Corrected QT interval in cirrhosis: A systematic review and metaanalysis
2023-10-19VasileiosPeriklisPapdopoulosKonstantinosMimidis
Vasileios Periklis Pap.dopoulos,Konstantinos Mimidis
Abstract BACKGROUND Corrected QT (QTc) interval is prolonged in patients with liver cirrhosis and has been proposed to correlate with the severity of the disease.However,the effects of sex,age,severity,and etiology of cirrhosis on QTc have not been elucidated.At the same time,the role of treatment,acute illness,and liver transplantation (Tx)remains largely unknown.AIM To determine the mean QTc in patients with cirrhosis,assess whether QTc is prolonged in patients with cirrhosis,and investigate whether QTc is affected by factors such as sex,age,severity,etiology,treatment,acute illness,and liver Tx.METHODS In the present systematic review and meta-analysis,the searching protocol“{[QTc] OR [QT interval] OR [QT-interval] OR [Q-T syndrome]} AND {[cirrhosis]OR [Child-Pugh] OR [MELD]}” was applied in PubMed,EMBASE,and Google Scholar databases to identify studies that reported QTc in patients with cirrhosis and published after 1998.Seventy-three studies were considered eligible.Data concerning first author,year of publication,type of study,method used,sample size,mean age,female ratio,alcoholic etiology of cirrhosis ratio,Child-Pugh A/B/C ratio,mean model for end-stage liver disease (MELD) score,treatment with β-blockers,episode of acute gastrointestinal bleeding,formula for QT correction,mean pulse rate,QTc in patients with cirrhosis and controls,and QTc according to etiology of cirrhosis,sex,Child-Pugh stage,MELD score,and liver Tx status (pre-Tx/post-Tx) were retrieved.The Newcastle-Ottawa quality assessment scale appraised the quality of the eligible studies.Effect estimates,expressed as proportions or standardized mean differences,were combined using the ra.domeffects,generic inverse variance method of DerSimonian and Laird.Subgroup,sensitivity analysis,and meta-regressions were applied to assess heterogeneity.The study has been registered in the PROSPERO database (CRD42023416595).RESULTS QTc combined mean in patients with cirrhosis was 444.8 ms [95% confidence interval (CI): 440.4-449.2;P < 0.001 when compared with the upper normal limit of 440 ms],presenting high heterogeneity (I2=97.5%;95%CI: 97.2%-97.8%);both Egger’s and Begg’s tests showed non-significance.QTc was elongated in patients with cirrhosis compared with controls (P < 0.001).QTc was longer in patients with Child-Pugh C cirrhosis when compared with Child-Pugh B and A (P < 0.001);Child-Pugh B patients presented longer QTc when compared with Child-Pugh A patients (P=0.003).The MELD score was higher in patients with cirrhosis with QTc > 440 ms when compared with QTc ≤ 440 ms (P < 0.001).No correlation of QTc with age (P=0.693),sex (P=0.753),or etiology (P=0.418) was detected.β-blockers shortened QTc (P< 0.001).QTc was prolonged during acute gastrointestinal bleeding (P=0.020).Tx tended to improve QTc (P < 0.001).No other sources of QTc heterogeneity were revealed.CONCLUSION QTc is prolonged in cirrhosis independently of sex,age,and etiology but is correlated with severity and affected by β-blockers and acute gastrointestinal bleeding.QTc is improved after liver Tx.
Key Words: Liver cirrhosis;Corrected QT interval;Child-Pugh stage;Model for end-stage liver disease score;Liver transplantation;Meta-analysis
INTRODUCTION
The prolongation of ventricular repolarization,as reflected in rate-corrected QT (QTc) electrocardiogram interval,was first reported in 44% of patients with cirrhosis of alcoholic etiology[1,2].QTc prolongation was soon recognized as a frequent electrocardiographic abnormality in patients with cirrhosis,regardless of the subsequent etiology[3,4].QTc prolongation has been historically attributed to a broad spectrum of pathophysiological mechanisms involving electrolyte imbalance,sympathetic nervous system hyperactivity,portal hypertension,elevated bile salt plasma concentrations,direct alcohol toxicity,regimens such as β-blockers and diuretics,and stressful events such as acute gastrointestinal bleeding[1,3,5-10].However,QTc prolongation is currently considered to reflect delayed ventricular repolarization in the presence of cirrhotic cardiomyopathy,an entity characterized mainly by ventricular diastolic dysfunction associated with liver cirrhosis in the absence of other known cardiac disease[11-19].Of note,some contradictory evidence support that QTc prolongation is independent of the structural and functional abnormalities that characterize cirrhotic cardiomyopathy[20].Moreover,it is debatable whether taming the gonadal hormone metabolism in cirrhosis might blur QTc sexdependence observed in patients without cirrhosis[21].Interestingly,liver transplantation (Tx) has been demonstrated to at least partly restore prolonged QTc[4,21-25].
QTc prolongation > 440 ms has been correlated with shortened overall survival in cirrhosis[3,26,27];however,there is contradictory evidence obscuring this proposal[28].More commonly,QTc length has been considered to reflect the severity of the disease in terms of either Child-Pugh stage[26,29-37] or model for end-stage liver disease (MELD) score[27,37-40].On the contrary,several studies support dissimilar conclusions[4,41-45].Additionally,the direct (due to alcoholic cardiomyopathy) and indirect (due to the aggravated course of the disease) role of alcohol in QTc cirrhosis-linked prolongation is still debatable[1].Whether QTc abnormalities are more pronounced in alcoholic cirrhosis has not been elucidated yet,as there is contradictory evidence either for[33,46] or against[24,25,47] that possibility.Finally,QTc sex dependence might be less evident or even absent in patients with cirrhosis[3,21,23,25,30,38-41].
The present systematic review and meta-analysis was conducted to provide further evidence regarding a potential correlation between QTc length in patients with cirrhosis and age,sex,etiology of cirrhosis,severity of the disease in terms of Child-Pugh stage,and MELD score,treatment with β-blockers,episode of acute gastrointestinal bleeding,as well as liver Tx by identifying all relevant studies and summarizing their results.
MATERIALS AND METHODS
Literature search
The study was conducted following Preferred Reporting in Systematic and Meta-Analysis (PRISMA) guidelines[48].We used the PubMed and EMBASE databases to identify studies that reported QTc in patients with cirrhosis and were published between January 1998 and April 2023.We also utilized the Google Scholar database to retrieve any additional published or unpublished data,such as conference proceedings and other grey literature.We performed an iterative search until we could trace no additional publications.Moreover,a search for unpublished dissertations as well as other unpublished work was completed.The literature search was performed by both authors (Pap.dopoulos VP and Mimidis K).The study has been registered in the PROSPERO database (CRD42023416595);PROSPERO data were revised on August 8,2023[49].
Study selection
The present systematic review was conducted following a search strategy that included the terms {[QTc] OR [QT interval]OR [QT-interval] OR [Q-T syndrome]} AND {[cirrhosis] OR [Child-Pugh] OR [MELD]}.Pre-specified eligibility criteria used the PICO strategy [P: Populations/people/patient/problem: Patients who have cirrhosis and healthy individuals(controls),I: Intervention(s): Liver Tx,C: Comparison: QTc in (1) Patients with cirrhosisvsupper normal limit;(2) Patients with cirrhosisvscontrols;(3) Males with cirrhosisvsfemales with cirrhosis;(4) Patients with cirrhosis of Child-Pugh stage AvsBvsC;(5) Patients with cirrhosis of alcoholic etiologyvsviral etiology;(6) Relation with age;(7) Relation with MELD score;(8) Patients with cirrhosis beforevsafter liver Tx;(9) Relation with β-blockers;(10) Relation with episode of acute gastrointestinal bleeding;and (11) Relation with age,sex,and etiology of cirrhosis in transplanted patients,O: Outcome:Combined mean,percentage;standardized mean difference (SMD)][50].Exclusion criteria were: (1) Review articles,case reports,and letters;(2) Duplicated or overlapping studies (if that was the case,only the most recent or the highest level of study or the most informative study was included);and (3) Studies published only as abstracts.The process was performed independently by both authors.Mimidis K was responsible for resolving any discordance.The Cohen kappa statistic was preferred to assess the level of agreement between the two investigators.No software was used for study retrieval.Sources of financial support were traced where possible.
