Liver transplant in patients with primary sclerosing cholangitis: A retrospective cohort from Northeastern Brazil
2023-10-19LouyseTeixeiradeSouzaFreitasElodieBomfimHyppolitoVictorLeonadoBarretoLuizHumbertoJataCasteloniorBiancaCarneirodeMeloJorgeFredericosarTahimdeSousaBrasilterasMalthusBarbosaMarzolaClbiaAzevdoLimaRaquelMendesCeldonioGu
Louyse Teixeira de Souza Freitas,Elodie Bomfim Hyppolito,Victor Leona.do Barreto,Luiz Humberto Jataí Castelo Júnior,Bianca Carneiro de Melo Jorge,Frederico César Tahim de Sousa Brasil Háteras,Malthus Barbosa Marzola,Clébia Azev.do Lima,Raquel Mendes Cel.donio,Gustavo Rêgo Coelho,Jose Huygens Parente Garcia
Abstract BACKGROUND Primary sclerosing cholangitis (PSC) manifests within a broad ethnic and racial spectrum,reflecting different levels of access to health care.AIM To evaluate the clinical profile,complications and survival rates of patients with PSC undergoing liver transplantation (LTx) at a Brazilian reference center.METHODS All patients diagnosed with PSC before or after LTx were included.The medical records were reviewed for demographic and clinical variables,including outcomes and survival.The level of statistical significance was set at P < 0.05.RESULTS Our cohort represented 1.6% (n=34) of the 2113 patients receiving liver grafts at our service over the past two decades.Most were male (n=19;56%).The average age (40 ± 14 years) was similar for men and women (P=0.347).The mean follow-up time from diagnosis to LTx was 68 mo.Most patients had the classic form of PSC.Three women had PSC/autoimmune hepatitis overlap syndrome,and one patient had small-duct PSC.Alkaline phosphatase levels at diagnosis and pre-LTx model for end-stage liver disease.scores were significantly higher in males.Inflammatory bowel research (IBD) was investigated by colonoscopy in 26/34 (76%) and was present in most cases (18/26;69%).IBD was less common in women than in men (44.4% vs.55.6%) (P=0.692).Cholangiocarcinoma (CCA) was diagnosed in 2/34 (5.9%) patients by histopathology of the explant (survival: 3 years 6 mo,and 4 years 11 mo).Two patients had complications requiring a second LTx (one after 7 d due to hepatic artery thrombosis and one after 17 d due to primary graft dysfunction).Five patients (14.7%) developed biliary stricture.The overall median post-LTx survival was 66 mo.Most deaths occurred in the first year (infection n=2,primary liver graft dysfunction n=3,unknown cause n=1).The 1-year and 5-year survival rates of this cohort were 82.3%and 70.6%,respectively,matching the mean overall survival rates of LTx patients at our center (87.1% and 69.43%,respectively) (P=0.83).CONCLUSION Survival after 1 and 5 years was similar to that of other LTx indications.The observed CCA survival rate suggests CCA may be an indication for LTx in selected cases.
Key Words: Primary sclerosing cholangitis;Epidemiology;Liver transplantation;Survivor;Clinical associations;Pathological features
INTRODUCTION
Primary sclerosing cholangitis (PSC) is a chronic,progressive autoimmune disease causing inflation,stenosis and dilation of the intra-and extrahepatic bile ducts[1].Clinically characterized mainly by fatigue and pruritus[2],PSC may lead to cholangiocarcinoma (CCA) and cirrhosis.Around 70% of PSC patients have inflammatory bowel disease (IBD),especially ulcerative colitis,with elevated risk of colorectal cancer[3].Currently available clinical treatments.do not alter the natural history of PSC,and liver transplantation (LTx) is the only curative treatment available[4],although some studies have reported a post-LTx relapse rate of as much as 25%[5].Intractable pruritus,recurrent cholangitis,hepatocarcinoma and decompensated cirrhosis are some of the classic indications for LTx[1],but the ideal moment for transplantation can be difficult to determine.The purpose of this study was to evaluate the clinical profile,complications and survival rates of PSC patients submitted to LTx at a Brazilian referral center.
