Application of multidisciplinary collaborative nursing with family care for enhanced recovery after surgery in children with inguinal hernia
2023-10-21XiuMeiWangQiangHou
Xiu-Mei Wang, Qiang Hou
Abstract
Key Words: Multidisciplinary collaborative; Enhanced recovery after surgery; Family care; Perioperative nursing; Prognosis; Postoperative complications
INTRODUCTION
Inguinal hernia in children is a common pediatric disease that requires surgery, with an incidence rate of 1% to 4%. In these children, congenital development of the abdominal wall is imperfect and can form direct and oblique hernias. The oblique hernia and the incidence of hernia (in general) in male children is higher. After the male is born, the testis descends to the scrotum along the inguinal canal, and the peritoneum that descends with the testis forms a sheath process[1,2]. In children with an open sheath process, the abdominal pressure increases with constipation, cough, ascites, abdominal tumor, or long-term crying, causing abdominal organs such as the small intestine and omentum majus to protrude from the body surface through the internal ring outside the inferior abdominal artery and the subcutaneous ring. The clinical manifestation is a circular elastic mass on one side of the groin that can be recovered into the abdominal cavity. Currently, surgery is the only clinical treatment for oblique inguinal hernia in children. Children under 6 mo old easily self-heal, and those who do not self-heal require surgery. However, surgery may cause psychological and physical trauma, significantly affecting the postoperative rehabilitation of children; therefore, effective nursing is required during the perioperative period. Enhanced recovery after surgery (ERAS) refers to nursing protocols that relieve patients’ pain, reduce the stress response and complications, and promote postoperative rehabilitation by optimizing nursing measures during the perioperative period according to evidence-based medicine. Multidisciplinary collaboration is the medical strategy that integrates experts’ opinions in nursing, anesthesia, nutrition, surgery, and other disciplines for effective perioperative care. Currently, multidisciplinary collaborations are primarily applied to cancer treatment and nursing. With the continuous development of modern medical technology, interdisciplinary cooperation has become an inevitable trend in medical care. This strategy mainly targets medical care behaviors during the perioperative period of patients undergoing elective surgery, aiming to accelerate patients’ rehabilitation from the physiological, psychological, and social medical care modes[3,4]. Integrating multidisciplinary care into enhanced recovery will break down the barriers between disciplines and focus on coordinating the entire care process. Some domestic studies have explored the effects of multidisciplinary collaboration on ERAS. Lanet al[5] applied multidisciplinary collaborative nursing for ERAS to perioperative colorectal cancer patients and observed a significant shortening of the hospital stay. Zhouet al[6] also implemented ERAS nursing under multidisciplinary collaboration for patients undergoing a whole joint replacement surgery and observed effective postoperative recovery. Children with insufficient cognitive ability are more likely to have postoperative manifestations such as fear and nightmares. Family care emphasizes humanistic care in nursing to eliminate children’s negative emotions. Multidisciplinary collaborative nursing for ERAS has been widely used in clinical practice, with significant results[7,8]. Family care is also widely recommended for pediatric diseases[9,10].
This study explored the effects of multidisciplinary collaborative nursing combined with family care nursing for ERAS in the perioperative care of children with inguinal hernia.
MATERIALS AND METHODS
General data
This retrospective study analyzed the data of 100 children with an inguinal hernia from May 2020 to August 2022 and categorized them into Groups A (n= 38), B (n= 32), and C (n= 30) according to different nursing methods. In Group A, there were 35 males and 3 females, aged 17-24 mo (average = 20.89 ± 1.45 mo); there were 29 cases of right and 9 of left indirect hernias. Group B comprised 30 males and 2 females, aged 18-25 mo (average = 20.91 ± 1.94 mo), with 25 right and 7 left indirect hernia cases. Group C included 25 males and 5 females, aged 18-24 mo (average = 20.90 ± 1.37 mo), with 22 right and 8 cases of left indirect hernias. The general data of the three groups were comparable (P> 0.05).