Data extraction
Data concerning first author,year of publication,type of study,method used,sample size,mean age,female ratio,alcoholic etiology of cirrhosis ratio,Child-Pugh A/B/C ratio,mean MELD score,use of β-blockers,formula for QT correction,mean pulse rate,QTc in patients with cirrhosis and controls,and QTc according to etiology of cirrhosis,sex,Child-Pugh stage,and Tx status (pre-Tx/post-Tx) were retrieved independently by both authors.Mimidis K supervised the process and resolved any potential discordance.
Risk of bias
Funnel plots assessed the risk of publication bias.Trim-and-fill analysis was used to impute missing studies in cases of significant publication bias.The Newcastle-Ottawa Scale (NOS) evaluated the risk of bias assessment of the eligible studies;scores ≥ 7-9,4-6,and < 4 were considered to reflect low,intermediate,and high risk,respectively[51].Furthermore,the GRADE assessment was used to evaluate evidence certainty rating risk of bias,imprecision,inconsistency,indirectness,publication bias,and effect size for every endpoint[52].When comparing hazard ratios (HRs)between two groups,small,medium,and large effect sizes were considered to be approximately 1.3,1.9,and 2.8,respectively[53].
Statistical analysis
Data were synthesized using MedCalc Statistical Software version 20.218 (MedCalc Software bv,Ostend,Belgium;https://www.medcalc.org;2023).Effect estimates,expressed as QTc/upper normal limit percentage or SMD,were extracted from every study possible and combined using the ra.dom-effects,generic inverse variance method of DerSimonian and Laird[54],which assigned the weight of each study in the pooled analysis inversely to its variance.Combination of means and standard deviations (SDs) were performed using the freely available online tool located at https://www.statst.do.com/CombineMeansSDs.php.Means and estimates based on sample size,median,range,and interquartile range were calculated using the freely available online tool located at https://www.math.hkbu.edu.hk/~tongt/papers/median2mean.html[55-57].SD estimates were computed from the mean,confidence interval (CI),and sample size using the freely available online tool https://www.omnicalculator.com/statistics/confidence-interval.Effect size Cohen’sdwas calculated from 22contingency data using the freely available online tool https://www.psychometrica.de/effect_size.html.The correlation coefficient was calculated for paired data using the formula (SDbaseline2+SDfinal2-SDchange2)/(2 ×SDbaseline× SDfinal).A subgroup analysis was performed to investigate the potential effect of hospitalization,comorbidities,and treatments affecting QT.Sensitivity analysis assessed the correlation coefficientrconcerning pre-Tx and post-Tx status.HR was calculated from time-to-event data and log-rankPvalue as described elsewhere[58].The NORMSINV function,freely available from MedCalc software,was used for that purpose.The formula QTBazett=QTFridericia× RR-1/6was used to convert QTFridericia(QTc corrected with the use of Fridericia formula) to QTBazett(QTc corrected with the use of Bazett formula) given that the mean heart rate was 60-100 beats/min.Heterogeneity was approached using theQtest andI2statistic;QtestPvalue < 0.10 was indicative of a statistically significant result.Furthermore,a value ofI2≤ 25% was indicative of insignificant heterogeneity,26%-50% of low heterogeneity,51%-75% of moderate heterogeneity,and > 75%of high heterogeneity[59,60].Heterogeneity was analyzed through meta-regressions and derived standardized coefficients beta (bSD) focusing separately on study characteristics and quality assessment.Multivariate analysis was omitted in cases where the available studies numbered less than 10.Meta-regressions were performed using SPSS 26.0 software(IBM Corp.,Armonk,NY,United States).Synthesis of effect sizes was performed using the MedCalc®Statistical Software version 20.218 and Meta-Essentials Excel-based software[61].
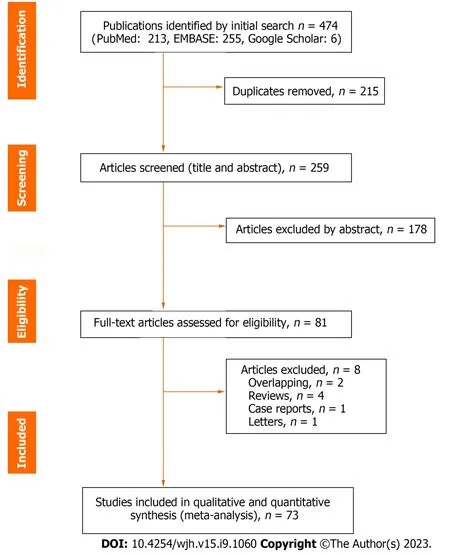
Figure 1 Study selection.
RESULTS
Study selection
Four hundred and sixty-eight potentially relevant publications (PubMed: 213,EMBASE: 255,Google Scholar: 6) were identified.No unpublished data of interest were detected.The authors removed duplicates and critically appraised the title,the abstract,and the full text of the remaining publications (Figure 1).Finally,73 studies,including 14495 patients,were eligible for qualitative and quantitative meta-analyses (Table 1)[3,4,6,7,10-15,17,18,21,23-47,62-96].
QTc interval in patients with cirrhosis
QTc was elongated in patients with cirrhosis when compared with controls (SMD=1.187;95%CI: 0.804-1.570;P< 0.001).TheI2was 88.8% (95%CI: 81.0%-93.4%;P< 0.001) (Figure 2A).QTc combined mean in patients with cirrhosis (n=7715)was 444.8 ms (95%CI: 440.4-449.2;P< 0.001 when compared with the upper normal limit of 440 ms),presenting high heterogeneity (I2: 97.5%;95%CI: 97.2%-97.8%;P< 0.001) (Figure 2B).
A subgroup analysis was performed to investigate the potential effect of hospitalization,comorbidities,and treatments affecting QT.Thus,when non-hospitalized patients with cirrhosis without any other comorbid condition or treatment with known effect of QT were considered (n=1448),the QTc combined mean was 444.0 ms (95%CI: 437.8-450.1) with anI2of 92.4% (95%CI: 89.6%-94.5%;P< 0.001).When patients with cirrhosis who either might have been hospitalized or presented other comorbidities or were treated with regimens affecting QT were considered (n=6267),the QTc combined mean was 445.3 ms (95%CI: 439.6-450.6) with anI2of 98.1% (95%CI: 97.9%-98.4%;P< 0.001).These two groups yielded comparable results (P=0.823) (Supplementary Figures 1 and 2).