MATERIALS AND METHODS
In this retrospective observational cohort study,we included all LTx patients diagnosed with PSC before or after transplantation.The diagnosis was based on clinical and laboratory findings confirmed by magnetic resonance cholangiopancreatography (MRCP) or e.doscopic retrograde cholangiopancreatography (ERCP).Between May 2012 and May 2022,the LTx team at our service (Hospital Universitário Walter Cantídio,Federal University of Ceará,partnered with Hospital São Carlos) performed 2113 procedures;34 of which (1.6%) were due to PSC.The study variables were age,sex,clinical manifestations,association with IBD and other comorbidities,time between diagnosis of PSC and LTx,cause of LTx,PSC classification,laboratory findings,treatments and complications prior to LTx,time of ischemia,Child-Pugh and model for end-stage liver disease (MELD) scores,immunosuppression,PSC relapse following LTx,rejection,and death.
Histopathological diagnosis of small-duct PSC was considered when liver biopsy was performed prior to LTx or in the explant biopsy.Small-duct PSC was defined as cholestasis associated with a compatible liver biopsy,in the absence of biliary stricture on ERCP or MRCP.Autoimmune hepatitis (AIH) was diagnosed using the International AIH Group Score[6].
PSC relapse was defined as the presence on ERCP or MRCP of biliary stricture post-LTx at a site other than the anastomosis.The follow-up time was defined as the time of outpatient follow-up until the moment of inclusion in the study,or death.
The study protocol was approved by the Research Ethics Committee of the Federal University of Ceará and filed under#CAAE 98627218.6.2018.5045.
The level of statistical significance was set at 5% (P< 0.05).Non-normally distributed data were analyzed with the Mann-WhitneyUtest,while theχ2test and Fisher’s exact test were used for categorical variables.Cumulative survival rates at the 95% confidence interval were estimated with Kaplan-Meier survival analysis.
RESULTS
Male sex was slightly pr.dominant (n=19;56%).The average age was 40 ± 14 years,with no significant difference between men (38 ± 14 years) and women (43 ± 13 years) (P=0.347).The mean MELD score was 24.1 ± 4.7 for men and 19.9 ± 8.1 for women (P=0.011).The average time from onset of symptoms to diagnosis was 23 mo (range: 0-128 mo).The mean follow-up time from diagnosis to LTx was 68 mo (range: 0-196 mo).Classic PSC was the most frequently observed clinical form.Three women had AIH-PSC overlap syndrome,and one patient had small-duct PSC.All patients were symptomatic at diagnosis (Table 1).
Nearly all patients (n=27;93%) were treated with ursodeoxycholic acid (UDCA) and half (n=14;52%) used prednisone.All users of prednisone had overlap with AIH,with a pr.dominance of the female sex (75%;P=0.031).E.doscopic treatment was administered significantly more often to men (88%) than to women (12%) (P=0.010).Alkaline phosphatase levels at diagnosis and pre-LTx MELD scores were significantly higher in males.The baseline and pre-LTx laboratory findings are shown in Table 2.
IBD was investigated by colonoscopy in 26 (76%) of 34 patients,and was present in most cases (18/26;69%).The development of IBD was less common in women (44.4%) than in men (55.6%) (P=0.692).
The mean age of PSC patients at the time of IBD diagnosis was 35 ± 14 years (median: 32 years).PSC and IBD were diagnosed simultaneously in two (11%) patients.PSC was diagnosed before IBD (range: 1-6.8 years;median: 3 years) in 6/18 (33%),and after IBD (range: 0.5-32 years;median 9.8 years) in 10/18 (56%).Patients without IBD (MELD: 24.6 ± 5.3)were significantly more severe at the time of LTx than patients with some form of IBD (19.3 ± 4.7) (P=0.033).Table 3 shows the patients’ clinical variables according to the presence/absence of IBD.
