Comparison of anatomical and functional outcomes of different surgical techniques in myopic macular hole without retinal detachment
2023-10-21MerveOzbekSehnazOzcaliskanCengizAlagozOzgurArtunay
Merve Ozbek, Sehnaz Ozcaliskan, Cengiz Alagoz, Ozgur Artunay
Department of Ophthalmology, Beyoglu Eye Training and Research Hospital, Istanbul 34421, Türkiye
Abstract
● KEYWORDS: free internal limiting membrane patch graft; inverted internal limiting membrane flap; myopic macular hole; internal limiting membrane peeling
INTRODUCTION
Macular hole (MH) in highly myopic eyes can lead to significant central vision loss and increases the risk of complications such as retinal detachment (RD).The efficacy of surgical intervention and the visual outcomes are lower in high myopic MHs compared with non-myopic eyes[1].The occurrence of posterior staphyloma, the elongation of the axial length and epiretinal membrane formation render this surgery challenging and may elicit lower success rates.The inelasticity of the retinal blood vessels and internal limiting membrane(ILM) have also been considered to be an important factor in myopic MH surgery[2].
Several surgical methods have been defined to improve the outcomes of pars plana vitrectomy (PPV) and ILM peeling in the treatment of myopic, unclosed and large MHs, including free ILM patch transplantation and inverted ILM flap technique[3-4].Kuriyamaet al[5]reported that the inverted ILM flap procedure can be beneficial for the MHs with and without RD in high myopic eyes.They showed that closure rates would reach to 80%.Previously two studies compared the inverted ILM flap technique and the ILM peeling technique in MH patients with highly myopic eyes.The MH closure rates were higher in the inverted ILM group (100% and 91.7%) compared to the ILM peeling group (66.7% and 81.2%)[6-7].On the other hand, Morizaneet al[8]achieved successful results with autologous transplantation of ILM in patients with refractory MH.MH closure rate was 90% in their study.
However, there is little agreement among surgeons as to whether which procedure is superior, and treatment choice are frequently dependent on personal experience and preference.In this study, we purposed to assessed the anatomical and functional success of this approaches vitrectomy with ILM peeling, inverted ILM flap and free ILM patch graft technique for the treatment of myopic MH without RD.
SUBJECTS AND METHODS
Ethical ApprovalThe ethical clearance was obtained from the Hamidiye Ethics Committee of University of Health Sciences (Approval number 6/9).All authors adhered to the tenets of the Declaration of Helsinki.Informed consent had been obtained from all the participants.
This was a retrospective study consists of consecutive patients who underwent vitrectomy with inverted ILM flapprocedure,free ILM patch graft procedure or conventional ILM peeling for myopic MH without RD between January 2017 and May 2021, at a tertiary referral center.
The inclusion criteria were: 1) myopic MH without RD; 2)high myopia (defined as an axial length of at least 26 mm or a refractive error of -6.00 dioptres or more); 3) a followup period of more than 6mo from the surgery.The exclusion criteria were: 1) recurrent MH; 2) traumatic MH; 3) presence of systemic disease or chronic ocular disease.
All patients underwent detailed preoperative ophthalmologic examination, including best corrected visual acuity (BCVA)according to Snellen charts, measurement of axial length and dilated indirect and contact lens slit-lamp biomicroscopy,applanation tonometry and spectral domain optical coherence tomography (SD-OCT; Spectralis HRA OCT, Heidelberg Engineering, Heidelberg, Germany).The diagnosis of myopic MH was verified with SD-OCT.
在科学课上,学生对于科学世界的探索和理解,经常不是一个人去完成的,正如科学界的伟大发现,经常是一个团队共同努力的结晶。教师在教学过程中要让学生明白这样的道理,并且在合作学习过程中得到更多的成功喜悦之感。此外,教师要善于调动学生的积极性,让学生组成合作探究学习小组,让他们在合作学习的过程中够主动地发现问题,并且将问题在发挥小组成员各自优势的前提下高效解决。
At the follow-up visits, all ophthalmologic examinations including BCVA, dilated slit lamp biomicoscopy, applanation tonometry and SD-OCT were performed.Data from the final visit were used to determine the efficacy of the surgical technique.SD-OCT images were used to evaluate the anatomical recovery of myopic MH.Preoperative and final BCVA values were used to evaluate the functional recovery.
