Risk estimation of chronic kidney disease in a leptospirosis endemic area: A casecontrol study from south Andaman Islands of India
2023-11-17AmbreenFatemaManjunathaRamuPaluruVijayachari
Ambreen Fatema,Manjunatha Ramu,Paluru Vijayachari
ICMR- Regional Medical Research Centre, Port Blair, Post Bag No. 13, Dollygunj, Port Blair 744101, Andaman &Nicobar Islands, India
ABSTRACT Objective:To estimate the risk of chronic kidney disease in patients with leptospirosis.Methods:All reported (41 890) and later confirmed leptospirosis(1 990) cases from 2010-2020 were traced by universal sampling.386 Laboratory-confirmed leptospirosis cases were enrolled and 413 age,gender,area,and occupation matched healthy persons were included as controls.Variables including socio-demographic characteristics,medical history,and health-related behaviours were compared between the two groups and association between these variables and reduced estimated glomerular filtration rate (eGFR)was analyzed with multiple linear regression.Results:The median of eGFR was 49.0 (27.0,75.0) mL/min/1.73 m2 in the cases and 96.0 (72.0,121.0) mL/min/1.73 m2 in the controls,showing significant differences (P<0.001).Bivariate analysis showed that leptospirosis seropositivitiy,repeat leptospirosis infection,diabetes,male gender,working in field (sun exposure),COVID-19 infection and smoking had statistically significant association with reduced eGFR.Leptospirosis seropositivity had negative effects on eGFR.Multiple linear regression confirmed that leptospirosis seropositivity had negative effects on eGFR (unstandardised β coefficients=-30.86,95% CI -49.7 to -11.9,P<0.001).Conclusions: Chronic kidney disease is a complex disease with multiple risk factors involved.Exposure to leptospirosis is one of the essential factors in accelerating its progression.
KEYWORDS: Chronic kidney disease;Endemic leptospirosis;Estimated glomerular filtration rate (eGFR)
1.Introduction
A longer than three-month occurrence of structural or functional abnormalities of the kidney,with GFR<60 mL/min/1.73 m2,with or without kidney damage,is referred to as Chronic Kidney Disease(CKD)[1].Globally,the prevalence of CKD is estimated to be 8%–16%[2];there were 697 million cases of CKD worldwide in 2017,and nearly one-third of these patients lived in China (132 million cases) and India (115 million cases).CKD caused 1.2 million deaths worldwide in 2017.Globally kidney dysfunction contributed to an additional 1.4 million cardiovascular disease deaths.CKD was the 17th most common cause of global mortality in 1990,but its significance has grown over time,and it was the 12th most common cause of death in 2017[3].The report on the global burden of CKD shows that the growth rate has lagged behind HIV/AIDS[4].Kidney Disease Improving Global Outcomes (KDIGO) categorises the CKD severity into the following stages based on estimated glomerular filtration rate (eGFR) values to expedite the assessment[5].Stage 1:normal eGFR≥90 mL/min per 1.73 m2,stage 2: eGFR between 60 to 89 mL/min per 1.73 m2,stage 3: eGFR between 30 to 59 mL/min per 1.73 m2,stage 4: eGFR between 15 to 29 mL/min per 1.73 m2and stage 5: eGFR of <15 mL/min per 1.73 m2or end-stage renal disease.Classification based on proteinuria level ranges from A1-A3 (albumin: creatinine ratio),where Albuminuria stage 1 refers to:normal to mildly increased <30 mg/g to <3 mg/mmol,Albuminuria stage 2: moderately increased mmol 30-300 mg/g to 3-30 mg/mmol and Albuminuria stage 3: severely increased >300 mg/g to >30 mg/mmol[5].
