selected as adjustment factors.These maternal factors were then categorized into quintiles,and the chi-square for trend was used to compare the incidence of different offspring growth patterns throughout quintiles.Sensitivity analyses were also performed according to the corrected weight trajectories and stratified by chorionicity.
Results
Catch-up growth trajectories of the twin children from birth to 36 months
The original cohort recruited 63,998 pregnant women,2083 of whom had twin pregnancies.Thirty women with stillbirths,miscarriages,or neonatal death in one or both offspring and 482 women without offspring anthropometric data were excluded,leaving a final dataset including 3142 live births from 1571 mothers (Supplementary Fig.1).The average follow-up time was 34.8 months.

Fig.1 Twin offspring weight-for-age trajectories from birth to 36 months of age
A total of five latent weight classes were identified from the 3142 live twin births.Latent class one included 4.9% (154/3142) of the offspring who exhibited insufficient catch-up growth.Latent class two and three included 30.6% (961/3142) and 46.8% (1469/3142) of the offspring who showed adequate catch-up growth from diverse birth weights.Latent class four and five included 15.0%(472/3142) and 2.7% (86/3142) of the offspring who experienced varying degrees of excessive catch-up growth,respectively (Fig.1 a).As shown in Fig.1 a,all twin children from the five classes showed rapid catch-up growth to different degrees within six months from birth and then plateaued until 36 months.Sensitivity analysis using corrected WFA to adjust for gestational age showed similar offspring weight grouping results,except for the changed number of participants in each group (Fig.1 b).
Maternal factors during pregnancy associated with twin offspring growth
To examine maternal factors during pregnancy associated with the latent weight classes of the twin offspring,we classified the mothers according to the offspring weight classes into three groups: women with either or both offspring who exhibited an insufficient catch-up growth trajectory (latent class one) into Group 1;women with both offspring who exhibited an adequate growth trajectory (latent Classes Two and Three) into Group 2;and women with either or both offspring who exhibited an excessive catch-up growth trajectory (Latent Class four and five) into Group 3 (Table 1).Five women with one child who showed insufficient catchup growth and one who showed excessive catch-up growth were excluded from further analysis.As shown in Table 1,the three groups differed in maternal anthropometrics,including height,pre-pregnancy BMI,total GWG,and GWG rate.Incidences of TTTS,preterm delivery,cesarean section,and TC and LDL-C in the first trimester (T1) also differed across groups.No difference in the distribution of growth trajectories was observed between monochorionic and dichorionic twins.Table 2 indicates that neonatal asphyxia,birth weight and length were significantly associated with offspring growth patterns.The three weight groups showed divergent weights and lengths/heights throughout infancy and early childhood (Fig.2).

Table 1 Maternal characteristics categorized by offspring weight trajectory

Table 2 Offspring characteristics categorized by growth trajectories

Fig.2 The body weights and lengths/heights of the twin offspring stratified by growth trajectories
The results from the multivariable analysis suggested that short maternal stature and lower total GWG were associated with insufficient catch-up offspring growth.In contrast,maternal height,pre-pregnancy BMI,total GWG,GWG rate,TC and LDL-C in T1 were positively associated with excessive catch-up growth of the offspring.After correcting for gestational age,the negative association between maternal height and insufficient catch-up growth of the offspring and the positive association of the anthropometric measurements and lipid profiles with excessive offspring growth remained significant (Table 3).Further results from Fig.3 support the findings above by examining the trend of offspring growth patterns throughout the quintiles of the maternal factors.The proportions of offspring with insufficient catch-up growth decreased with maternal height,and the proportions of offspring with excessive catch-up growth increased with prepregnancy BMI,maternal height,GWG,TC and LDL-C in T1 (Pfor trend <0.05).In further analysis stratified by chorionicity,monochorionic twins and dichorionic twins showed different associations of maternal factors with postnatal growth.Only maternal height was associated with excessive catch-up growth in monochorionic twins,while all the aforementioned maternal factors were associated with excess growth in dichorionic twins (Table 4).