Inclusion criteria
(1) Children diagnosed with an inguinal hernia by clinical symptoms, signs, and imaging data; (2) 6 mo ≤ age ≤ 6 years; (3) Children with unilateral indirect inguinal hernia; and (4) Children treated with internal ring high-ligationviatransumbilical single-site laparoscopy under general anesthesia.
Exclusion criteria
(1) Children with an external incarcerated and huge inguinal hernias (internal ring diameter ≥ 1.5 cm); (2) Children with severe organ dysfunction such as heart, liver, kidney, and lung; (3) Children with severe immune diseases; (4) Children with blood diseases; and (5) Children with contraindications to surgery.
Methods
Group C: Group C received routine perioperative nursing, including preoperative health education, postoperative water deprivation and fasting, intraoperative fluid replenishment, and routine warming.
Group B: Group B was given multidisciplinary collaborative ERAS nursing. (1) A multidisciplinary collaborative nursing team comprised of professionals from the pediatrics, anesthesiology, general surgery, nutrition, and psychology departments. The head nurse of pediatrics was the team leader for coordinating team affairs, and nurses from all departments were team members responsible for implementing the nursing plan. The team members jointly analyzed the condition of the children and formulated the anesthesia and perioperative management plans; (2) Preoperative nursing. Health education: The medical staff educated the patients about inguinal hernia by distributing a knowledge manual, informed children’s families of the possible perioperative conditions and provided relevant solutions, and encouraged the children with appropriate psychological care and preoperative contact to help them establish confidence to overcome the disease. Preoperative preparation: 6 h before the operation, fasting and water deprivation were performed, and a normal diet was resumed after anesthesia recovery. After a multidisciplinary discussion, an appropriate anesthesia plan was determined; (3) Intraoperative nursing. Intraoperative warming: The operating room temperature was controlled at 24-26 ℃, and the disinfection and towel-laying processes were closely connected. Strict liquid intake control: Liquid intake was maintained at 6-10 mL/kg/h to avoid bladder swelling at the end of the surgery, causing restfulness in children. Intraoperative analgesia: Appropriate lidocaine cream was applied after endotracheal incubation, and local infiltration anesthesia was administered with bupivacaine for umbilicus abdominal access after the operation. Bladder emptying: Before surgery, after successful anesthesia, the bladder area was squeezed to empty to avoid the surgical vision field; and (4) Postoperative nursing. Pain management: Children were distracted from pain and discomfort by distracting their attention, instructing their families to provide toys they love, playing music or cartoons they like, and with pacifiers or licking lollipops. During the operation, children with tracheal intubation failure were given methylprednisolone (1-2 mg/kg) prophylactically and budesonide (0.5-1 mg/time) by intravenous drip or aerosol inhalation per doctors’ advice. Children with incision pain were given intravenous tramadol 1-2 mg/kg (≤ 100 mg) and oral ibuprofen 10 mg/kg (≤ 200 mg). Diet management: Children were allowed lollipops after anesthesia to reduce hunger and for a pacifying role. This fake feeding behavior also promotes the recovery of gastrointestinal function and reduces postoperative complications. Children were allowed to drink a small amount of water 4 h postoperatively with 15 min of observation. If the child did not appear nauseous, vomit, or show any other symptoms, they were allowed liquid food, followed by multiple small meals, to gradually transition from semi-liquid to general food. Oxygen inhalation: After surgery, the children’s face and lips were observed for an anoxic state, the blood oxygen saturation changes were measured, and low-flow oxygen was given according to the children’s needs. Fluid supplement: After the operation, a small amount of fluid was given, and the amount and infusion speed were adjusted according to the age and the children’s body mass. The fluid amount was < 500 mL/d and the infusion stopped the next day after the operation. Early activity: Activity was recommended at the earliest after the operation. After awakening, the child was put in a knee flexion supine position to reduce the abdominal incisions’ tension and the incision pain. After anesthesia, children could move properly in bed when they woke up and left the bed after 6 h; intense activities were avoided.