Closure of MH was identified by SD-OCT as the disappearance of the hole and no bare retina pigment epithelium exposed to the vitreous.Flat-open and elevated-open myopic MHs were noted as anatomical failure in this study.
All patients underwent 23 gauge 3-port PPV (Alcon Constellation®nAlcon Laboratories, Fort Worth, TX, USA).Core vitrectomy was performed posterior vitreous detachment was induced with the vitrectomy probe or soft silicone-tipped cannula.In this retrospective study, the surgical technique was chosen based on surgeons personal experience and preference.All surgeries were performed by two qualified surgeons(Ozcaliskan S and Artunay O).A mixture of brilliant blue G was applied over the macula to stain the ILM.In the group of ILM peeling, the ILM was removed for nearly two disk diameters around the MH.Basically the inverted ILM flap surgery was performed in accordance with the description of Michalewskaet al[3].
The ILM was peeled in a circular manner for about two disc diameters around the MH after the staining procedure.During the circumferential peeling, the ILM was not peeled offentirely from the macula but was left related to the rim of the MH.A segment of the peeled ILM, which was hanging in the vitreous cavity, placed over the MH.To stabilize the flap and facilitate the surgical maneuvers, the perfluorocarbon liquid was applied over the macula.Then the MH was covered with the inverted ILM flap.
In the free ILM patch group, the ILM was peeled off completely to the vascular arcades and then removed.Perfluorocarbon liquid was placed over the optic disc and macula.The free ILM flap of slightly wider than the size of the MH was harvested from the residual ILM close to the vascular arcades.Then the free flap was placed over the MH under perfluorocarbon liquid.The fluid-air exchange was performed.During this procedure, the remnant fluid on the disc was removed continuously to avoid movement of the free flap.At the end of the operation, the air was replaced with 12% perfluoropropane or 20% sulfur hexafluorid.Patients maintained face down position for 7d postoperatively.
Patients who underwent ILM peeling surgery comprised Group 1 (n=26); patients who underwent free ILM patch graft surgery comprised Group 2 (n=20) while patients treated with inverted ILM flap surgery comprised Group 3 (n=18).
The BCVA was assessed using Snellen charts and converted to the logarithm of the minimal angle of resolution (logMAR) for calculation.To define the surgical outcomes, the preoperative and postoperative BCVA (logMAR value) were compared using the pairedt-test.APvalue of less than 0.05 was considered significant.All statistical analyses were performed using SPSS for Windows version 22.0 (SPSS Inc., Chicago,Illinois, USA).Data were presented as mean±standard deviation (SD).
RESULTS
Sixty-four eyes of 64 consecutive patients (eighteen males and forty-six females) with myopic MHs were included in this study.The median age of the patients was 63.2±2.35y.On the SD-OCT examination at baseline, the base diameter of the MHs were 863.23±256.00 µm in the Group 1, 981.12±274.13 µm in the Group 2 and 1195.11±364.00 µm in the Group 3.Thirtyone eyes were phakic, and 33 eyes were pseudophakic.None of the eyes underwent phacoemulsification in combination with MH surgery.The follow up period was 20.11±7.24mo in Group 1, 17.11±6.52mo in Group 2 and 20.20±7.20mo in Group 3.The patient demographics and clinical features for the three groups are presented in Table 1.There was no significant difference in the baseline parameters between the three groups,including age, gender, axial lenght, length of follow up,preoperative BCVA and MH size.