Table 3 Maternal factors associated with offspring catch-up growth trajectories by multivariate analysis

Table 4 Maternal factors associated with offspring catch-up growth trajectories in monochorionic and dichorionic twins
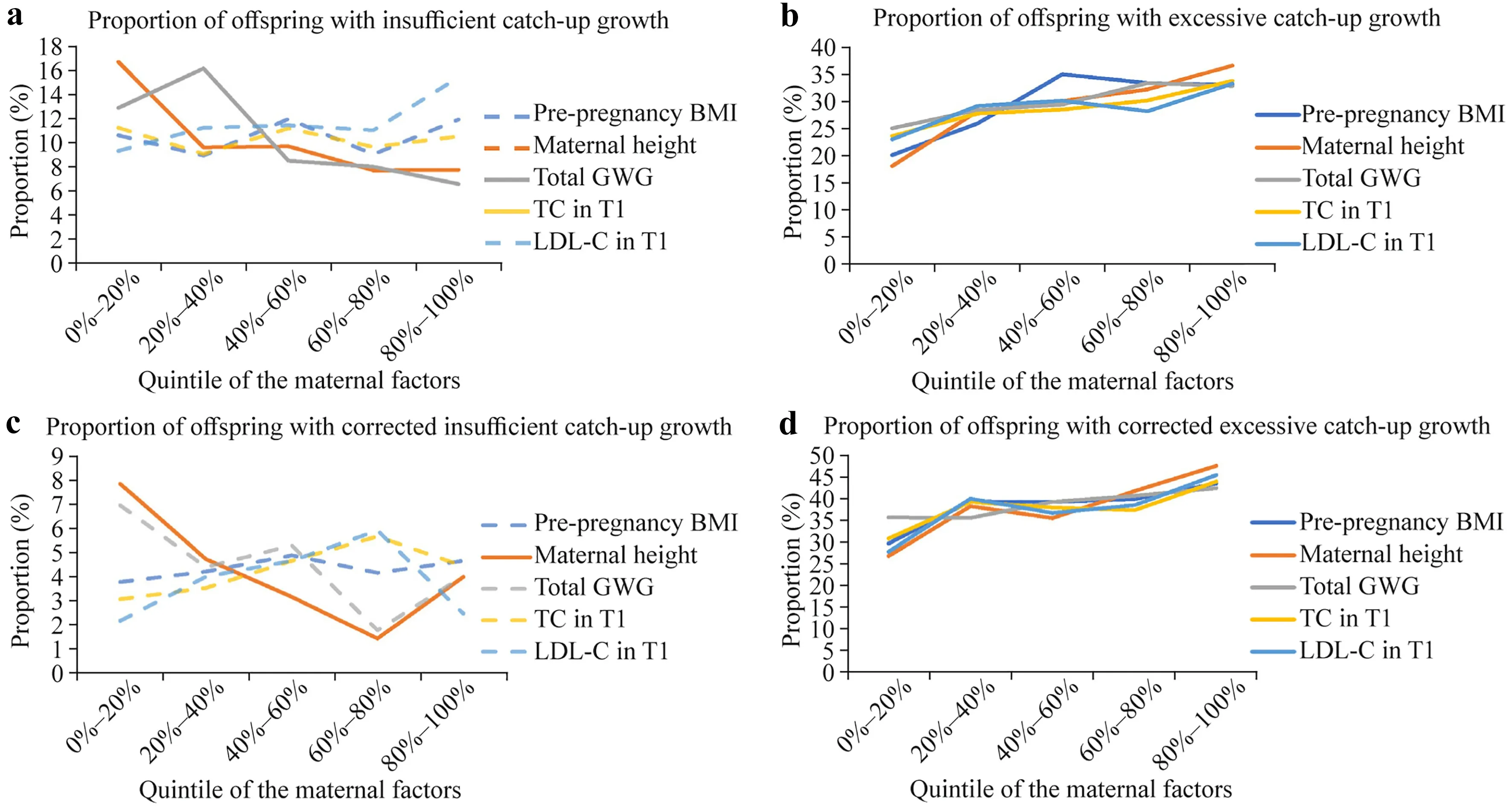
Fig.3 Trends of offspring with insufficient and excessive catch-up growth by maternal factor quintile.The solid lines indicate significant trends across the quintiles (P for trend <0.05).GWG gestational weight gain,TC total cholesterol,T1 the first trimester,LDL-C lowdensity lipoprotein-cholesterol
Discussion
This study portrayed different catch-up growth patterns of twin children and explored associated maternal factors during pregnancy,thereby providing evidence for multifetal gestation management.Five latent weight trajectories of twin children from birth to 36 months of age were identified and classified as insufficient,adequate,and excessive catch-up growth.Short maternal stature and lower weight gain in pregnancy were associated with insufficient catchup growth.In contrast,higher maternal stature,higher prepregnancy BMI and GWG,and elevated levels of TC and LDL-C in early pregnancy were associated with excessive catch-up growth of the offspring.
Catch-up growth is a ubiquitous compensatory mechanism for infants born preterm or LBW [10–12].Although it is well recognized that twin children constitute a substantial part of preterm birth and LBW [1,3],studies investigating the catch-up growth patterns of twin children are limited.This study first depicted disparate catch-up growth curves of twin children using WFA as the indicator by WHO criteria.This is because the length-based index of infants and young children is less reliable than the weight-based index due to measurement difficulties.Despite the discordant results regarding catch-up growth in singleton children [16,25,26],this study showed that most twin children reached adequate WFA SD-scores at 36 months of age,with a minority ending with insufficient or excessive growth.By analyzing the dynamics of the WFA SD score during the early life stage,we found that all five latent weight trajectories of twin children reached an SD score plateau after significant catch-up growth within six months of birth.These growth patterns concord with previous reports that critical postnatal catch-up growth occurs during the first year of life in singleton infants [27].
Catch-up growth of preterm and LBW neonates in the early life stage is critical for long-term health [10,12,28–31].Failing to catch up in weight or length usually indicates undernutrition and poor physical and neural development [10,12].In contrast,excessive catch-up growth raises serious concerns about the metabolic health of the offspring in adulthood [28,29].Compelling evidence has indicated that excessive catch-up growth often implies “catch-up fat”,meaning a disproportionately higher rate of body fat deposition than lean mass [30,31].The “catch-up fat” phenomenon is primarily driven by the adapted thrifty energy metabolism,during which glucose spared from oxidation in skeletal muscle is redirected toward de novo lipogenesis and fat storage in white adipose tissue [30,31],resulting in insulin resistance and an elevated risk of metabolic syndrome [28,29].