Group A: For ERAS, Group A received multidisciplinary collaborative nursing and family care nursing. Multidisciplinary collaborative ERAS nursing protocols were similar to Group B. Family care operating room: The head nurse of the department of pediatrics carefully analyzed the children’s medical records, inquired about their condition in detail, and developed a perioperative family care nursing protocol. (1) Admission: The receiving nurse dressed properly and introduced herself to family members and children with a kind attitude and etiquette; (2) Hospitalization: During hospitalization, “smile” communication was performed to understand a child’s needs. During communication, gentle children’s heads touch comforted them through physical contact, gave them a sense of intimacy, and eliminated their fear. Every day, a thoughtful greeting and a caring action were exhibited to the child to make him feel warm. If a child asked questions, patient and gentle answers were given and were actively communicated with to ensure comfort to the child and family; and (3) Discharge: Nurses organized children to hold hands and wish each other a happy life. This “handshake” activity sends family affection to the children and eliminates their fear and inferiority complex. Nurses were guided to pay more attention to the children and their families, greet and explain, and give them more preoperative and postoperative comfort.
Indicator analysis
(1) Postoperative rehabilitation process. The changes in postoperative rehabilitation indexes, such as blood loss, feeding time, the time of getting out of bed, hospitalization time, and defecation time, were compared among the three groups; (2) The postoperative pain at 4, 12, and 24 h was assessed and compared among the three groups. With the help of facial expression scoring (FLACC)[11], the pain at 4, 12, and 24 h after surgery was evaluated in the three groups. The scale is applied to children aged 0 to 7 years and comprises five items with a total score of 10 points, where 0 = painless, 1-3 = mild pain, 4-6 = moderate pain, and 7-10 = severe pain; (3) Comparison of postoperative stress indexes among the three groups. The heart rate (HR), systolic blood pressure (SBP), and diastolic BP (DBP) were assessed in the three groups before and 1 h after the operation. Furthermore, 3 mL fasting venous blood was collected from the three groups before and 1 h after the operation. After serum separation, the three groups’ noradrenaline (NE) and cortisol (Cor) levels were determined by the enzyme-linked immunosorbent assay; (4) Comparison of complications among the three groups; and (5) Family satisfaction. A questionnaire was established to evaluate the satisfaction of patients’ family members with nursing, including health education, nursing attitude, nursing quality, and psychological nursing. The full score of each content was 0-100 points; the higher the score, the higher the satisfaction.
Statistical methods
Two persons independently entered all data into excel tables, analyzed it, and then processed it using SPSS 24.0. The data are expressed as the mean ± SD. For normally distributed and homogeneous variance data, at-test was performed, and single-factor analysis of variance was performed for the intergroup comparison. Counting data were described bynand %, and not normally distributed data were compared byχ2test or the Fisher’s exact test.P< 0.05 was considered statistically significant.
RESULTS
Comparison of postoperative rehabilitation progress of the three groups
There was less intraoperative blood loss in Groups A and B than in Group C (P< 0.05), and the postoperative time of getting out of bed, hospitalization time, and defecation were also lower than in Group C (P< 0.05). There was no significant difference in postoperative feeding time among the three groups (P> 0.05). There was no statistically significant difference in each index between Groups A and B (P> 0.05) (Table 1).
Comparison of postoperative FLACC scores at 4, 12, and 24 h in the three groups
There was no significant difference in postoperative FLACC scores among the three groups at 4 h (P> 0.05). At 12 and 24 h after surgery, the FLACC score of the three groups was decreased (P< 0.05). The FLACC scores were lower in Groups A and B than in Group C (P< 0.05), and lower in Group A than in Group B (P< 0.05) (Table 2).
Comparison of stress indexes among the three groups
No significant differences were observed in the preoperative HR, SBP, DBP, NE, and Cor levels among the three groups (P> 0.05). At 1 h after surgery, the HR, SBP, DBP, NE, and Cor levels in the three groups were increased (P< 0.05). The HR, SBP, DBP, NE, and Cor changes before and after surgery in Groups A and B were less than those in Group C (P< 0.05). The HR, NE, and Cor changes in Group A pre- and post-surgery were less than those in Group B (P< 0.05) (Table 3).