According to a recent report from India,the prevalence of CKD was 13.00%–15.04%,with stages 1,2,and 3 being 6.62%,5.40%,and 3.02%,respectively.Results are consistent with data from the US National Health and Nutrition Examination Survey,indicating that the status in India is similar to that in the Western world[6].CKD due to traditional risk factors is well established[7,8],but another severe form of CKD is with an absence of traditional risk factors such as hypertension,diabetes,coronary artery disease,or senescence,toxins,pesticides,heavy metals,silica,hantavirus infections,Nonsteroidal Antiinflammatory Drugs (NSAIDs),smoking,phosphate and sugarsweetened beverages,illicit liquor,aristolochic acid,and herbal treatments[9],features progressive renal failure,which is frequently detected at a relatively late stage due to the lack of early signs[10].The patients may occasionally arrive with CKD of unknown risk factors,or undetermined aetiology (CKDu)[9,11].
Leptospirosis is a zoonotic disease[12],it has two phases: the immunological (delayed) and leptospiremic (acute) phases.Leptospiremia means leptospires in blood,it is that contact betweenLeptospiraand the immune system in blood and other organs that leads to the immune phase,with the pathogen most concentrated in the proximal renal tubules of the kidneys[13].Kidney biopsy on meat industry workers affected withLeptospira(L.)pomonainfections suggests renal lesions can be immunologically mediated;acute renal failure is primarily caused by acute interstitial nephritis and tubular necrosis[14].Leptospirosis has been linked with the soaring prevalence and CKD severity,a sustained decline in renal function over time,particularly in cases with tenacious high Microscopic Agglutination Test (MAT) titre levels[15].
Andaman and Nicobar is an Indian territory situated in the Bay of Bengal as a remote group with limited medical facilities.The archipelago has been endemic to leptospirosis for decades;hence,the chronic sequelae of the disease concerning renal damage are highly significant for better public health management.CKD has become a global burden,so knowledge regarding the association between CKD and leptospirosis has become essential.
2.Subjects and methods
2.1. Study design
A case-control study,with universal sampling,all reported cases(total of 41 890) and later confirmed leptospirosis cases (total of 1 990) from the year 2010 to 2020 were included in the study.Samples are received at Regional Medical Research Centre (RMRC)for leptospirosis diagnosis as it is a WHO reference centre for leptospirosis diagnosis and research.Leptospirosis suspicion in the acute stage was made based on the febrile illness of sudden onset,headache,and body aches,related to any of the following symptoms:1) calf muscle tenderness,2) bleeding tendencies,including subconjunctival haemorrhage,3) cough,hemoptysis,breathlessness,4)jaundice and 5) oliguria[16].
Leptospirosis confirmation was by any one of the following methods: 1) IgM ELISA;2) RTPCR;3) MAT titre of 1 400 in single;4) Fourfold rise in titre or seroconversion in paired sera[17].From 12/07/2021 to 24/01/2022 (6 months,12 days) single time follow-up of leptospirosis confirmed cases was done by multiple camps held at Ferrargung hospital,Tushnabad in Ograbraj community hall,three different locationsviz: Guptapara,Manglutan,Wandoor community hall and Chouldari Hospital for data and sample collection.Observer bias was controlled by single blinding where the sample/data collector was unknown about the serostatus of the patients.After considering inclusion and exclusion criteria,386 cases and 416 control were enrolled in the study,as shown in Figure 1.The caseto-control matching was done based on similar age,gender,and area(possibly in the same house,neighbour or same study area).A caseto-control ratio of 1:1 was followed[18].
2.2. Study area
South Andaman district of the Andaman and Nicobar Islands,India,is an archipelago in the Bay of Bengal that stretches over 700 kilometres from north to south and lies between longitude 92 º°and 94 º° East and latitude 6 º° and 14 º° North.The south Andaman district has a population of 238 142[19].
2.3. Inclusion and exclusion criteria
All laboratory-confirmed cases with leptospirosis were enrolled and age,gender,area,and occupation matched healthy persons were included as control.But cases already diagnosed with kidney disease with other aetiology were excluded.