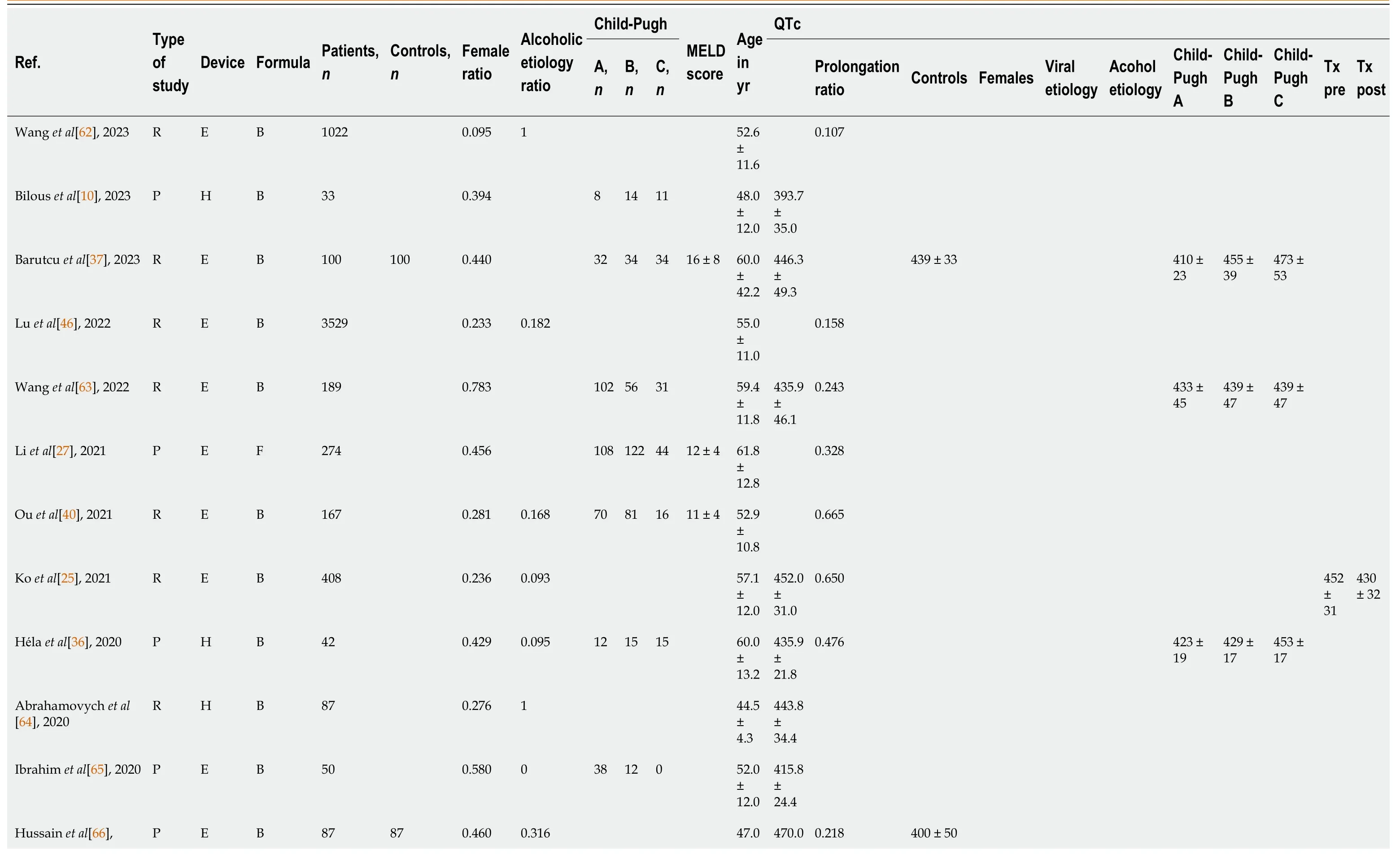
Table 1 Characteristics of eligible studies
The pre-specified upper normal limit for QTc was higher for females (median: 440 ms;range: 440-470 ms) when compared with males (median: 440 ms;range: 420-462 ms).The related samples Wilcoxon signed rank test showed statistical significance (P< 0.001) (Figure 3).
Effect of sex and age on QTc interval
QTc was comparable between male and female patients (SMD=-0.032;95%CI: -0.229 to 0.165;P=0.753);I2was 78.5%(95%CI: 62.0%-87.8%;P< 0.001) (Figure 4A).Moreover,no correlation of QTc with age (P=0.974) was detected,even after adjustment for alcoholic etiology rate and MELD score (Padj=0.160).
Effect of etiology of cirrhosis on QTc interval
Patients with cirrhosis of alcoholic etiology exhibited comparable QTc with those of viral etiology (SMD=0.095;95%CI:-0.109 to 0.264;P=0.418).Heterogeneity was moderate (I2: 47.8%;95%CI: 0.0%-74.8%;P=0.045) (Figure 4B).
Effect of Child-Pugh stage and MELD score on QTc interval
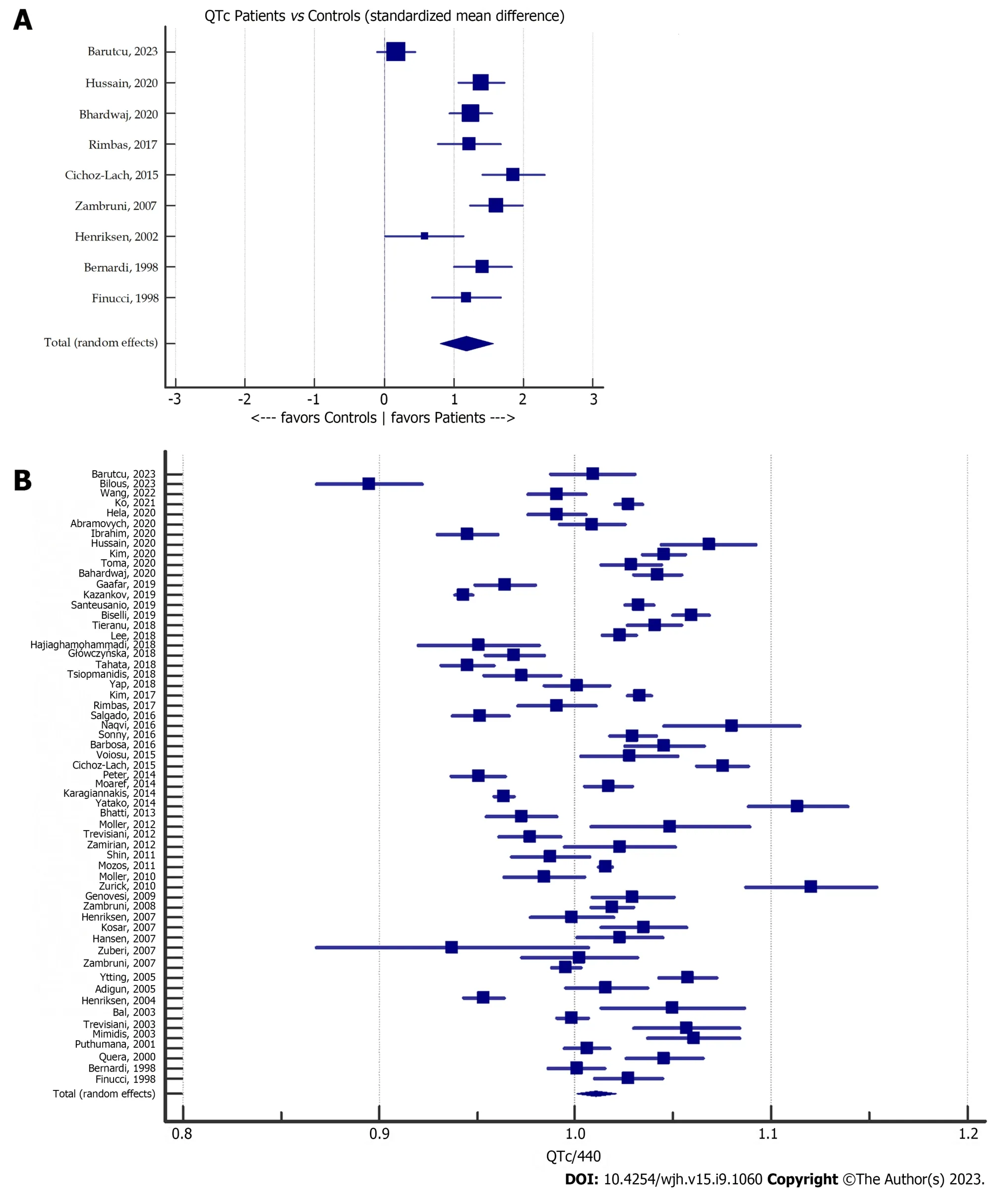
Figure 2 Meta-analysis forest plot. A: Corrected QT (QTc) in patients with cirrhosis vs controls;B: QTc compared with the upper normal limit (440 ms) ratio in patients with cirrhosis.QTc: Corrected QT.
QTc was longer in patients with Child-Pugh C cirrhosis when compared with Child-Pugh A (SMD=0.860;95%CI: 0.547-1.173;P< 0.001) and B (SMD=0.474;95%CI: 0.344-0.6003;P< 0.001);I2was 80.8% (95%CI: 71.5%-87.1%;P< 0.001) and 24.9% (95%CI: 0.0%-55.4%;P=0.647),respectively (Figures 5A and B).Moreover,Child-Pugh B patients with cirrhosis were characterized by longer QTc when compared with Child-Pugh A patients (SMD=0.372;95%CI: 0.126-0.619;P=0.003);I2was 76.0% (95%CI: 63.5%-84.2%;P< 0.001) (Figure 5C).Considering the effect of the Child-Pugh score on QTc,a significant.dose-response gradient was observed using Spearman’s non-parametric correlation coefficient (rho=0.526,P< 0.001).The MELD score was higher in patients with cirrhosis with QTc > 440 ms when compared with patients with QTc ≤ 440 ms (SMD=0.509;95%CI: 0.249-0.769;P< 0.001);I2was 78.1% (95%CI: 47.4%-90.9%;P=0.001) (Figure 6A).