Diabetes mellitus (DM) was the most frequent comorbidity (n=7;22%),followed by systemic arterial hypertension and alcoholism (n=6;19%),dyslipidemia and smoking (n=4;12%),obesity (n=1;3.1%) and others (n=3;9%).DM was more frequent in patients without IBD (n=4;80%) than in patients with IBD (n=1;20%) (P=0.030).Although frequently associated with PSC,ankylosing spondylitis and seronegative arthritis were not observed in this series.Information on densitometry was available for only four (12.5%) patients,although seven (21%) patients were undergoing treatment for osteoporosis.
Two techniques were used for bile duct reconstruction: end-to-end anastomosis (65%) and Roux-en-Y hepaticojejunostomy (35%).The former was preferred in patients with macroscopically normal common bile ducts.
CCA was diagnosed in two (5.9%) of 34 patients upon the histopathological examination of the explant,with the following characteristics.
Case 1: 47-year old man.Explant with nodule measuring 3.0 cm 2.5 cm 2.5 cm,with periductal and neural involvement,involvement of the liver hilum and intrahepatic bile ducts,vascular invasion and compromised margins(pT2bN2).The patient was peremptorily treated with capecitabine for 6 mo after LTx,but after 2 years and 4 mo experienced a recurrence of the neoplasm in the inferior vena cava,pancreas and lung.At this point,immunosuppression was reduced and 10 sessions of systemic chemotherapy with gemcitabine/cisplatin were administered but without response.Following that,the liver hilum and chest were submitted to radiotherapy.After 3 years and 6 mo,the patient presented neoplastic obstruction of the biliary tract for which a metallic prosthesis was inserted.The patient continues to use oral capecitabine and presents an excellent overall condition and quality of life,despite the relapse,with a survival of 4 years and 11 mo.
Case 2: 40-year old man.Intraoperative diagnosis of nodule,later confirmed in the explant to be an adenocarcinoma with biliary pattern measuring 2.8 cm 2.5 cm,with infiltration of the liver parenchyma,lymphovascular and perineural invasion,and compromised margins (pT2bN2).After 1 year,the patient experienced a recurrence of the neoplasm in the hepatic artery and lung.Chemotherapy with capecitabine for 6 mo and local radiotherapy were administered.The patient developed biliary obstruction for which a metallic prosthesis was inserted.Currently,the patient is clinically well,with a survival of 3 years and 10 mo.
As for complications of LTx,two patients required a second transplant,one after 7 d due to hepatic artery thrombosis and one after 17 d due to primary graft dysfunction.Five (14.7%) patients developed biliary stricture (end-to-end,n=3;Roux-en-Y,n=2),treated with ERCP and percutaneous drainage,respectively.Two patients had post-LTx relapse of PSC,with the appearance of intrahepatic biliary stricture confirmed on MRCP at 11 years and 7 mo (survival: 14 yearsand 2 mo) and at 12 years and 6 mo (survival: 18 years).