Table 1 Preoperative characteristics of the patients mean±SD

Table 2 Comparison of visual and anatomic outcomes between three surgical methods mean±SD
The mean preoperative and postoperative BCVA was 1.60±0.53 logMAR and 1.27±0.58 logMAR, respectively.A significant increase was observed in the BCVA after the MH surgery (P<0.05).MH closure was obtained in 52 of 64 cases(81.25%).Anatomical success rates were 76.9% in the Group 1, 80% in the Group 2 and 88.9% in the Group 3.There was no statistically significant difference in the anatomical closure rates between the three groups (P=0.773; Table 2).
There were no complications during or after MH surgery in any patients.Late reopening of the MH was not observed in any patient during the follow-up period.Representative cases of the free ILM patch graft procedure and the inverted ILM flap procedure are presented in Figures 1 and 2.
Case 1Preoperative and postoperative scans of a 62-year-old woman with myopic MH.The BCVA was 1.80 logMAR and OCT scan demonstrated prominent retinoschisis around the MH.Primary PPV with the free ILM patch graft technique was performed.Six months after after surgery, the MH was closed and the BCVA was improved to 1.30 logMAR.
Case 2A 55-year-old woman was referred with a long standing MH (documented for at least 3y).Her BCVA was 1.30 logMAR preoperatively.The minimal MH diameter was 618 μm.Primary PPV with the inverted ILM flap procedure was performed.MH was closed and BCVA improved to 1.00 logMAR 3mo postoperatively.
DISCUSSION
In this study, we observed succesful anatomic and visual outcomes in myopic MHs using three different surgical tecniques.Our findings suggest that ILM peeling is an essential intervention in myopic MHs and flap techniques may offer higher postoperative closure rates in myopic MHs.
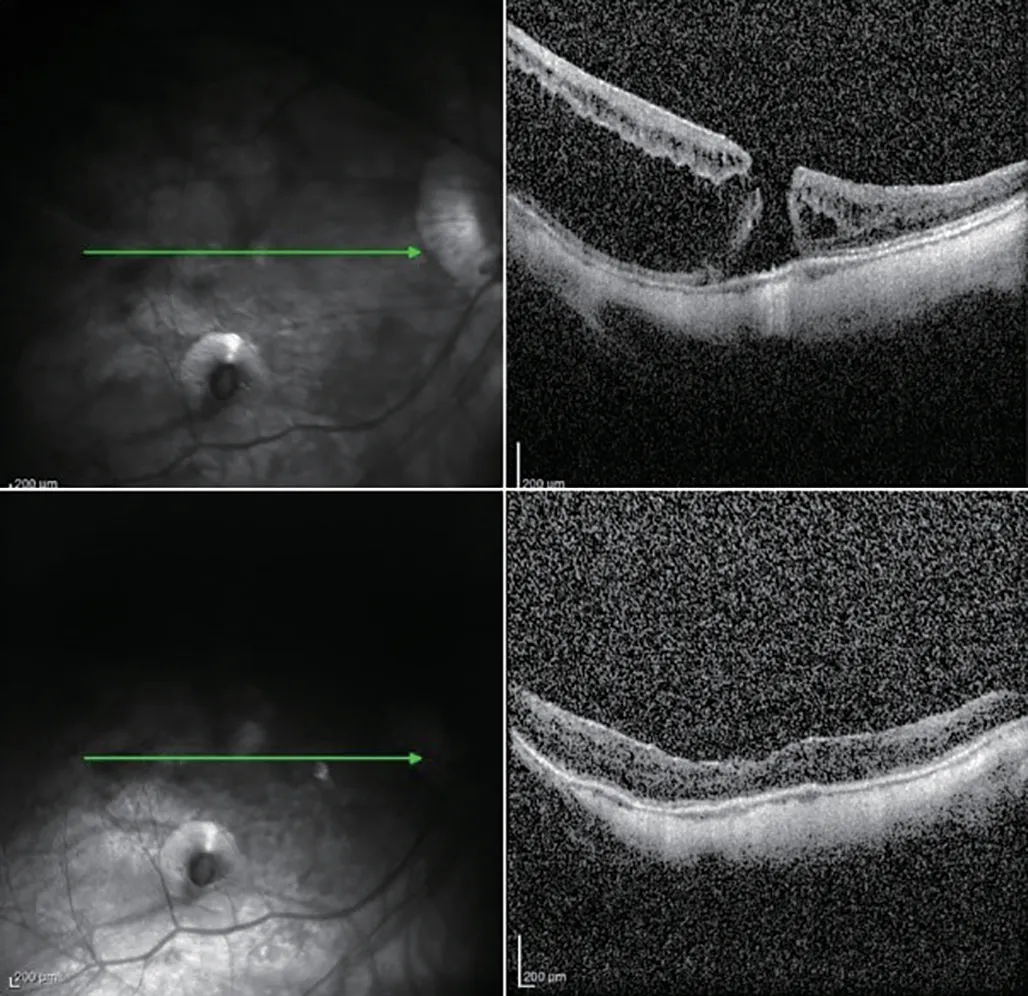