Comparison of complications among the three groups
There was a lower incidence of urinary retention, infection, hematoma, hernia recurrence, and other complications in Group A than in Group C (P< 0.05). No significant differences were identified in the overall complication rate between Groups A and B and between Groups B and C (P> 0.05) (Table 4).
Comparison of satisfaction among three groups
Groups A and B scores for health education, nursing attitude, nursing quality, and psychological nursing satisfaction were higher than those in Group C (P< 0.05), and each satisfaction score in Group A was higher than that in Group B (P< 0.05) (Table 5).
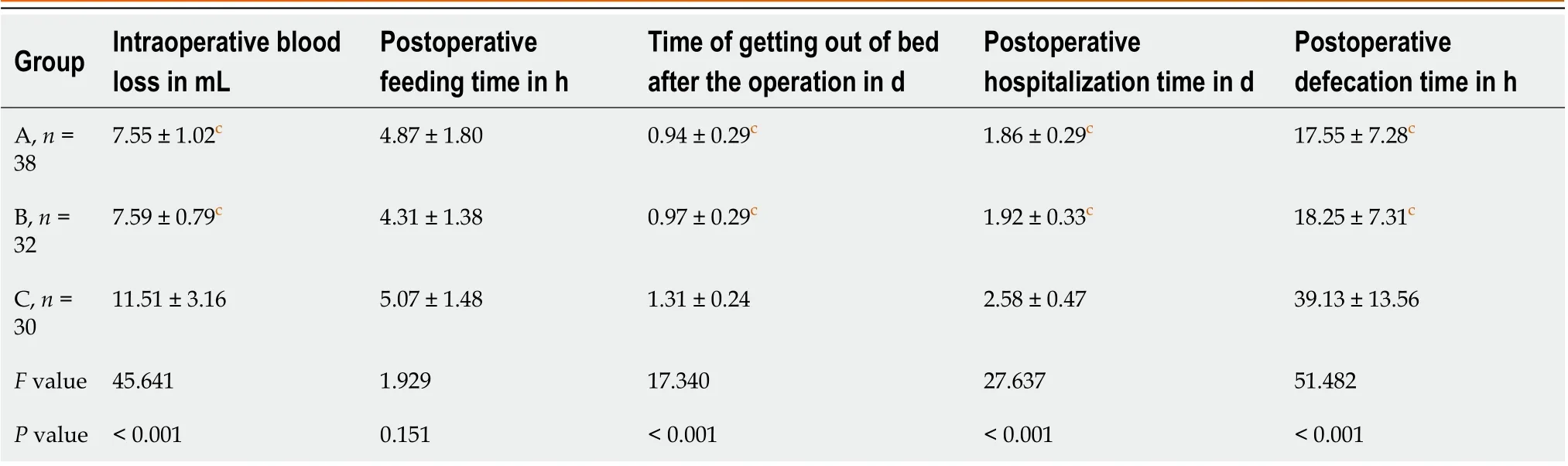
Table 1 Comparison of postoperative rehabilitation progress of the three groups
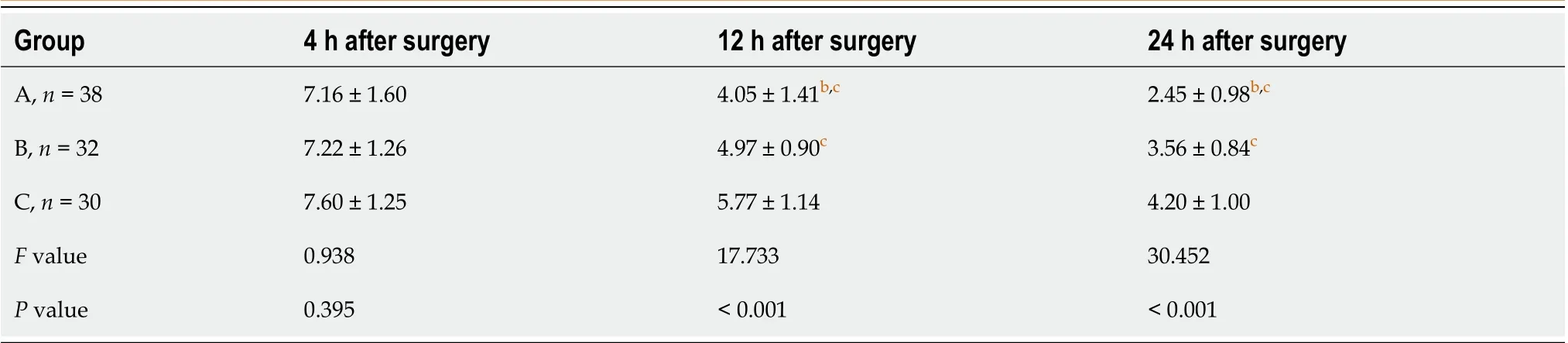
Table 2 Comparison of facial expression scoring scores at 4, 12, and 24 h after surgery in the three groups
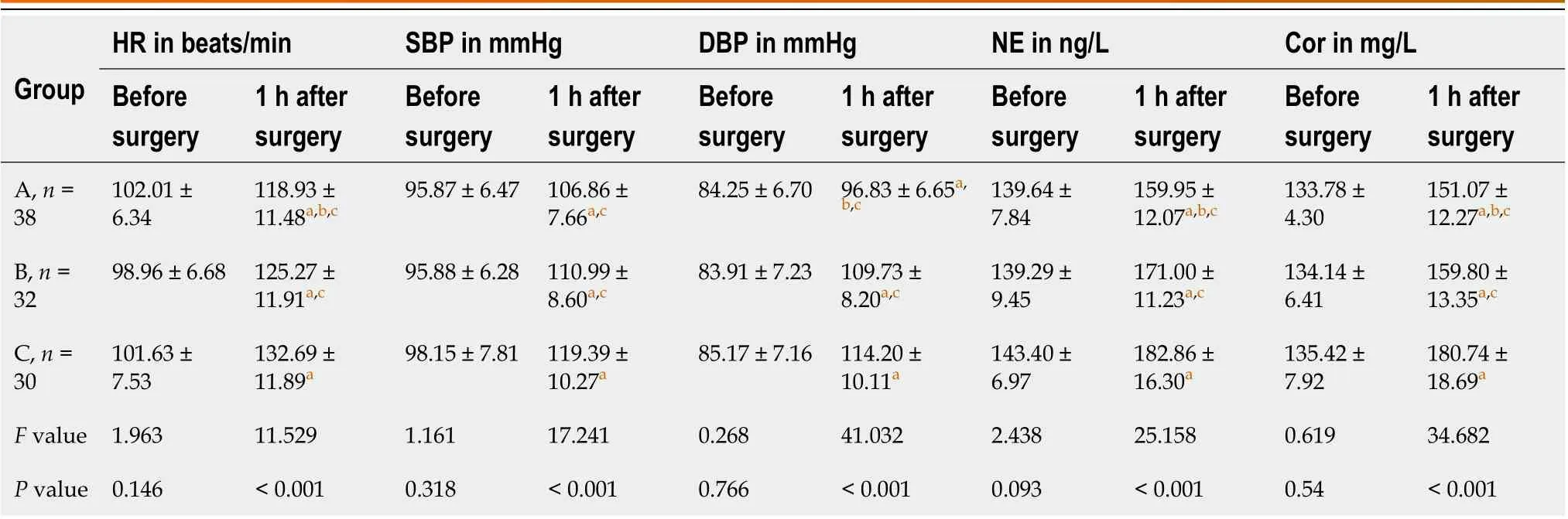
Table 3 Comparison of stress indexes among the three groups
DISCUSSION
The ERAS is a novel protocol with many advantages over traditional perioperative management. It has been widely used in orthopedics, obstetrics and gynecology, oncology, and other departments[12-14], achieving good outcomes. The multidisciplinary collaborative mode is the clinical treatment/nursing strategy developed by professionals from different disciplines for a certain disease. In the multidisciplinary collaborative nursing for ERAS, multidisciplinary clinical knowledge is integrated into nursing. This is a challenge for professionals of different departments such as pediatrics, anesthesiology, comprehensive surgery, nutrition, and psychology[15,16]. In nursing, family care refers to treating children as relatives and providing them with comprehensive, considerate, and safe services, embodying humanized nursing mode. Family care has also been widely used for patients’ breast cancer and other diseases, with significant effects[9,10].