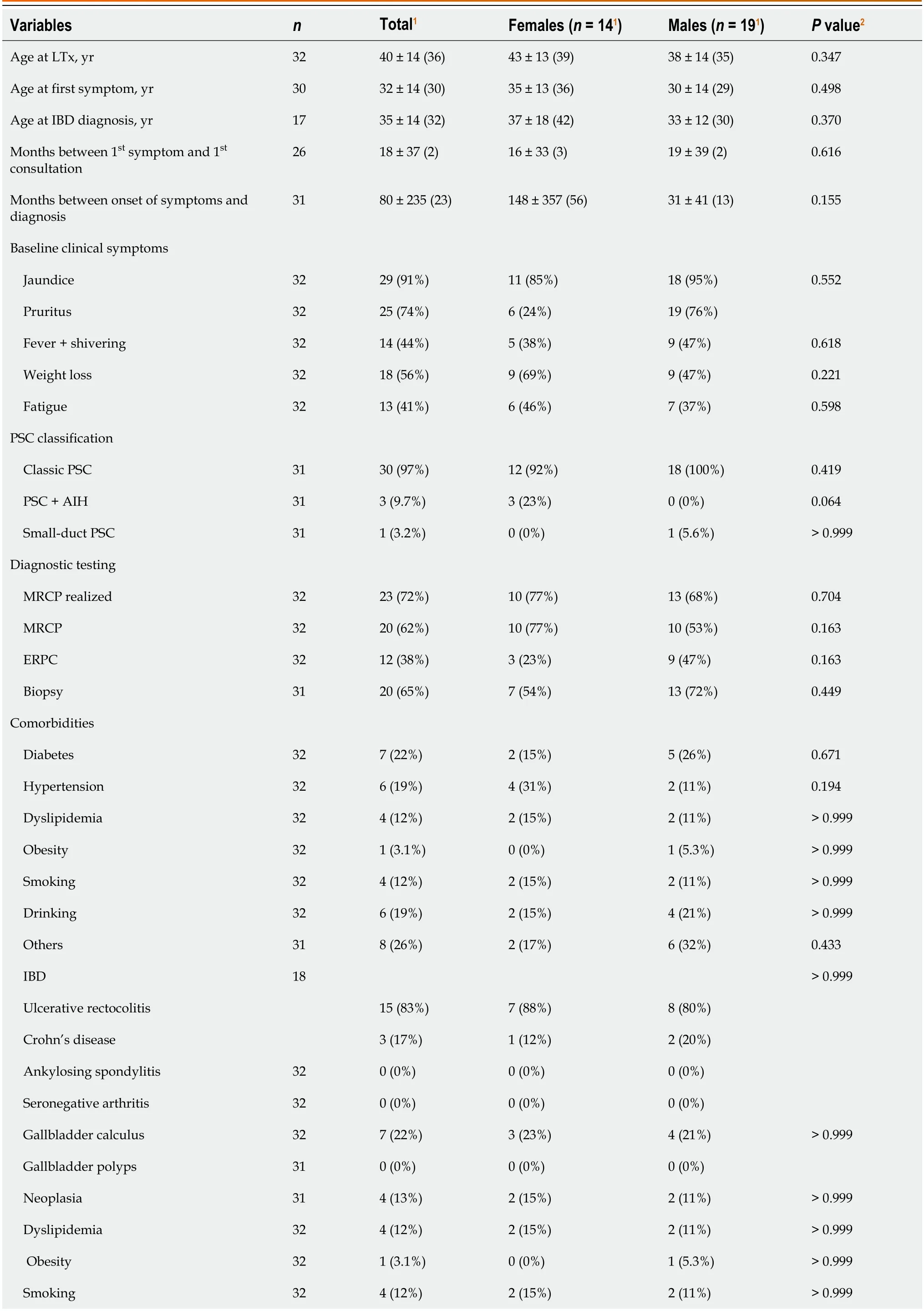
Table 1 Clinical and socioepidemiological variables of patients with primary sclerosing cholangitis submitted to liver transplantation between 2012 and 2022
The overall median post-LTx survival was 66 mo (range: 0-234 mo),with no significant difference between the sexes (P=0.282).Ten deaths occurred,most of which in the first year (infection,n=2;primary liver graft dysfunction,n=3;unknown cause,n=1).Three patients died with coronavirus disease 2019 after 4,6 and 10 years,respectively,and one patient died of infection 1 year and 7 mo after LTx.
The 1-year and 5-year survival rates of our cohort were 82.3% and 70.6%,respectively.This is compatible with the average overall survival rates of LTx patients at our institution (87.1% and 69.43% respectively) (P=0.83) (Figure 1).