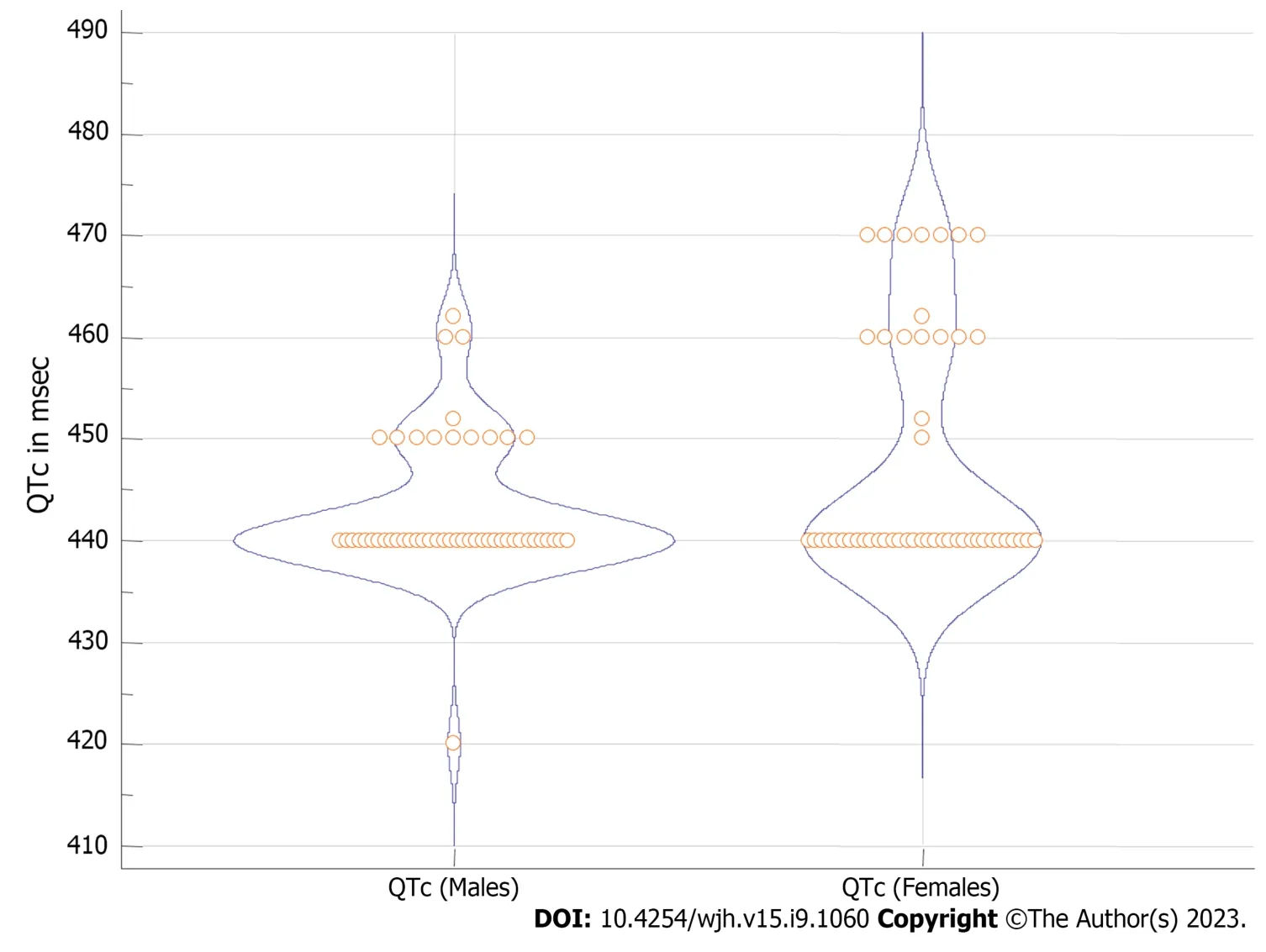
Figure 3 Violi plot for corrected QT upper normal limit used in the included studies. QTc: Corrected QT.
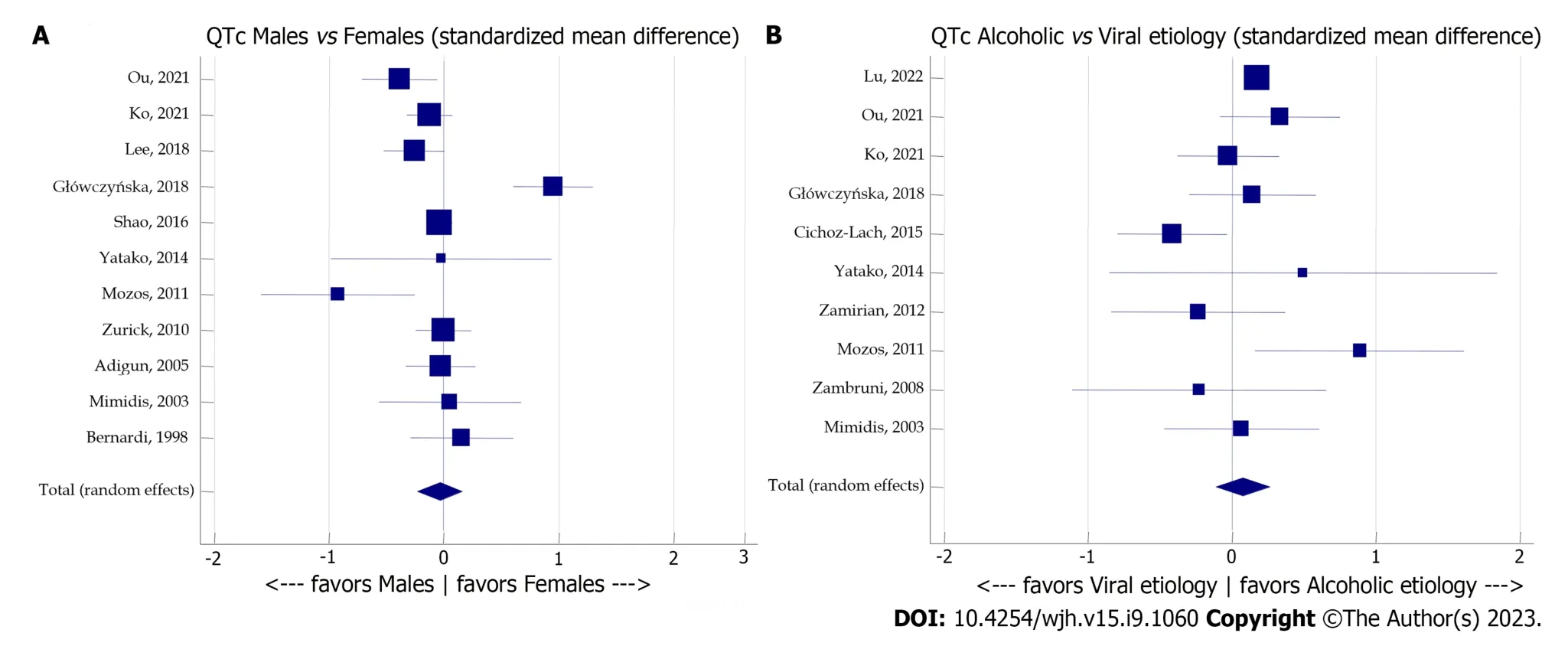
Figure 4 Meta-analysis forest plot concerning the effect of sex and etiology of cirrhosis on corrected QT. A: The effect of sex on corrected QT(QTc) in patients with cirrhosis;B: The effect of etiology of cirrhosis on QTc.QTc: Corrected QT.