由于独立学院学生英语底子薄、学习积极性不强,视听说课堂活动流于形式,教学效果不佳。为充分调动学生积极性,提高其听说能力,优化视听说教学设计尤为重要。

Table 4 Comparison of complications among the three groups
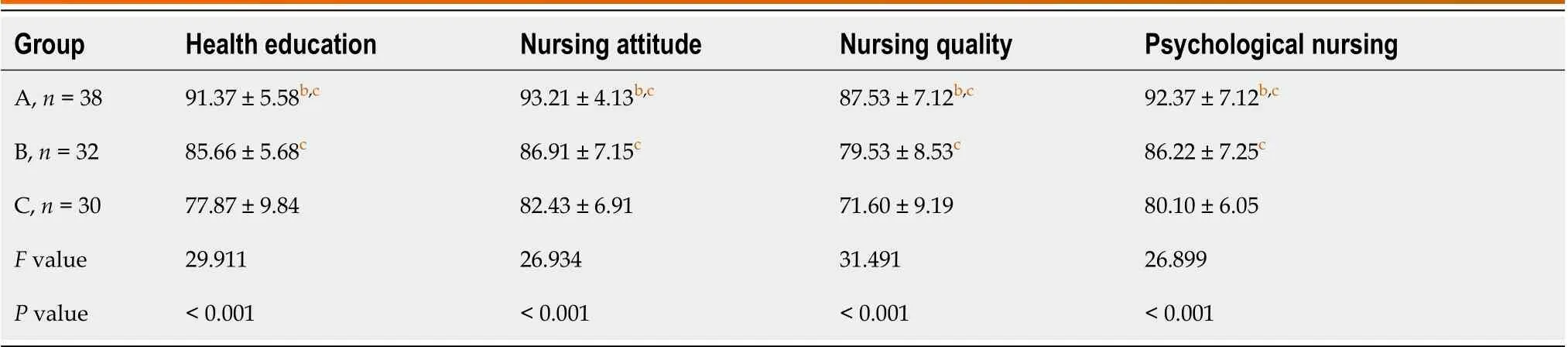
Table 5 Comparison of satisfaction among the three groups
In this study, Group A was given multidisciplinary collaborative nursing combined with family care for ERAS, Group B was given multidisciplinary collaborative nursing for ERAS, and Group C was only given routine nursing. The results showed that the intraoperative blood loss and postoperative time of getting out of bed, hospitalization, and defecation in Groups A and B were significantly better than in Group C. There was no significant difference in postoperative rehabilitation indexes between Groups A and B, suggesting that multidisciplinary collaborative nursing for ERAS can significantly improve postoperative recovery and the prognosis of children with inguinal hernia surgery. The multidisciplinary collaborative nursing for ERAS, a multidisciplinary collaborative team for nursing management, was established. The personnel from the pediatrics, anesthesia, general surgery, nutrition, and psychology departments analyzed the physiological and psychological conditions of the children. The anesthesia and perioperative nursing plans were formulated. Intraoperative fluid control, anesthesia (per anesthesiologist advice), and intraoperative heat preservation were important for a smooth operation and reduced postsurgical outcomes. Furthermore, postoperative pain management, early exercise, and diet management also reduce pain and shorten the postoperative time of hospital stay, getting out of bed, and defecation[17,18]. Multiple previous studies[19,20] have shown that multidisciplinary collaborative ERAS nursing effectively promotes postoperative rehabilitation of patients, consistent with the results of this study. In terms of pain, improved FLACC scores were observed in Groups A and B than in Group C, and that of Group A was better than Group B. Both Groups A and B received multidisciplinary collaborative nursing for ERAS; pain management programs were developed through multidisciplinary discussion; therefore, paint improvement was better than Group C receiving routine nursing. Stressful invasive surgery can cause trauma to the children’s body. Additionally, the fear of an unfamiliar environment can cause anxiety, depression, and other negative emotions. According to the literature[21], postoperative pain is closely related to anxiety and depression, and other adverse emotions. Therefore, the family care nursing in Group A improved children’s bad mood and relieved their incision pain with care and love similar to their relatives, indicating improved pain in Group A than in Group B.