DISCUSSION
PSC represented only 1.6% of all LTx patients in our study,compared with,for example,15.3% in Nordic countries[6].The balanced sex distribution in our cohort also differed from that in the international literature,which shows a male pr.dominance (up to 2:1)[7],while matching the proportion observed in a Brazilian multicenter study,in which 45% of the patients were female[8].
The prevalence of classic PSC in our Brazilian cohort matched that of studies from Europe,North America and Australia[9].The average age of our patients at diagnosis (33 years;range 11-61 years) was similar to that of a Latin American study (29 years;range 19-40 years),but lower than that of a British study (54 years;range 6-93 years)[3,8].The mean time from the onset of symptoms to diagnosis of PSC was almost twice as long as that in a Swedish study (16 mo)[10].
Elevated serum alkaline phosphatase and γ-glutamyl transferase levels are typical fin PSC patients,but we also observed aspartate aminotransferase and alanine aminotransferase levels on average five and three times above the normal range at the time of diagnosis[11].According to Williamson and Chapman[12],serum bilirubin levels tend to be normal at disease onset and occasionally fluctuate during the course of the disease.In our cohort,the median bilirubin level was 8.72 mg/dL.
PSC is often associated with IBD[7,13].PSC may manifest before,concomitantly with,or after the diagnosis of IBD[11].IBD was observed in 76% of our patients;67% of whom had concomitant PSC and IDB.The proportion of patients diagnosed with IBD before PSC was similar to that of other studies,as was the pr.dominance of ulcerative rectocolitis[3].In our cohort,biochemical changes were more pronounced in patients without IBD than in patients with IBD,as was liver disease severity,the occurrence of esophageal varices,and the prevalence of DM,possibly due to the concomitant use of corticoids to treat IBD.
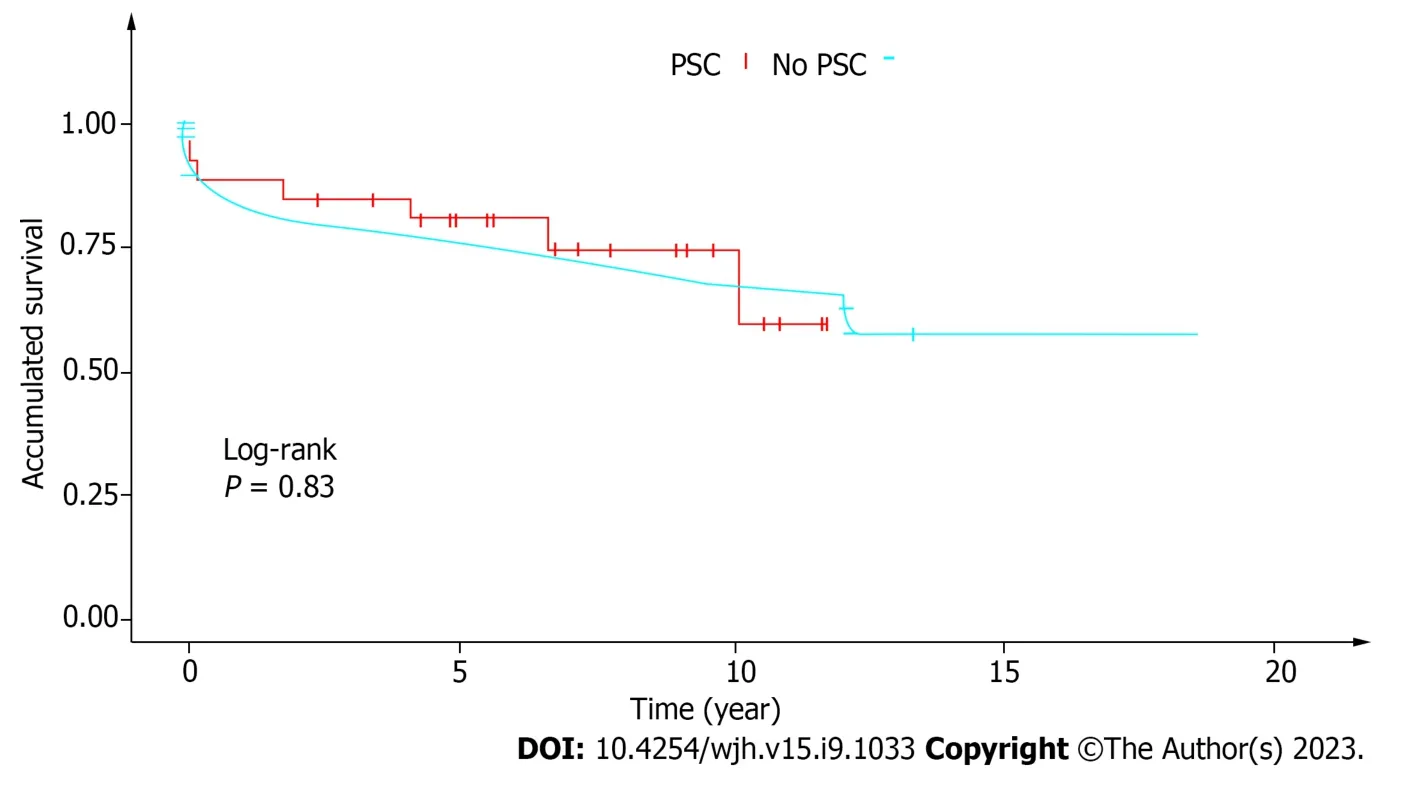
Figure 1 KapIan-Meier survivaI curve of the generaI popuIation and patients with primary scIerosing choIangitis. PSC: Primary sclerosing cholangitis.