Role of liver Tx regarding QTc interval
Liver Tx tended to improve QTc (pre-Txvspost-Tx QTc SMD=0.808;95%CI: 0.488-1.129;P< 0.001).I2was 93.9% (95%CI:90.1%-96.2%;P< 0.001) (Figure 6B).Since pre-Tx and post-Tx QTc values were correlated,the correlation coefficientrwas 0.7,using two separate approaches: (1) Sensitivity analysis forr=0.1 tor=0.9 (step 0.1),which suggested that the combined Hedges’g (0.714;95%CI: 0.645-0.783) withI2: 0.00% (P=0.988) corresponded to 0.7 <r< 0.8;and (2) Direct calculation from Finucciet al[4],which resulted inr=0.642 (Figure 7).QTc improvement after Tx remained unaffected by age (P=0.417) and was negatively correlated with female ratio (P=0.002),alcoholic etiology of cirrhosis ratio (P< 0.001),and age of the study (P=0.019) (Figures 8A-D).
Pharmacological effects on QTc: The paradigm of β-blockers
The effect of β-blockers on QTc was investigated using data from three relevant studies.Patients with cirrhosis who were treated with β-blockers presented shorter QTc than those who were not (SMD=-0.540;95%CI: -0.836 to -0.243;P< 0.001);I2was 0.0% (95%CI: 0.0%-92.1%;P=0.653) (Supplementary Figure 3).
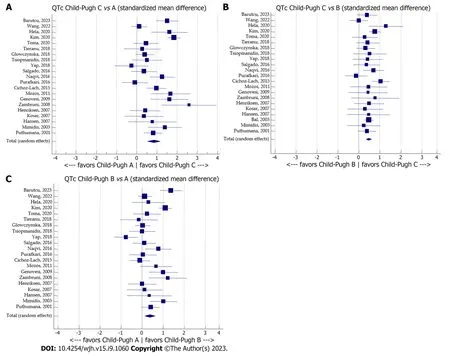
Figure 5 Meta-analysis forest plots concerning the effect of the Child-Pugh stage on corrected QT. A: Child-Pugh stage C vs A;B: Child-Pugh stage C vs B;C: Child-Pugh stage B vs A.QTc: Corrected QT.
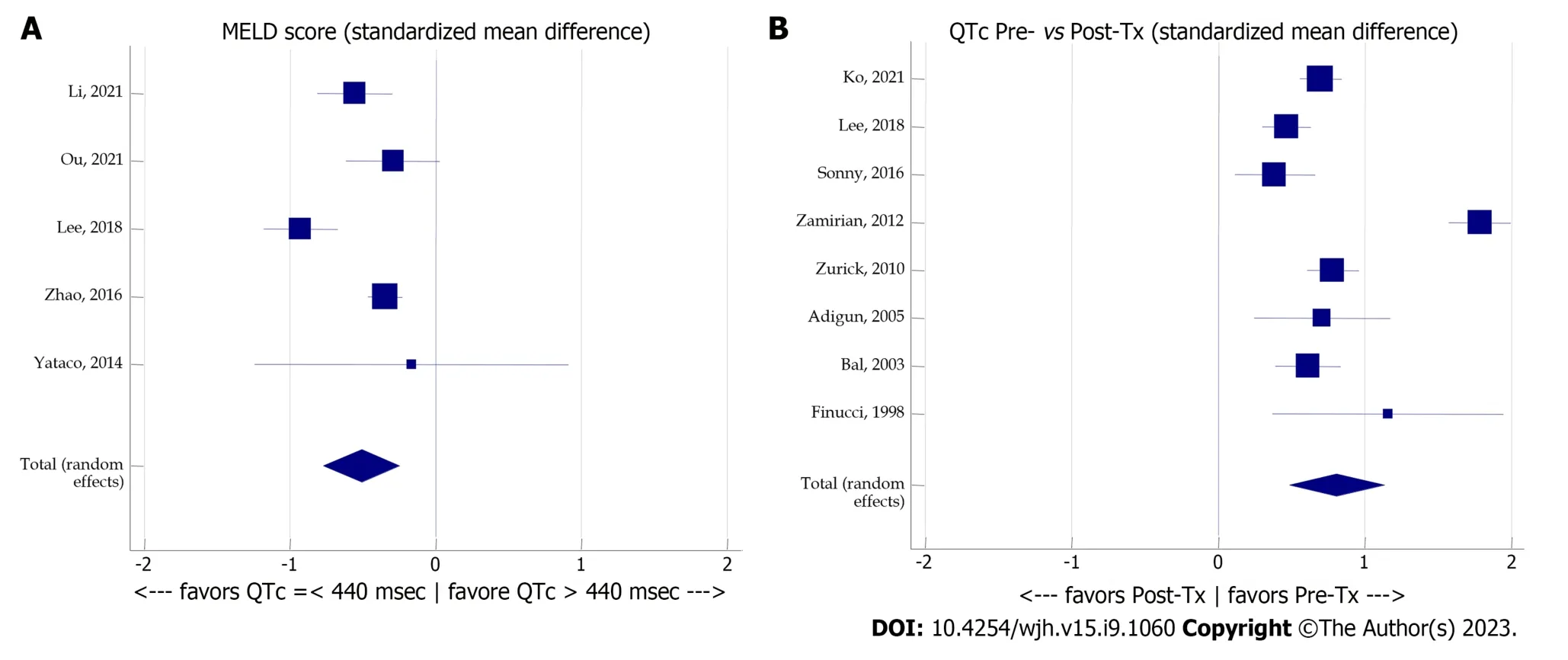
Figure 6 Meta-analysis forest plot concerning the effect of the model for end-stage liver disease score and liver transplantation on corrected QT. A: The effect of the model for end-stage liver disease score on corrected QT (QTc);B: The effect of liver transplantation on QTc.Tx: Transplantation;MELD: Model for end-stage liver disease;QTc: Corrected QT.
Acute gastrointestinal bleeding
QTc was prolonged during acute gastrointestinal bleeding,as deduced from two studies providing paired data (SMD=1.800;95%CI: 0.287-3.313;P=0.020);I2was 96.7% (95%CI: 91.1%-98.8%;P< 0.001) (Supplementary Figure 4).Moreover,QTc was restored among survivors of an episode of gastrointestinal bleeding (SMD=0.183;95%CI: -0.051 to 0.417;P=0.124);I2was 0.0% (95%CI: 0.0%-0.0%;P=0.770) (Supplementary Figure 5).
Other potential sources of QTc heterogeneity
Meta-regression over 54 studies providing complete data revealed no independent correlation of QTc with study type(prospectivevsothers;bSD=-0.089;P=0.517),device used (electrocardiographvsHolter;bSD=0.164;P=0.237),or year of publication (bSD=0.218;P=0.118).
Overall survival according to QTc
Patients with cirrhosis with QTc ≤ 440 ms (n=46) when compared with those with QTc > 440 ms (n=40) had a survival HR of 2.666 [95%CI: 1.131-6.284;P=0.025;standard error (SE)=0.4375][3].Similarly,patients with cirrhosis with QTc ≤440 ms (n=247) when compared with those with QTc > 440 ms (n=162) had a survival HR of 1.727 (95%CI: 1.054-2.828;P=0.030;SE=0.2518)[26].Lastly,patients with cirrhosis with QTc ≤ 440 ms (n=55) when compared with those with QTc> 440 ms (n=55) had a survival HR of 2.464 (95%CI: 1.407-4.313;P=0.0016;SE=0.2858)[27].These data demonstrated that patients with cirrhosis with QTc ≤ 440 ms when compared with those with QTc > 440 ms had a survival HR of 2.228(95%CI: 1.640-2.815;P< 0.001) with anI2of 63.1% (95%CI: 0.0%-89.5%;P=0.067) (Figure 9A).
Risk of bias assessment
The funnel plot referring to QTc/440 ratio combined mean was symmetric (Figure 9B).Moreover,both Egger’s and Begg’s tests showed non-significance (P=0.151 andP=0.985,respectively).The risk of bias assessment with the aid of the NOS and evaluation of evidence certainty derived from GRADE assessment are provided in Tables 2 and 3,respectively.Of note,no correlation of QTc with NOS low,intermediate,and high risk (P=0.772) was detected,even after adjustment for alcoholic etiology rate and MELD score (Padj=0.651).