Figure 1 Spectral domain optical coherence tomography (SD-OCT)scans of macular hole (MH) with retinoschisis in high myopia A:Preoperative appearance; B: Postoperative appearance 6mo after pars plana vitrectomy (PPV) with the free internal limiting membrane(ILM) patch graftprocedure.
ILM peeling has been known as a crucial step in the surgical management of various retinal diseases, including MHs,vitreomacular traction, epiretinal membranes, macular edema and retinoschisis[9-10].ILM peeling in myopic MH have been widely adopted tecnique and accepted by the main part of retinal consultant as the primary treatment[5].It may ensure successful anatomical and functional outcomes by releasing the tangential traction attributed to the macula and reducing the risk of epiretinal membrane formation after surgery.However,recent studies revealed that ILM peeling may be insufficient for highly myopic MHs[5,9,11-12].
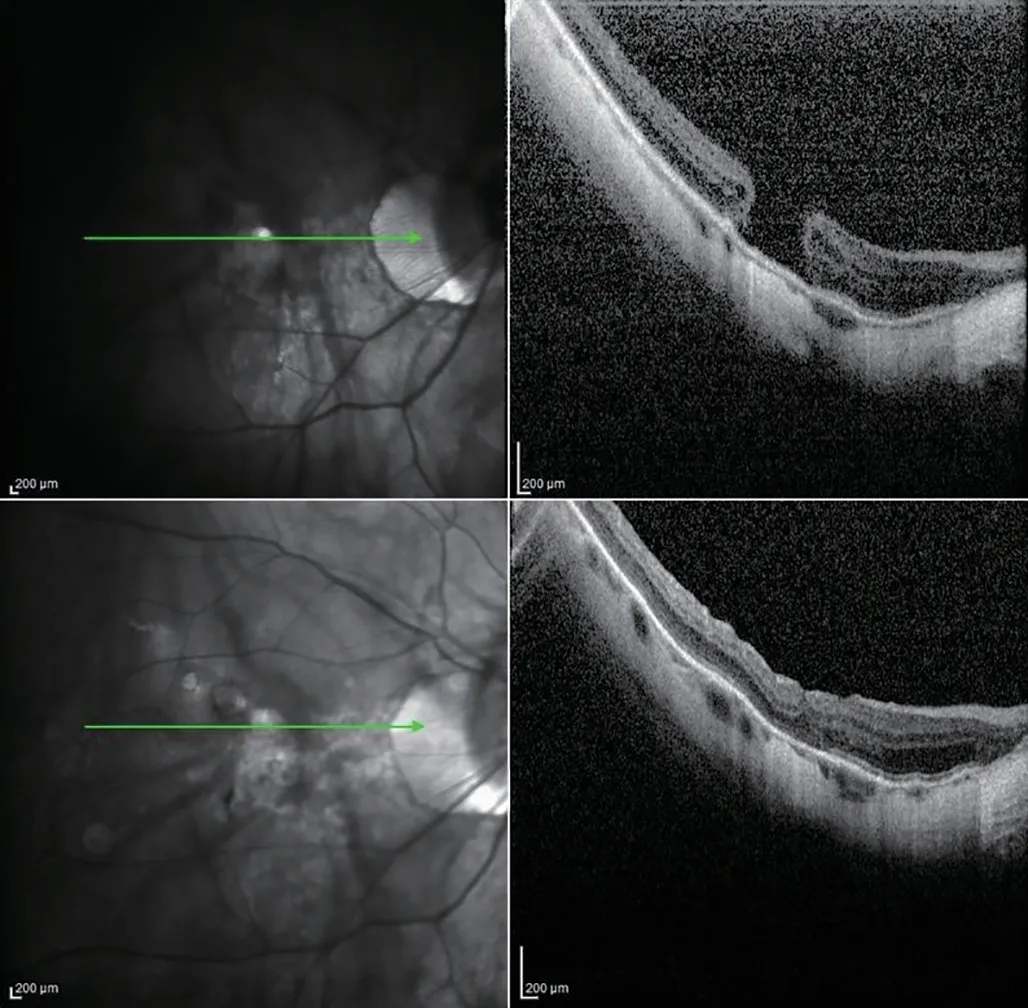
Figure 2 Spectral domain optical coherence tomography (SDOCT) scan of a high myopic full-thickness macular hole (MH) A:Preoperative image; B: Postoperative image 3mo after pars plana vitrectomy (PPV) with the inverted internal limiting membrane (ILM)flap procedure.
Kuriyamaet al[5]described the outcomes of a surgical intervention, named the inverted ILM flap procedure, for myopic MH surgery.They noted that the inverted ILM flap procedure can be advantageous for the MHs with or without RD in high myopic eyes.They showed that closure rates using the inverted ILM flap procedure would reach the success to 80%.Moreover, they achieved a progress in visual acuity scores more than 2 lines in 5 eyes (50%).
In another study, Huet al[6]compared the outcomes of the conventional ILM peeling technique and the inverted ILM flap technique for MH in eyes with high myopia.And observed better anatomic closure rates in the inverted ILM group (100%)compared to the ILM peeling group (66.7%).According to the study, inverted ILM flap technique offers superior structural recovery and visual improvement compared to the ILM peeling technique.