2.4. Independent variable
Association of independent variables such as age (at enrolment)[20],sex[21],place of residence[22],diet high in sodium of more than or equal to 2.5 g/day[23],smoking of 1-4 or more cigrattes/day for six months or more[24],chronic excessive consumption of absolute alcohol of more than 30 g per day[25],analgesics abuse of persistent or sporadic excessive drug use with inconsistent dose[26],obesity if BMI greater than or equal to 30 kg/m2[27],hot temperatures and humidity[28] and sources of water consumption[11] were studied along with outcome variable.
Co-morbid conditions: Association of co-morbid conditions including type 2 diabetes[8],hypertension[7],hyperuricemia[29],chronic urinary tract disease[30],known kidney diseases were studied along with outcome variable.Outcome variable: CKD based on eGFR values based on the CKD-EPI equation.
2.5. Medical measurements and laboratory testing
All subjects were asked to gather at their nearest community centres or hospital conference rooms.After a 10 minute rest period,the participant's blood pressure was assessed using a calibrated digital sphygmomanometer (Omron HEM 7120).Participants were categorized as those with hypertension (systolic BP≥140 mm Hg or diastolic BP≥90 mm Hg) and those with hypotension (systolic BP≤90 mm Hg or diastolic BP≤60 mm Hg).We measured blood glucose levels (Accu-check Active) using a finger prick method[31].Patients were classified if their blood glucose level ≥126 mg/dL after fasting or ≥200 mg/dL if the participant had not fasted were termed diabetes[32].Height was determined using a foldable stadiometer,and weight was determined using a calibrated digital flat mobile scale.Certified Technical Staff of RMRC collected blood samples in Becton Dickinson (BD) gold cap vacuum tubes for centrifugation and serum separation.The cold chain was maintained throughout the processing.Blood samples were separated into serum and processed for creatinine on the collection day.Samples were stored at–20 ℃.The following day,other biochemical tests were performed and samples were frozen at -80°℃.The tests were performed at RMRC on a semi-automatic biochemistry analyser,Transasia,Erba Mannheim Model: CHEM-7.Calibration of equipment and kits was done during pilot testing as per standards.
2.6. Biomarker test
For diagnosing the extent of damage to the respective organ,biomarker tests were carried out.The Siemens kit (autopak) was used for testing,sample condition,sample preference,reference values and kits standardisation;sample volumes were per respective biomarker test kits.To determine the eGFR (estimated Glomerular Filtration Rate),CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equation was used[33].
2.7. Leptospira serology
MAT,a gold standard anti-leptospiral antibody detection and confirmation test was used[17].Serum samples were examined for anti-leptospiral antibodies in accordance with the standardised procedure[34],utilising a panel of 17Leptospirareference strains and a local isolate.Representing serogroups are Autumnalis (BangkinangⅠ),Australis (Ballico),Grippotyphosa (Moskva Ⅴ),Grippotyphosa(CH 31),Canicola (Utrecht Ⅳ),Icterohaemorrhagiae (RGA),Icterohaemorrhagiae (AF61),Sejroe (Hardjoprajitno),Pomona(Pomona),Hebdomadis (Hebdomadis),Pyrogenes (Salinem),Louisiana (LSU 1945),Celledoni (Cellodoni),Cynopteri (3522 C),Dejasiman (Dejasinman),Tarassovi (Perepelicin) and Semaranga(Patoc 1).The live antigens were cultured in liquid McCullough Johnson Harris (EMJH) medium for 5-7 days,and 0.5 McFarland standard concentration was adjusted.MAT was carried out using doubling dilutions beginning at 1 in 50.Positive specimens were titrated up to end titres.The highest dilution that caused at least a 50% reduction in cells or agglutination was reported as the endpoint titre.The inverse of the quantity of dilutions still exhibiting 50%live bacterial antigen agglutination was used to calculate MAT titres.Cases with a MAT titre of 1: 100 indicating prior exposure were classified as seropositive and enrolled in study[13].Cases and control samples were processed in uniform conditions.