This study explored maternal factors during pregnancy that were associated with offspring growth patterns.We found that maternal stature and GWG were associated with offspring catch-up growth,indicating genetic and nutritional influences on children’s growth.Consistently,previous studies regarding singleton pregnancies also demonstrated that maternal height was a strong determinant for offspring catchup growth [32,33].Severe pregnancy complications and neonatal morbidities such as TTTS and neonatal asphyxia may impair the catch-up growth of the offspring but were not further evaluated due to their low incidences.According to the DOHaD theory,the intrauterine environment has long-lasting effects on offspring health [18].In this study,we obtained similar results in twin gestations as in singleton pregnancy: maternal pre-pregnancy BMI,GWG,TC and LDL-C in early pregnancy were positively associated with excessive catch-up growth in twin offspring [34–37].Maternal obesity is accompanied by metabolic changes in glucose and fatty acids and placental dysfunction that may regulate“fetal programming” and perpetuate the intergenerational transmission of overweight and obesity [38,39].Epigenetic modifications of the offspring may result in alterations in gene function and exert long-term health impacts without any change to the DNA sequence itself [38,39].
However,in this study,we did not find an association between maternal glucose level and offspring growth,which is divergent from previous reports on singleton pregnancies[40,41].Whether there is an association between glucose level in pregnancy and neonatal birth weight in twin pregnancies remains controversial [42–44].It has been proposed that GDM does not increase the risk of macrosomia in twin pregnancies due to the increased utilization of serum glucose in the presence of two fetuses [43,44].This study further evaluated the glucose level throughout pregnancy with twin offspring growth in infancy and early childhood and obtained negative results.
The growth trajectories were similar between monochorionic and dichorionic twins,consistent with previous reports[45].We further compared the maternal factors associated with catch-up growth in monochorionic and dichorionic twins.Maternal stature was the only predictor for catch-up growth in monochorionic twins,which was concordant with the previous reference that anthropometrics of monochorionic twins were mainly determined by the height of the parents [46].In contrast,maternal height,pre-pregnancy BMI,GWG,TC and LDL-C in early pregnancy were all associated with excess growth in dichorionic twins,similar to results from singleton pregnancies [34–37].The disparities in the risk factors for twin offspring growth with different chorionicities have pinpointed future directions for maternal and child care and research.
Strengths and limitations
This study verified the association between maternal anthropometrics and lipid profiles with offspring growth trajectories in twin pregnancies for the first time.Efforts have been made to clarify the effect of maternal weight on neonatal and childhood outcomes in twin pregnancies [47,48].However,weight only represents a single aspect of maternal health in pregnancy.This study comprehensively evaluated maternal pre-pregnancy weight,GWG,glucose and lipid levels,and maternal complications.Additionally,this study went a step further using the weight trajectories of twin children as primary outcomes,thereby making a more comprehensive assessment of child growth and providing converging evidence for improving twin pregnancy management together with previous findings [47,48].
However,there are certain limitations that need to be addressed.This study investigated offspring growth trajectories across infancy and early childhood,which may raise the concern that postnatal factors such as infant feeding practices may confound the study results.It has been reported that childhood obesity is less frequent among those who were exclusively breastfed for at least six months [49].This study did not find an association between infant feeding patterns and growth trajectories.However,this may be because the investigation was not sufficiently detailed or there were too many missing values.In addition,although as many relevant maternal and neonatal characteristics were collected as possible,some potential confounding factors,such as twin zygosity and maternal social status,were unavailable.