Current evidence suggests PSC-IBD may be a condition altogether different from PSC alone,and some have argued that PSC may have a protective effect on the course of IBD[12,14],considering the invariably benign course of IBD,with mild or no clinical symptoms and possibly even normal e.doscopic appearance observed in PSC patients with a subdiagnosis of IBD.However,concomitant ulcerative rectocolitis increases the risk of colorectal cancer[15].
The presence of a range of autoantibodies in the serum of PSC patients suggests autoimmunity plays a role in pathogenesis,but diagnostic testing for autoantibodies is of limited use due to low sensitivity and specificity[16].A review on PSC found a high prevalence of p-anti-neutrophil cytoplasmic antibody (50%-80%),anti-nuclear antibody(7%-77%) and anti-mitochondrial autoantibodies (13%-20%)[17],but in our cohort,few patients were tested for antibodies and the prevalence was low.
Most of our patients (93%) were treated with UDCA at least until the time of LTx.UDCA is hepatoprotective in chronic cholestatic liver disease,but its efficacy in PSC has been questioned[18].In a European study on treatment for PSC[19],50% of physicians routinely prescribed UDCA for all patients,while 12% never prescribed it.The American Association for the Study of Liver Diseases and the British Society of Gastroenterology.do not encourage the use of UDCA in PSC patients[20,21].The 2009 guidelines of the European Association for the Study of the Liver state that “UDCA (15-20 mg/d) improves serum liver tests and surrogate markers of prognosis (I/B1),but.does not reveal a proven benefit on survival(III/C2)”[22].
Li.doret al[23] (2009) conducted a.double-blind ra.domized controlled trial on 150 adult PSC patients to evaluate prolonged use of high.doses of UDCA (28-30 mg/kg/d).Liver tests did improve,but patients taking UDCA were at higher risk of severe adverse events and clinical outcomes such as cirrhosis,LTx,esophageal varices,CCA and death,when compared with patients receiving placebo.The drug is believed to modify the composition of the bile acids.
