Myricetin alleviates ovalbumin-induced allergic rhinitis in mice by regulating Th1/Th2 balance
2023-08-07YaNanShiJinZhuSuJuanWangJiangQiaoGeng
Ya-Nan Shi, Jin-Zhu Su, Juan Wang, Jiang-Qiao Geng✉
1Department of Otolaryngology, Sanya Women and Children's Hospital, Sanya, 572000, China
2Department of Otolaryngology, Hebei Children’s Hospital, Shijiazhuang, 050031, China
ABSTRACT
Objective: To evaluate the effect of myricetin on ovalbumin (OVA)-induced allergic rhinitis in mice.
Methods: Mice were sensitized and challenged using OVA (5%,500 mL) intraperitoneally and intranasally, respectively, on an alternative day for 14 days, followed by administration of myricetin(50, 100, and 200 mg/kg) till day 21.Nasal symptoms, biochemical parameters, protein expressions, and histopathology were observed.
Results: OVA-induced increased nasal symptoms including rubbing,sneezing, and discharge were significantly reduced by myricetin (100 and 200 mg/kg) (P<0.05).Myricetin also protected against histamine challenge and attenuated elevated serum immunoglobulin E (IgE;total and OVA-specific), total IgG1, and β-hexosaminidase levels, as well as leukotriene C4 and interleukins levels in nasal lavage fluid(P<0.05).Western blot analysis showed that myricetin significantly upregulated the protein expression of T-box expressed in T cells,while downregulating the protein expression of GATA binding protein 3, NF-κB, and IκB-α (P<0.05).Additionally, OVA-induced histopathological abberations in the nasal mucosa was markedly ameliorated by myricetin treatment (P<0.05).
Conclusions: Myricetin exerts anti-allergic effects against OVAinduced allergic rhinitis via regulating Th1/Th2 balance.
KEYWORDS: Allergic rhinitis; GATA3; Interleukins; Myricetin;Montelukast; Ovalbumin; Th1/Th2 balance
1.Introduction
Allergic rhinitis (AR) is an allergic disease resulting in the inflammation of the nasal membranes.This inflammation is triggered seasonally or perennially in response to the allergens present in the environment[1].AR affects more than 500 million people worldwide,and this number has been increasing over the past two decades,possibly due to changing environmental factors, including increased allergen exposure[2].Symptoms of AR, including itching, respiratory obstruction, sneezing, rhinorrhoea, etc., severely affect the quality of life of patients across all ages, ethnicities, and countries, impacting their work, school, social life, and sleep[3].
Significance
Allergic rhinitis is an allergic disease resulting in the inflammation of the nasal membranes.Chronic exposure to protein allergens,including ovalbumin, causes the induction of allergic rhinitis symptoms.The current work reported the anti-allergic potential of myricetin against ovalbumin-induced allergic rhinitis in mice via Th1/Th2 balance.Therefore, myricetin can be explored as a possible alternative for allergic rhinitis management.
Environmental factors such as pet hair, mold, pollens, etc., and genetic factors such as gene polymorphisms influence allergic reactions by producing inflammatory mediators[4].Exposure to a plethora of allergens results in the activation of T helper type 2(Th2) cells, which further elevates the production of interleukins[5].Interleukins stimulate B-lymphocytes to produce immunoglobulin E (IgE), and binding of this IgE to the mast cell surface resulted in the secretion of histamine, prostaglandins, leukotrienes, and other mediators[6].The release of these mediators causes an increased inflammatory cell penetration, mucus and tear secretion, and vasodilation, which results in the symptoms of AR[7].
The mainstream therapeutic regimens for the management of AR include antihistaminic, topical corticosteroids, anti-allergens,decongestants, and immunotherapy[8].However, several adverse events are also associated with these drugs[9].Thus, for the effective management of AR, there is a need for emerging treatment options that may regulate the allergic reaction.Immunotherapeutic agents that are allergen-specific have been emerging as a potential desensitization therapy for AR[10].Traditional Chinese Medicines also contain potential therapeutic agents to treat AR, with some traditional healers already being utilized in polyherbal preparations to manage AR[11,12].As therapeutic moieties of herbal origin are relatively safer than synthetic treatment options, recent investigators prioritize their research on evaluating the anti-allergic potential of bioactive moieties of food origin[13].