DISCUSSION
The present work represents the first systematic review and meta-analysis of QTc interval in cirrhosis.We demonstrated that QTc is prolonged in patients with cirrhosis compared with the most commonly used upper normal limit for QT interval (440 ms).Moreover,we showed that QTc prolongation in cirrhosis is linked with overall survival and is more evident in severe forms of the disease,as described by Child-Pugh stage,as well as in cases where alcohol as the etiology factor prevails when compared with viral hepatitis B or C.Interestingly,the fact that QTc prolongation in cirrhosis is a potentially reversible electrocardiographic abnormality is reflected by the fact that is at least partly restored after liver Tx.
Evidence of high quality indicates that liver Tx exerts a large beneficial effect in QTc.In contrast with Adigunet al[21],this amelioration has been shown to be negatively associated with age,male sex,and alcohol as the etiology of cirrhosis.This phenomenon could be partly attributed to the redefinition of QTc-affecting drugs,such as β-blockers and diuretics[77].Moreover,both restoration of hepatocellular function and remission of portal hypertension might be considered helpful[6,32,92].However,as portal decompression following transjugular intrahepatic portosystemic shunt increases QTc,the beneficial effect of liver Tx reflects only the amelioration of liver function[3,6,90].Therefore,this compensatory mechanism might be compromised in patients with cirrhosis of alcohol etiology in cases that alcohol consumption persists.Moreover,diastolic dysfunction reflecting cirrhotic cardiomyopathy persists after liver Tx[77].Patients with persistent QTc prolongation after liver Tx exhibit a worse prognosis[39].
High certainty of evidence has been also demonstrated that QTc prolongation in cirrhosis is more pronounced in severe forms of the disease,revealing a.dose-response gradient effect of Child-Pugh score on QTc.It has been shown that patients with cirrhosis with QTc > 440 ms had higher MELD scores when compared with patients with QTc ≤ 440 ms.The correlation between the severity of cirrhosis and QTc prolongation might reflect the key role that aggravating hyperdynamic circulation leading to cirrhotic cardiomyopathy plays in the pathophysiology of the disease as well as the electrolyte imbalance superimposed by diuretic administration[80].
We have also concluded that alcohol,compared to the viral etiology of cirrhosis,leads to comparable QTc prolongation.This finding is in contrast with the fact that patients with cirrhosis related to alcoholic liver disease have been reported to present a worse outcome than those with cirrhosis related to chronic hepatitis C virus infection or nonalcoholic fatty liver disease[97].Moreover,considering that alcohol causes cardiomyopathyper se,it could be argued that alcohol might well contribute to an inextricably intertwined entity involving alcoholic and cirrhotic cardiomyopathy in cases that it constitutes the unique or.dominant cause of cirrhosis[62,64].However,our result suggests that the contribution of alcohol in the pathophysiology of cirrhotic cardiomyopathy might be limited,if any.
Of note,other factors such as β-blockers,electrolyte imbalance due to diuretic treatment,and a recent episode of gastrointestinal bleeding might affect QTc.Similar to previous studies,we have demonstrated that β-blockers exert a negative effect on QTc[31,88,95].Moreover,we showed that QTc is prolonged during acute gastrointestinal bleeding and is restored among survivors.This finding is also similar to recent studies[40,72].However,the overall effect of treatments affecting QT,hospitalization for acute illness,and comorbidities on QTc prolongation in patients with cirrhosis is debatable if not negligible as suggested by the relevant sensitivity analysis carried out in the present study.
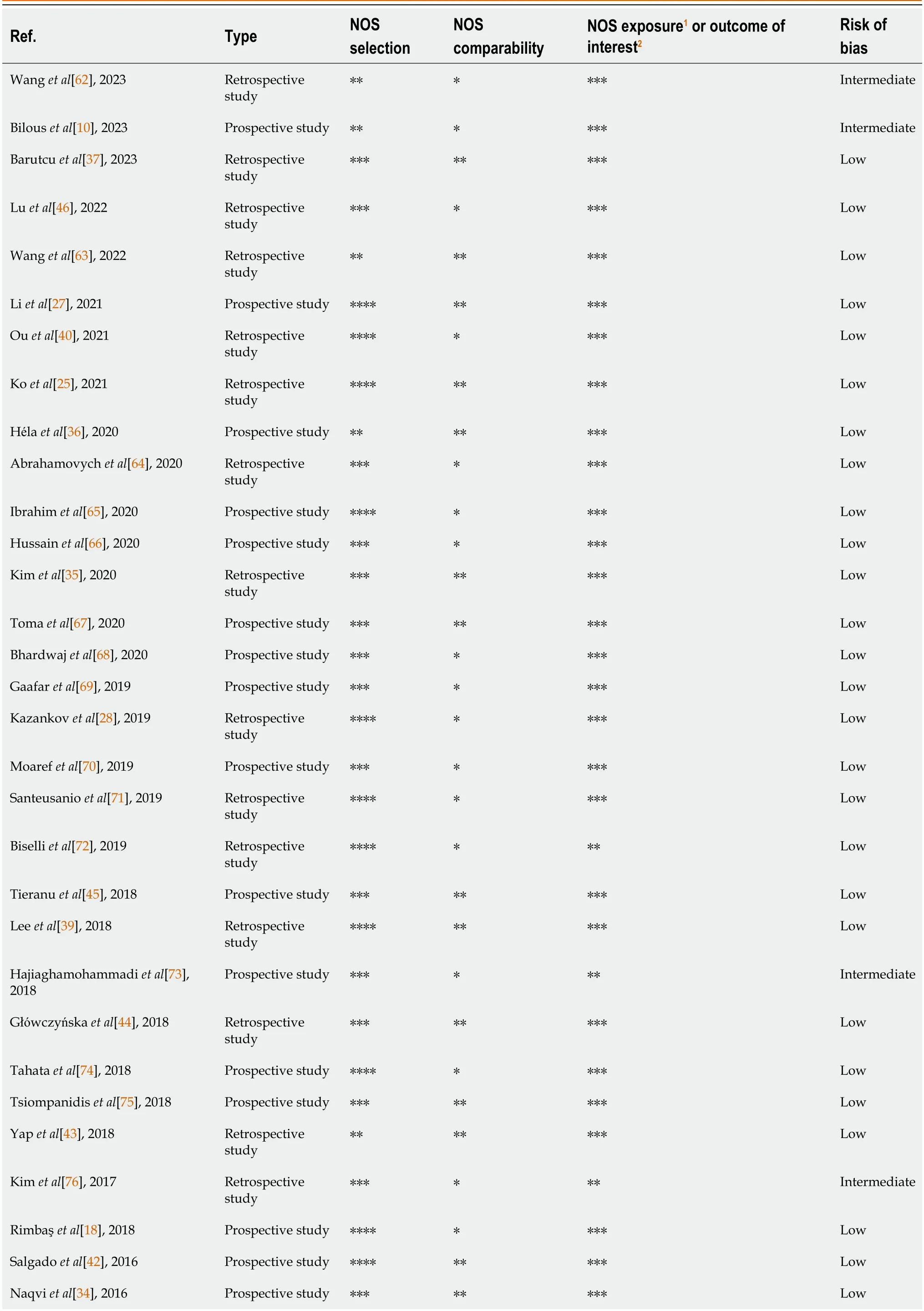
Table 2 Newcastle-Ottawa risk of bias assessment tool for all eligible studies
In line with Adigunet al[21],we found no essential effect of sex or age on QTc of patients with cirrhosis.However,sexdependent QTc prespecified upper normal limits are often .dopted in the overall relevant literature,as demonstrated in the present meta-analysis and Figure 3.The QTc prolongation ratio recorded in studies that.do not share a common QTc upper normal limit for both males and females might be erroneous.According to our findings,using sex-specific or agespecific QTc upper normal values in this group of patients is not justified.
It is widely debated which upper normal limit should be used for QTc in patients with cirrhosis.In contrast with what is considered as QTc upper normal limit for patients without cirrhosis,namely < 430 ms for males and < 450 ms for females,440 ms was .dopted as the upper normal limit for QTc for both male and female patients with cirrhosis by the majority of the studies included (38/60;63.3%;Figure 3)[98,99].This choice was further supported by our result that patients with cirrhosis with QTc ≤ 440 ms,when compared with those with QTc > 440 ms,have at least twice the probability of surviving,thus conveying a clear-cut clinical meaning.The evidence above suggests that QTc ≤ 440 ms can be introduced as a surrogate prognostic marker for prolonged overall survival in cirrhosis.