The intrauterine environment is critical for both shortterm and long-term offspring health.Previous studies have demonstrated that maternal factors are associated with perinatal outcomes in twin pregnancies [3,47].However,evidence regarding longer-term growth in twin offspring is limited.Our study revealed that maternal factors during twin pregnancy were associated with insufficient and excessive offspring growth trajectories in infancy and early childhood.Previous studies have mainly focused on intrauterine growth restriction and LBW in twin gestation.In contrast,a recent study by Bodnar et al.has raised general concern about the high prevalence of overweight and obesity in twin children[48].Our results suggest that inappropriate GWG and elevated blood lipid levels in twin pregnancies may inadvertently contribute to longer-term child obesity in dichorionic twins.
In conclusion,this study identified insufficient,adequate,and excessive classes of catch-up growth trajectories of twin children and pinpointed short maternal stature and lower maternal GWG as risk factors for insufficient offspring growth and higher pre-pregnancy BMI,excessive GWG,and elevated blood lipid levels in early pregnancy as risk factors for excessive offspring growth.These findings,along with previous studies evaluating maternal factors and perinatal outcomes in twin pregnancies,have provided evidence for improving twin pregnancy management.Nevertheless,further research is needed to confirm the findings,taking into account the underlying confounding factors during the relatively long time span.
Supplementary InformationThe online version contains supplementary material available at https:// doi.org/ 10.1007/ s12519-0 23-00703-z.
AcknowledgementsWe thank the participants for their contribution to the study and the medical stafffor collecting clinical information and blood samples.
Author contributionsZW: conceptualization,formal analysis,funding acquisition,methodology,writing–original draft;ZKS: data curation,investigation,writing–review and editing;YXX: methodology,validation,writing–review &editing;LJY: data curation,investigation;WJ:data curation,investigation;SW: data curation,investigation;LSN:data curation,investigation;WXX: data curation,investigation;GCM:data curation,investigation;LGH: funding acquisition,project administration,resources,writing–review and editing.
FundingThis work was supported by the Scientific Research Common Program of Beijing Municipal Commission of Education(KM202110025007),the National Natural Science Foundation of China (82171671),the National Key Research and Development(2016YFC1000304),and Beijing Hospitals Authority’ Ascent Plan(DFL20191402).
Data availabilityThe dataset is available upon reasonable request to the corresponding author.
Declarations
Conflict of interestNo financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article.
Ethical approvalThe study was approved by the ethics committee of Beijing Obstetrics and Gynecology Hospital,Capital Medical University (2018-ky-009-01),and written informed consent were obtained from all the participants or their legal guardian.
杂志排行

World Journal of Pediatrics的其它文章
- Sepsis heterogeneity
- How are children with medical complexity being identified in epidemiological studies? A systematic review
- Consensus for criteria of running a pediatric inflammatory bowel disease center using a modified Delphi approach
- Effectiveness of BNT162b2 and CoronaVac vaccines against omicron in children aged 5 to 11 years
- Association between maternal gestational diabetes and allergic diseases in offspring: a birth cohort study
- Determinants of infant behavior and growth in breastfed late preterm and early term infants: a secondary data analysis