2.8. Statistical analysis
The Statistical Package for Social Sciences (SPSS) was used to evaluate the data,version 28.0 (SPSS Inc.,Chicago,IL,USA).Proportions of total subjects on leptospirosis were calculated and presented as frequencies (%).The association between two categorical variables was analysed by the χ2test and Fisher’s exact test for cell count of less than 5.At the 95% confidence level (CI),less than 0.05P-value was regarded as statistically significant,and multiple linear regression was done by considering eGFR as the dependent variable.Median (IQR) is considered where the distribution was skewed and with outliers.All statistical tests were applied as per standard protocol.
3.Results
A total of 386 cases and 416 controls were selected.The mean age of the cases was (41.0±14.4) years,while for the controls it was (40.7±14.4) years.Among the cases,362 (93.8%) participants were from rural areas,only 24 (6.2%) were urban residents.Rural residents were more likely to aquire leptospirosis infection than corresponding urban residetnsts (χ2=39.027,P<0.001).Working in field is significantly (χ2=131.698,P<0.001) associated with cases(250,64.7%).A total of 212 cases (54.9%) use own tap as the source of drinking water suggesting subjects with their own tap as a drinking water source were less likely to get leptospirosis infection(P<0.05) presented in Table 1.
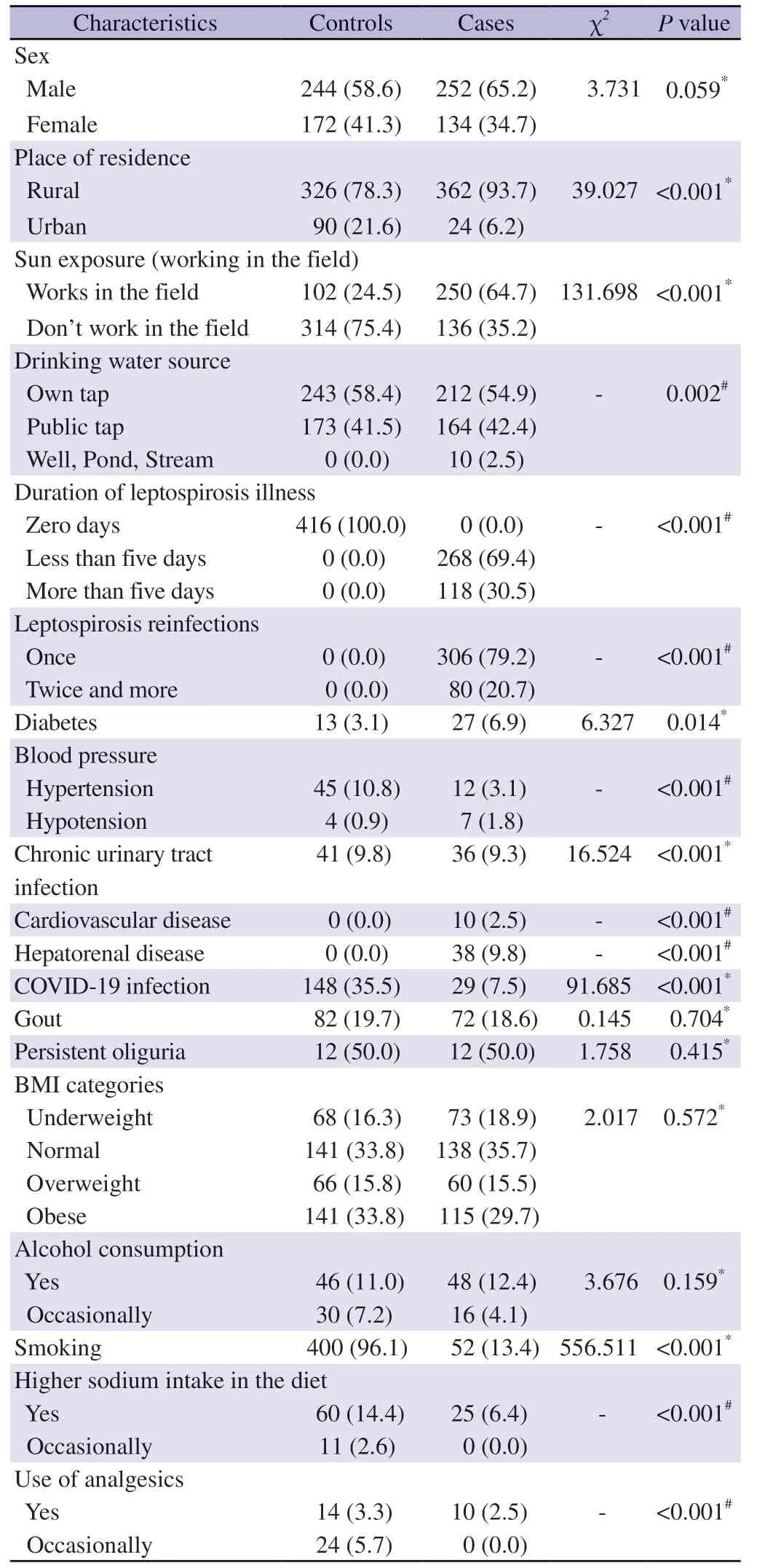
Table 1.Comparison of socio-demographic characteristics,medical history and health-related behaviours between the two groups [n (%)].