In a recent study, Wakabayashiet al[13]investigated the efficacy of vitrectomy with inverted ILM insertion for MH with RD in high myopia.They observed better closure rates in the inverted ILM group compared to the ILM peeling group (92%vs39%).In addition they achieved better postoperative functional outcomes in the inverted ILM group than the ILM peeling group.
In accordance with their findings, we observed higher closure rates with the inverted ILM flap tecnique compared to the other tecniques.Kuriyamaet al[5]suggested that the inverted ILM flap approach for filling the MH with proliferating cells could be superior to the ILM removal technique for relaxing the retina.
These aforementioned techniques may be an option for initial surgery, but the success rates are lower in eyes with refractory or recurrent MHs from which the ILM have already been peeled off.Morizaneet al[8]defined a new surgical approach, named autologous transplantation of the ILM.They transplanted an ILM flap inside the MH and obtained a significant BCVA increase in 8 eyes (80%) after a followup of 12mo in that study.They suggested that this technique may be a good option in eyes with refractory MHs.ILM peeling in highly myopic eyes requires advanced skills and add difficulty to the operation.During the peeling of ILM,there are two reasons for failure.These are the rupture of ILM or retina[14].In these cases, the inverted ILM flap procedure can not be caried out.In addition, the free ILM patch graft technique can be useful in patients who were operated surgery for macroaneurysm, myopic tractional maculopathy, diabetic macular edema and epiretinal membrane[15].