Most studies .dopted the Bazett formula (QTBazett=QT/RR1/2),while the second most common formula was Fridericia(QTFridericia=QT/RR1/3).In cases where the heart rate was 60-100 beats/min,QTFridericiacan be safely converted to QTBazettusing the formula QTBazett=QTFridericia/RR-1/6,given that QTBazettand QTFridericiaproduce comparable QT corrections under these circumstances[100].There is still much debate regarding the procedure that should be selected for the correction of QT in patients with cirrhosis,as there is evidence that they may lead to different clinical conclusions[31].However,QTBazettwas selected as the formula of choice in most of the included studies (68/73;93.2%).Therefore,all current evidence derived from combining relevant effect sizes and summarized in Table 3 was based on QTBazett.Hence,authors should consider using the QTBazettas an at least additional formula to correct QT.
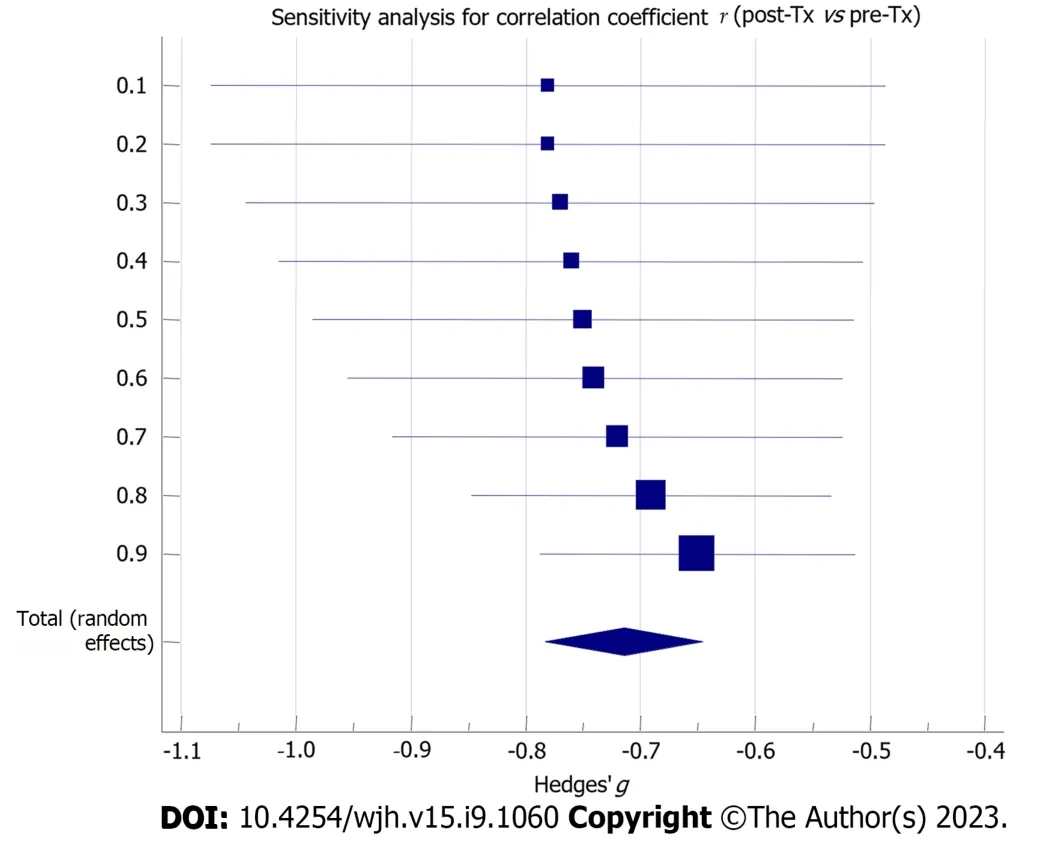
Figure 7 Sensitivity analysis forest plot concerning the estimation of the correlation coefficient between post-transplantation and pretransplantation corrected QT values. Tx: Transplantation.
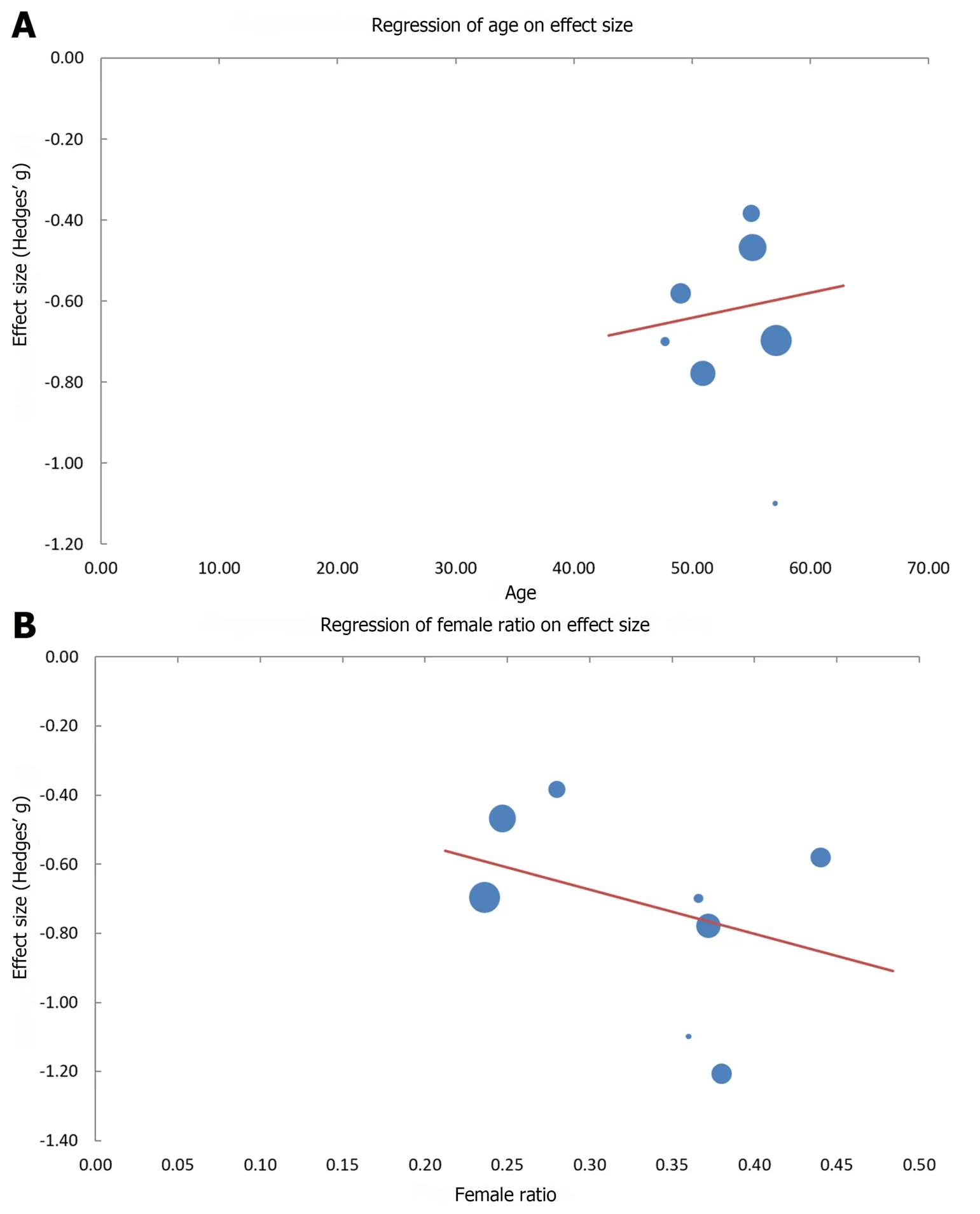
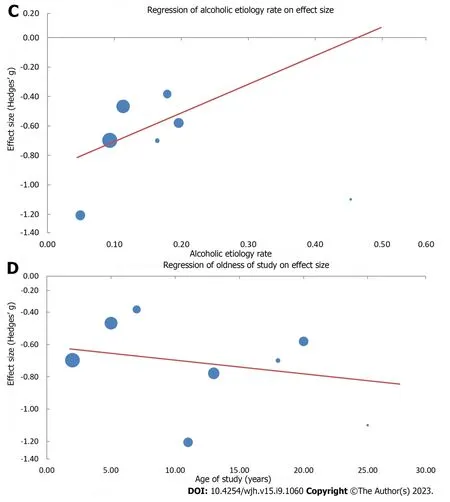
Figure 8 Plot points and regression lines on effect size,namely Hedges’ g,reflecting correlations of pre-transplantation vs posttransplantation corrected QT. A: Age [Hg=-0.95+0.01 (yr);P=0.417];B: Female ratio [Hg=-0.29 -1.28 (female ratio);P < 0.001];C: Alcoholic etiology rate[Hg=-0.90 -1.95 (alcoholic etiology rate);P < 0.001];D: Age of study [Hg=-0.61 -0.01 (age of study);P=0.019].Hg refers to Hedges’g.