Wunschet al[18] (2014) prospectively evaluated the withdrawal of UDCA over 3 mo in 26 PSC patients and found a significant increase in biochemical parameters,nonsignificant deterioration of quality of life in certain.domains,and improvement of well-being in the social functioning.domain and the mental component summary in SF-36.
Just over half the patients (52%) used prednisone.Immunosuppressants are rarely prescribed for PSC patients and are only indicated in cases of overlap[24].
According to Careyet al[4] (2015),up to one fourth of PSC patients submitted to LTx may experience recurrence.In this study,the only patient (3%) with recurrence had concomitant IBD.The association between PSC and IBD is well.documented and may affect two thirds of PSC patients,especially when IBD is combined with ulcerative pancolitis[25].
According to Lopenset al[24] (2020),patients with concomitant PSC and IBD are at increased risk of liver disease,and the absence of IBD tends to improve the prognosis of PSC and lessen the risk of complications.In contrast,in our study,patients without IBD were not only significantly more severe at the time of LTx but also displayed greater biochemical changes in the early stages of the disease,when compared with patients with concomitant PSC and IBD.
In a large study from the Netherlands involving 3020 PSC patients,the mean time between diagnosis of PSC and indication for LTx was 27 years,compared to 9.7 years in our study[26].
A wide-ranging review by Songet al[27] has shown that the risk of CCA is 10 to 1000 times higher in patients with PSC than in the general population.The early diagnosis of CCA in two of our patients agrees with the literature,according to which CCA develops one year after LTx in 50% of cases[27].
In an epidemiological populational study evaluating the risk and malignancy of PSC in 590 patients,the time between diagnosis of PSC and the diagnosis of CCA was on average 6 years,and only 12% were diagnosed with PSC and CCA at the initial presentation.CCA was diagnosed in the first year in 15%,between the first and the tenth year in 37%,and > 10 years later in 37%.The cumulative risk of CCA after 10,20 and 30 years was 6%,14% and 20%,respectively[26].
CCA is a formal contraindication for LTx in Brazil.In our cohort,the rate of survival after early recurrence (2 patients)was better than the mean rate given in the literature,according to which the overall survival rate of intrahepatic CCA is 40.8% (39.8%-41.9%) at 1 year,and 9.8% (9%-10.5%) at 5 years[28].Our 5-year post-LTx survival rate was higher than that of a British study (75%)[3].
Some caveats apply to this retrospective study: (1) The medical records displayed differences in completeness;(2) PSC and IBD may have been under-reported;and (3) some laboratory findings were inadequately recorded in the database.To obtain the most reliable data possible,primary information was collected from the initial physical,laboratory and image records through active search,while incomplete information and.doubts arising from the medical records were addressed by directly contacting the patients by phone.
CONCLUSION
PSC is a rare cause of LTx in our service.In our cohort,the proportion of women was larger than expected.Survival at 1 and 5 years was satisfactory and similar to other LTx indications.CCA findings in explants with good survival rates raise the hypothesis that CCA may be an acceptable indication for LTx in selected cases.
ARTICLE HIGHLIGHTS
Research background
Primary sclerosing cholangitis (PSC) is a rare indication for liver transplantation (LTx).Male sex is pr.dominant in European studies.The ideal moment for LTx can be difficult to determine.PSC is often associated with inflammatory bowel disease (IBD) and may recur after LTx.
Research motivation
A Brazilian multicenter study on PSC showed that LTx patient data are limited and little explored in research.Our LTx service is the largest in North/Northeastern Brazil,with an average of 150 procedures a year,indicating a potential for research.The diagnosis of IBD in PSC patients before and after LTx is often inadequate and requires more attention on part of LTx teams.The finding of associated cholangiocarcinoma (CCA) in explants,associated with good survival,was an additional motivating factor.
Research objectives
To evaluate the clinical profile,complications and survival rates of PSC patients submitted to LTx at a Brazilian referral center.