The duration of less than five days of leptospirosis illness was experienced by 268 (69.4%),and more than five days were experienced by 118 (30.5%) for the cases.Eighty cases (20.7%)experienced repeat leptospirosis infection (twice and more),is statistically significant.Significant differences in diabetes,hypertension,COVID-19 infection,cardiovascular disease,and other factors are noted as shown in Table 1.
In contrast,among the control group,326 (78.4%) were rural,and 90 (21.6%) were urban residents.The controls were more in obese category 141 (33.8%) followed by overweight category 66 (15.8%)than cases.Controls smoked significantly more (400,96.1%) but alcohol intake is less (46,11.0%) than the corresponding number of cases.More controls had source of drinking water as own tap 243(58.4%) as presented in Table 1.
We compared general and biochemical parameters of the study participants by median values.The cases had higher median creatinine values than the controls [cases: 1.6 (1.2,2.0) mg/dLvs.control: 0.9 (0.7,1.1) mg/dL,P<0.001].Overall cases had lower median range of eGFR than the controls [cases: 49.0 (27.0,75.0) mL/min/1.73 m2vs.control: 96.0 (72.0,121.0) mL/min/1.73 m2,P<0.001].Differences in albumin levels [cases: 4.4 (2.8,5.9) g/dLvs.control: 3.1(2.3,4.4) g/dL,P<0.001],along with height,serum glutamic-pyruvic transaminase (SGPT),serum glutamic-oxaloacetic transaminase(SGOT),urease and bilirubin leves were also significant.
In bivariate linear regression analysis,out of 19 variables only seven variables such as leptospirosis seropositivity,repeat leptospirosis infection,diabetes,male gender,working in field (sun exposure),COVID-19 infection and smoking has a statistical significant association with lower eGFR values as presented in Table 2.Multiple linear regression revealed that leptospirosis cases,male gender and diabetes mellitus had a significant association with the lower eGFR.The cases seropositive had unstandardised β coefficients of 30 lesspoints than controls (β coefficients=-30.86,95%CI-49.7 to -11.9,P<0.05) as shown in Table 2.Moreover,the overall adjustedR2=0.19 value depicts that the model explains 19% of the variance in the eGFR values as shown in Table 2.

Table 2.Bivariate and multivariate linear regression results on eGFR derived by CKD-EPI equation.
Among 386 cases,240 (79.9%) developed CKD whereas,in control,it is 61(20.3%).Cases had nine times higher odds of developing CKD (OR9.5,95%CI6.80 to -13.45,P<0.05).However,maximum cases were from stage 3b (28.75%),followed by stage 3a (22.02%),stage 2 (19.68%),stage 1 (19.17%) and stage 4 (10.36%) respectively.Cases had significantly greater proportions of CKD than controls,especially at stages 3b (28.75%vs.3.36%),stage 3a (22.02%vs.9.85%).