According to related reports[22], traumatic surgical stimulation can lead to the excitation of the sympathetic nervous system, increased adrenaline secretion, and hemodynamic changes in patients, manifested as increased HR and BP. Due to cognitive insufficiency, children show strong psychological stress when facing traumatic surgery. Here, the stress indexes, including HR, SBP, DBP, NE, and Cor levels in Groups A and B one hour before and after surgery, were less than in Group C, and that of Group A was decreased than in Group B. The results showed that multidisciplinary collaborative nursing combined with family care nursing positively relieved children’s physiological stress, indicating that in Groups A and B, attention was paid to environmental management during surgery, the appropriate temperature was adjusted, physiological discomfort was reduced, and psychological intervention was given to children before and after surgery. Since Group A was treated with family care nursing, the nursing staff actively encouraged and comforted the children like their relatives, increased communication to divert their attention, and managed their pain. The combined action of various measures effectively relieved their stress response. Furthermore, the incidence of urinary retention, infection, hematoma, hernia recurrence, and other complications in Group A was lower than in Group C (P< 0.05). No significant difference was observed in the overall complication rate between Groups A and B and between B and C (P> 0.05). The satisfaction scores of health education, nursing attitude, nursing quality, and psychological nursing in Groups A and B were higher than Group C (P< 0.05), and each satisfaction score of Group A was higher than Group B (P< 0.05). It was indicated that multidisciplinary collaborative nursing with family care effectively alleviated the complications in children and improved the nursing satisfaction of their families by providing high-quality nursing care with multidisciplinary opinions such as nursing, nutrition, and psychological intervention. Family care can also improve nursing compliance and reduce the incidence of complications to a certain extent through encouragement. Combined nursing integrates multidisciplinary collaboration, ERAS, and family care models. It is highly professional in health education, nursing attitude, nursing quality, and psychological intervention, so the family members of children are more satisfied.
The limitation of this retrospective study was its small size. Therefore, for additional perspectives, a large sample size and multicenter study are required to explore the influence of multidisciplinary collaborative nursing with family care for ERAS in children with inguinal hernia.
CONCLUSION
In conclusion, the application of multidisciplinary collaborative nursing with family care for ERAS in perioperative children with an inguinal hernia can effectively improve their postoperative recovery, relieve their pain, reduce their postoperative stress and incidence of complications, and improve the satisfaction of their families, which has clinical application value.
ARTICLE HIGHLIGHTS


FOOTNOTES
Author contributions:Wang XM were responsible for the research design, conducting the experiments, and data acquisition; Hou Q were responsible for the investigation, data analysis, writing, and revising the manuscript; Both authors contributed to the completion of this paper.
Institutional review board statement:The study was reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Shandong First Medical University.
Informed consent statement:As the study used anonymous and pre-existing data, the requirement for the informed consent from patients was waived.
Conflict-of-interest statement:The authors have no financial relationships to disclose.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Qiang Hou 0009-0002-3787-7554.
S-Editor:Qu XL
L-Editor:Filipodia
P-Editor:Cai YX
猜你喜欢
杂志排行
World Journal of Gastrointestinal Surgery的其它文章
- Quantitative evaluation of colorectal tumour vasculature using contrast-enhanced ultrasound: Correlation with angiogenesis and prognostic significance
- Risk factors for myocardial injury during living donor liver transplantation in pediatric patients with biliary atresia
- Value of enhanced computed tomography in differentiating small mesenchymal tumours of the gastrointestinal from smooth muscle tumours
- Multifactor analysis of the technique in total laparoscopic gastric cancer
- Clinical significance of serum oxidative stress and serum uric acid levels before surgery for hepatitis Brelated liver cancer
- Prediction model of stress ulcer after laparoscopic surgery for colorectal cancer established by machine learning algorithm