Chenet al[16]reported their concern about this technique.They argued that even with the ILM placement technique, there is a predisposition for the inverted flap to bend backwards.The recurrent manipulation within or around the MH can produce tissue injury and presumably limiting visual recovery.The most considerable point about the free ILM patch graft method is preserving proper location of the flap until the finalization of the fluid-air exchange or during the postoperative days.Minor changes to the original technique have been proposed to prevent the dislodgement of the flap and increase the anatomical success[17].Perfluorocarbon liquids may be used for free flap positioning, and autologous serum or viscoelastic plugs usage can improve tissue adhesion[15,18-19].
Müller cell proliferation and gliosis may perform a significant role in closing MHs and production a convenient conditions to the photoreceptors in new locations.Michalewskaet al[9]speculated that the ILM flap may induce gliosis on the surface of the ILM and inside the retina.The ILM also can be a scaffold for tissue growing and Müller cell proliferation.
Morizaneet al[8]showed that new tissue is formed surrounding the ILM flap after autologous ILM transplantation using OCT.In addition, Leeet al[20]demonstrated that autologous ILM flaps inside the holes stimulate prolonged glial proliferation.They showed that large MHs can be successfully closed as a result of this process.However, it is not known certainly how the ILM flap restores the fovea.
Previously several studies compared the anatomic and visual outcomes between ILM peeling and ILM flap insertion technique for MH in highly myopic eyes[21].In this study,we carried out a retrospective study aiming to compare the conventional 360 degree ILM peeling, the inverted flaptechnique and the free ILM patch graft.To the best of our knowledge, the current study is the first to compare these three techniques.We evaluated the functional success with improvement in BCVA and anatomical success was defined by MH closure rate.This study indicated that the free ILM patch graft and the inverted-flap technique has a slightly higher MH closure rate than the conventional 360 degree ILM peeling.In terms of MH closure rates of the inverted flap technique and the free-ILM patch graft, our outcomes seemed to resemble those published by now.Although the closure rates in the inverted ILM group and the free-ILM patch graft group was higher than that in the ILM peeling group.But significant differences in closure rates between the three groups were not found.In this study, no significant difference was found between the groups, between preoperative and postoperative BCVA.Severe chorioretinal atrophy and loss of foveal photoreceptor layer may be associated with this results.
The limitations of this study are that its retrospective desing and small sample size.We would like to specify that myopic MHs is extremely infrequent.Therefore, it is very difficult and time-consuming to conduct a randomized study.In this retrospective study, there was no difference in the MH base diameter.But we can see that the surgeon was tended to prefer free ILM patch graft or inverted ILM flap surgery in larger holes.This condition may lead to selection bias.Further studies are needed to define the impact of some additional factors, such as refractive errors, the presence of staphyloma,and the axial length.The relationship between BCVA and restoration of the ellipsoid zone and the external limiting membrane was not assessed.A longer follow-up time will be required to evaluate the long-term outcomes of this techniques on improving BCVA.
In conclusion, ILM flap techniques are superior in terms of anatomical results in myopic MH surgery.But, there is no concensus about which method is better for functional recovery.A larger, prospective, randomized studies are recommended to elucidate the long-term anatomical and visual outcomes of the three techniques for the treatment of myopic MH without RD.
ACKNOWLEDGEMENTS
Conflicts of Interest: Ozbek M,None;Ozcaliskan S,None;Alagoz C,None;Artunay O,None.
猜你喜欢
杂志排行

International Journal of Ophthalmology的其它文章
- A novel pathogenic splicing mutation of RPGR in a Chinese family with X-linked retinitis pigmentosa verified by minigene splicing assay
- Vault predicting after implantable collamer lens implantation using random forest network based on different features in ultrasound biomicroscopy images
- Multiple evanescent white dot syndrome relapse following BNT162b2 mRNA COVID-19 vaccination
- Acute micro-macular hole associating with extensive intraoperative rotation of implantable collamer lens without ophthalmic viscosurgical device assistance: a case report
- Effectiveness of conjunctival bleb scarring by knockdown of heat shock protein 47 in rat model
- Effect of miR-27b-3p and Nrf2 in human retinal pigment epithelial cell induced by high-glucose