Confirmed leptospirosis cases from the past ten years were tracked and included in the study and then we have performed MAT to detect presence of anti-leptospiral antibodies in both cases and controls.Presence of single strains in the blood samples of the cases are in the proportions as Icterohaemorrhagiae (AF61) present in 64% cases,Australis (Ballico) was present in 15%,Grippotyphosa(CH 31) in 10%,Icterohaemorrhagiae (RGA) in 6%,Autumnalis(Bangkinang I) in 3%,Pyrogenes (Salinem) in 1% and Djasiman(Djasinman) in 1%.We have also observed mixed strains in MAT in which only strain with highest titre is mentioned in Table 3,where Icterohaemorrhagiae (AF61) was most predominant strain which was present even in one in more than 400 titre and the subjects were asyptomatic for leptospirosis.Few controls also showed titre but it was less than 1: 100.

Table 3.Presence of mixed strains of anti-leptospiral antibodies in chronic cases.
4.Discussion
This study aimed to estimate the relationship between leptospirosis(long endemic in the Andaman Islands) and CKD.The connection between Acute Kidney Injury (AKI) and leptospirosis is wellestablished[35].In the paediatric population,anicteric oliguric AKI caused by leptospirosis is more common and severe than nonoliguric kidney failure[36].About 50% of cases in adults develop renal complications[37].Fatalities happen when Acute Renal Failure (ARF) is present with jaundice[37].Patients with ARF after leptospirosis may experience non-oliguria and oliguria[38].
Renal biopsy has provided information on the histopathological characteristics of human leptospirosis.When a distinctive lesion is present,the distal convoluted and proximal tubules' lining cells are dilated and necrotic.In severe cases,lymphocytic infiltration,interstitial oedema,and tubulorrhexis are also present.Leptospirais concentrated around the tubules and in the tubular lumen,as shown by electron microscopy[14].Sitprijaet al.believed that extracellular fluid depletion caused acute renal failure in leptospirosis;nevertheless,the interstitial injury was listed as the most crucial element in a later paper[39].AKI can induce CKD,which often occurs if the condition seriously injures the kidneys[36].
Diabetes and high blood pressure are prominent CKD-associated factors[7,8].In our study,diabetes has shown a significant association with reduced eGFR.However,additional CKD cases unrelated to established causes have recently been observed among tropical agricultural workers[9].It is called chronic renal disease with unknown aetiology (CKDu)[40],hypertension[7],diabetes[8],and traditional factors such as glomerulonephritis are not linked to CKDu[11,15].Numerous causes have been put up,including agrochemicals and chronic low-dose exposure to certain heavy metals[40].Andaman and Nicobar Islands are dependent on the import of vegetables and fruits from mainland India which are often coated with preservatives/chemicals to extend shelf life.Hence,this factor also demands research in association with CKD.Kidney damage is also reported due to high sodium intake[23].Our findings suggest that subjects with higher sodium intake were more likely to get leptospirosis infection.In our study subjects with abuse of analgesics,and daily consumption of combinations comprising at least two antipyretic analgesics for years,typically mixed with caffeine/codeinehad higher chances of leptospirosis infection,link between leptospirosis and analgesic abuse was significant[26],but analgesic abuse was not significant in bivariate analysis with eGFR as the dependent variable.Other factors linked to CKD are hyperuricemia and hyperuricosuria[29],genetic susceptibility and obesity[27].In our study the subjects had BMI values in the normal range,as mentioned in Table 3.Hence,no statistical significance was observed with CKD.