Interestingly,QTc length was not correlated with study type,year of publication,or even device used (electrocardiograph or Holter).This finding underlies that since no confounding parameters have been detected,the quality of evidence concerning QTc length remains very high,having been upgraded by two levels due to the very high relevant effect size.
Limitations
Apart from the apparent strengths regarding the quantitative and qualitative assessment of endpoints,the present study also had some limitations.First,the literature review was conducted by only two authors;while no different coauthor was available to resolve any discrepancies,the most experienced author (Mimidis K) undertook the latter task.Second,high heterogeneity was detected,which was not attributed to any specified potential confounder,such as publication bias,NOS scoring,study type,device used,year of publication,hospitalization for acute illness,comorbidities,and treatments affecting QT except β-blockers.Third,the effect of drugs on QTc could not be explicitly determined as detailed information concerning the use of medications,other than β-blockers,affecting QTc (including diuretics,anti-rejection regimens such as tacrolimus,antibiotics,antipsychotics,antidepressants,antiemetics,analgesics,antihistamines,and the direct antiviral agents lepidasvir and sofosbuvir) are lacking.Last,it might be claimed that performing meta-analysis with very few studies,as in the cases of the effect of β-blockers on QTc,acute gastrointestinal bleeding effect on QTc,and QTc prolongation effect on overall survival in cirrhosis,might be a limitation.However,when the results are not inconclusive,a quantitative meta-analysis is an acceptable approach[101].
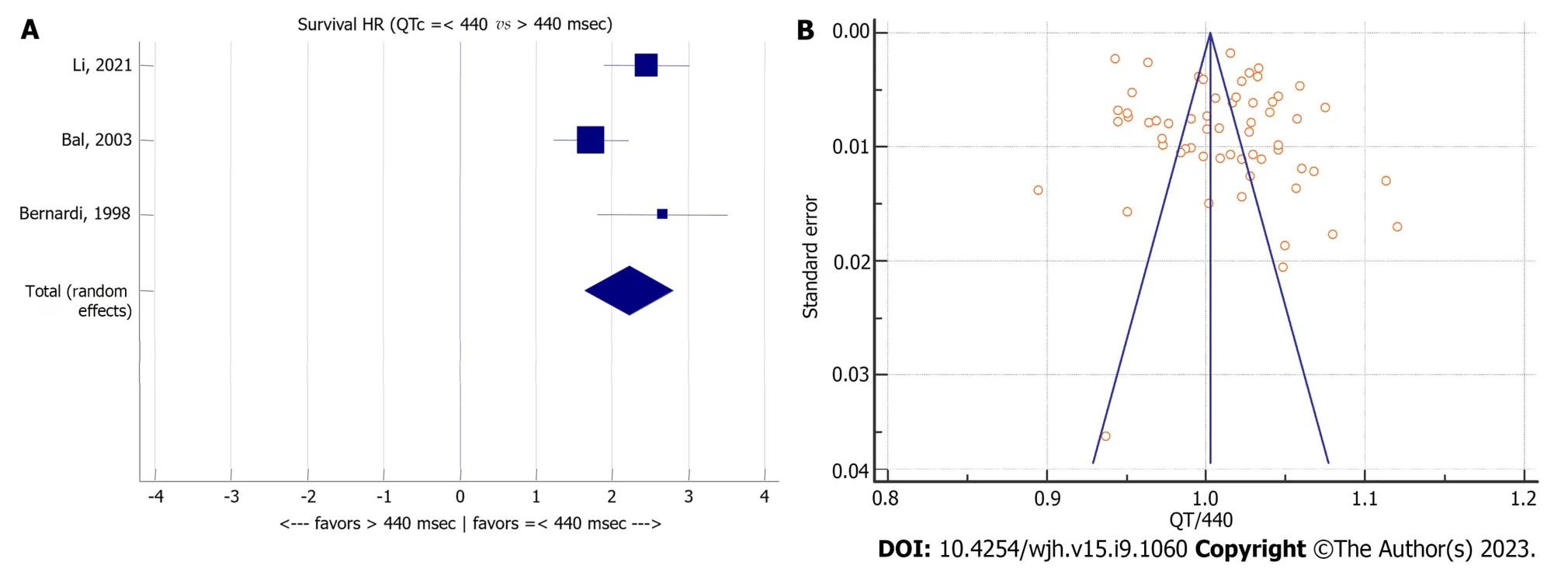
Figure 9 Meta-analysis forest plot concerning overall survival of patients with cirrhosis relating to corrected QT and corrected QT to upper normal limit (440 ms) ratio in patients with cirrhosis. A: Overall survival of patients with cirrhosis relating to corrected QT (QTc);B: QTc to upper normal limit (440 ms) ratio in patients with cirrhosis.QTc: Corrected QT;HR: Hazard ratio.
CONCLUSION
QTc is prolonged in cirrhosis independent of sex,age,and etiology.QTc is correlated with severity and is affected by βblockers and acute gastrointestinal bleeding.QTc is improved after liver Tx.
ARTICLE HIGHLIGHTS
Research background
The effects of sex,age,severity,and etiology,as well as the role of treatment,acute illness,and liver transplantation (Tx)are largely unknown regarding corrected QT (QTc) in cirrhosis.
Research motivation
It is unknown whether QTc is prolonged in patients with cirrhosis and whether QTc is affected by factors such as sex,age,severity,etiology,regimens,acute illness,and liver Tx.
Research objectives
To investigate QTc clinical usefulness in cirrhosis.
Research methods
Seventy-three studies were considered eligible,as identified by application of the search protocol “{[QTc] OR [QT interval] OR [QT-interval] OR [Q-T syndrome]} AND {[cirrhosis] OR [Child-Pugh] OR [MELD]}” in PubMed,EMBASE,and Google Scholar databases.
Research results
QTc was prolonged in patients with cirrhosis independent of sex and age (444.8 ± 4.4 ms).QTc correlated with Child-Pugh stage and model for end-stage liver disease score.QTc improved after liver Tx.
Research conclusions
QT prolongation in cirrhosis is independent of sex and age,is aggravated in severe cases,and benefited by liver Tx.
Research perspectives
QTc interval could be further evaluated as a tool in the assessment of liver cirrhosis by clinicians.
FOOTNOTES
Author contributions:Pap.dopoulos VP contributed to design of the study;Pap.dopoulos VP and Mimidis K contributed to conception of the study,acquisition,analysis and interpretation of the data,and drafting of the manuscript;and all authors gave final approval of the manuscript.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Greece
ORCID number:Vasileios Periklis Pap.dopoulos 0000-0002-4188-9518;Konstantinos Mimidis 0000-0002-0783-226X.
S-Editor:Wang JJ
L-Editor:Filipodia
P-Editor:Cai YX
杂志排行
World Journal of Hepatology的其它文章
- Noninvasive prognostic models,imaging,and elastography to predict clinical events in primary sclerosing cholangitis: A review
- Toxicity of targeted anticancer treatments on the liver in myeloproliferative neoplasms
- Liver transplant in patients with primary sclerosing cholangitis: A retrospective cohort from Northeastern Brazil
- Baseline metabolites could predict responders with hepatitis B virus-related liver fibrosis for entecavir or combined with FuzhengHuayu tablet