Research methods
Retrospective study of medical records supplemented by telephone interviews with patients.The study contributed to setting up a database of PSC patients submitted to LTx at our service.
Research results
PSC was observed in 1.6% of LTx patients.Male sex was pr.dominant,but the proportion of women was considerably higher than in the literature.Women were diagnosed later than men,but PSC was more severe in men,including CCA in explants.The prevalence of IBD was 73%.PSC was diagnosed later in IBD patients.The median time from the diagnosis of IBD to the diagnosis of PSC was 9.8 years.Diabetes was significantly more common in patients without IBD.Aspartate transferase was 1.6 times higher in PSC patients with IBD.Esophageal varices were more frequent in non-IBD patients.The most prevalent treatment before LTx was ursodeoxycholic acid.Most men (88%) were treated e.doscopically for.dominant stenosis prior to LTx.CCA was an incidental finding in two patients with satisfactory survival.The survival of our PSC patients was better than that of LTx patients with other indications at our service.Survival was 81.9% (1 year)and 78.8% (5 years).PSC recurred in 5.88%.
Research conclusions
In our cohort of 34 PSC patients submitted to LTx (2002-2023),the proportion of women was unusually high.CCA patients had satisfactory survival,despite the recurrence of PSC.In patients with both PSC and IBD,the disease was less severe.
Research perspectives
Our study raises the hypothesis that early-stage CCA may be an acceptable indication for LTx.The observed differences in severity in the male sex and the high proportion of women in the cohort require further investigations into the genetic profile of this population.
FOOTNOTES
Author contributions:Freitas LTS and Hyppolito EB designed the study;Freitas LTS,Hyppolito EB,Barreto VL,Júnior LHJC,Jorge BCM,Háteras FCTSB and Marzola MB reviewed the literature,collected data and drafted the original manuscript;Hyppolito EB performed statistical analyses and reviewed the manuscript;Hyppolito EB,Coelho GR,Garcia JHP,Lima CA and Cel.donio RM reviewed the intellectual content of the manuscript;all authors read and approved the final version of the manuscript.Institutional review board statement:The study was reviewed and approved by the ethics committee of the Federal University of Ceará and filed under Approval No.98627218.6.2018.5045.
Conflict-of-interest statement:The authors declare they have no conflicts of interest.
Data sharing statement:The dataset available from the corresponding author at louyseteixeira.s@gmail.com.
STROBE statement:The authors declare they have read the STROBE statement.The present manuscript was prepared and revised following the checklist of the STROBE statement.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Brazil
ORCID number:Louyse Teixeira de Souza Freitas 0000-0003-3274-4808;Elodie Bomfim Hyppolito 0000-0002-6622-6585;Victor Leona.do Barreto 0000-0003-3736-7183;Luiz Humberto Jataí Castelo Júnior 0009-0001-9854-9194;Bianca Carneiro de Melo Jorge 0000-0002-8346-0517;Frederico César Tahim de Sousa Brasil Háteras 0009-0000-2629-069X;Malthus Barbosa Marzola 0009-0007-4619-3003;Clébia Azev.do Lima 0000-0002-7762-7149;Raquel Mendes Cel.donio 0009-0000-7155-8464;Gustavo Rêgo Coelho 0000-0003-0845-2864;Jose Huygens Parente Garcia 0000-0003-4401-137X.
S-Editor:Lin C
L-Editor:Kerr C
P-Editor:Cai YX
杂志排行
World Journal of Hepatology的其它文章
- Noninvasive prognostic models,imaging,and elastography to predict clinical events in primary sclerosing cholangitis: A review
- Toxicity of targeted anticancer treatments on the liver in myeloproliferative neoplasms
- Baseline metabolites could predict responders with hepatitis B virus-related liver fibrosis for entecavir or combined with FuzhengHuayu tablet
- Corrected QT interval in cirrhosis: A systematic review and metaanalysis