Along with leptospirosis and Hantavirus infection,respiratory exposure to silica is linked with CKD,which can cause tubulointerstitial damage[40].Leptospirosis also is a potential factor for CKD[15].A study by Yanget al.suggests leptospirosis cases have lower mean eGFR values than the control group [cases: (98.3±0.4)mL/min per 1.73 m2vs.control: (100.8±0.6) mL/min per 1.73 m2,P<0.001)[15].Recent perspective study from Thailand proposes that severe leptospirosis is associated with long-term kidney sequelae[35].Another research by Riefkohlet al.demonstrated leptospirosis seropositive sugarcane workers had higher NGAL concentrations,possible indication of CKD[41].Our study’s multiple linear regression analysis indicated that leptospirosis seropositivity,male gender and diabetes mellitus were significantly associated with lower eGFR values.Multilinear regression with eGFR as the dependent variable suggests leptospirosis seropositivity had standardised (β coefficients=-0.31,95%CI-49.7 to -11.9,P<0.05),our study suggests there is a significant relationship between leptospiral infection and CKD.Women typically have less muscle mass than men resulting in lower creatinine levels[21].In our analysis,we found that women have lower mean eGFR values.
The climatic conditions of South Andaman are hot and humid,wherein annual minimum/maximum average temperature ranges between 22.1 ℃ to 32 ℃.Average annual sunshine hours vary from 250 h (December to April) to 113 h (September),and the relative average humidity is 80%[19].Along with the climatic conditions,particular occupations such as agriculture,fishing and other labourintensive jobs have prolonged exposure to the sun,which causes excessive sweating and dehydration.Further,dehydration leads to hyperosmolarity,leading to a rise in vasopressin,which quickens the course of CKD[36,42].Dehydration also causes the harmful side effects of hyperuricemia and rhabdomyolysis,which advance chronic tubulointerstitial illness[42].In our study,bivariate analysis of sun exposure on the eGFR equation resulted in a significant association with a unstandardised β coefficient of 12.58 (95%CI5.80 to 19.34,P<0.001),subjects who had more sun exposure had lower eGFR values.
There are limitations.Records of serum creatinine values before leptospirosis exposure were absent and periodical follow-up of cases and control was not feasible.Another limitation is that all the confirmed leptospirosis cases could not be included due to nontraceability,deaths and migration.
This is the first systematic study of chronic renal disease and its association with leptospirosis in the South Andaman slands involving cases from the last ten years.Evidence suggests that CKD is a complex disease with many factors involved.Repeated exposure to high leptospirosis titre is one of the essential factors in accelerating the progression of CKD.Practising preventive measures can reduce the morbidity and mortality linked to CKD.Many suggestions have been put forth concerning potential causes of CKD of unknown etiology,which are related to behaviours that can be modified by training in occupational health,safety and public health regulations.
Ethics statement
The local institutional human ethics committee meeting was held on 09/03/2021,in which the Proposal number 6-“Risk factors of leptospirosis and chronic sequelae: A followup study in an endemic area of South Andaman” had been approved.
Conflict of interest statement
We declare that we have no conflict of interest.
Funding
This study was finicially supported by ICMR SRF (Grant 2021-9539/F102).
Authors’contributions
All authors contributed to the interpretation of the results.All authors reviewed,edited,and approved the final version of the manuscript.AF conducted field visits,acquired data,experiments and manuscipt preparation.AF and MR performed the statistical analysis.PV designed,critically revised and supervised the research.
Acknowledgements
The authors acknowledge the help of Dr I.P.Sunish,Mr T.Kannan,Dr M.G.Madanan and Dr R.Parvez for their efficient guidance and overall inputs throughout the process and Mrs K.Saida for help in sample collection.
杂志排行
Asian Pacific Journal of Tropical Medicine的其它文章
- Malaria slide bank plays a crucial role in achieving and sustaining malaria elimination in India
- Insecticide resistance status of Aedes aegypti and Aedes albopictus in Malaysia (2010 to 2022): A review
- South Asian dairy smallholders: A scoping review of practices and zoonoses
- Impact of H1N1,H7N9,ASFV,dengue virus and COVID-19 on pharmaceutical manufacturing firms' R&D investments and economic consequences: Evidence from China
- Aeromonas hydrophila infection in acute myeloid leukemia: A case report
- Protection against symptomatic SARS-CoV-2 infection during the second wave among individuals with pre-existing binding antibodies to SARS-CoV-2: A population-based study from Puducherry,India