Many animal models are available for AR, with murine models being the most useful for studying the immunology of the disease[14].Wei et al.investigated a mucosal immune response in an ovalbumin(OVA)-sensitized BALB/c mouse model of AR[15].The protein allergen OVA is systematically administered to cause sensitivity in the animal, followed by the intranasal administration of OVA resulting in the induction of AR symptoms[16].This occurs due to increased histamine and IgE levels, increasing inflammatory penetration[17].OVA-induced AR is the most widely used animal model as it is inexpensive, simple, and non-invasive[16].Furthermore,this model displays the characteristic pathological features that resemble clinical AR[16].
Flavonoids are one of the most common substances in many plants and plant-derived products that comprise our daily diet.Flavonoids have been researched for various diseases and disorders due to their antimicrobial, antioxidant, hepatoprotective, apoptotic, and analgesic properties[18].Furthermore, studies have also shown their antiallergic properties[19].The potential of morin, a flavonol, in AR has been previously demonstrated[20].Myricetin, another flavonoid, was also identified as the possible cause of the anti-allergic activity of bee pollen against OVA-induced allergy[21].The study suggested that the inhibition of mast cells, IgE and IgG1 production, and inflammatory markers (including interleukins, histamine, and tryptase) may be responsible for the anti-allergic potential of myricetin[21].Considering the abovementioned effects of myricetin, the aim of present study was to evaluate the effect of myricetin against OVAinduced AR in experimental mice.
2.Materials and methods
2.1.Animals
Male mice of strain BALB/c with weights ranging from 18-22 g were obtained from the Shanghai Children’s Medical Center animal house.They were maintained at standard conditions, including temperature: (24 ± 1) ℃, relative humidity: 45%-55%, and a light/dark cycle: 12:12 h throughout the experimental period.In addition,mice were provided with standard pellet chow and filtered water.
2.2.Ethical statement
The Institutional Animal Ethics Committee of the Shanghai Children’s Medical Center provided approval for the experimental protocol (approval number: 2021008720) and all the experimental steps were performed as per the National Institute of Health Guide for Care and Use of Laboratory Animals.
2.3.AR model establishment
Mice were sensitized on alternate days by administration of OVA(Grade V, Sigma-Aldrich Co., St Louis, MO, USA, 500 μL, 5%, i.p.)till day 14[22].Then they were randomly allocated into the following treatment groups (n=18 mice/group): AR control [received distilled water (10 mg/kg), orally], montelukast (10 mg/kg, orally), myricetin(purity ≥96%, Sigma-Aldrich Co., St Louis, MO, USA; 50, 100, 200 mg/kg, p.o.) and the groups received different treatments till day 21.A group of mice was maintained separately and received aluminum hydroxide i.p.without OVA followed by treatment with distilled water (10 mg/kg), and another group (per se) received myricetin (200 mg/kg).
The three different doses of myricetin (50, 100, 200 mg/kg)were selected based on previous studies[23-25], whereas a dose of montelukast (10 mg/kg, p.o.) was based on other previous studies[16,20].The body weight of mice was determined daily using electronic balance.Myricetin and montelukast solutions were prepared in distilled water daily and administered intraperitoneally from day 14 to 21 for biological evaluations.
2.4.Nasal symptoms in OVA-induced AR mice
On day 21, nasal symptoms were evaluated within 10 min after the OVA challenge[22].The number of sneezes and nasal itching motions(nasal rubbing) was recorded.The nasal discharge was scored as 0 =no discharge, 1 = the discharge reaches the anterior nasal aperture,2 = the discharge overshoots the anterior nasal aperture, and 3 = the discharge flows out.
2.5.Nasal symptoms during histamine-induced hypersensitivity in OVA-induced AR mice
To evaluate the effects on histamine-induced hypersensitivity after interruption of the drugs, mice were challenged with histamine dihydrochloride (10 μL per nostril of a solution of 1 μmol/mL in physiological saline) on day 24 of the study, and the number of nasal rubbing and sneezing were counted during 10 min period after challenge[22].
2.6.Blood sample collection from OVA-induced AR mice
On day 21, 2 h after the OVA challenge, blood specimens were collected from the retro-orbital plexus, and serum was obtained by centrifugation at 8 350 ×g for 10 min at 4 ℃.Samples were stored at-20 ℃ for biochemical and hematological measurements.
2.7.Collection of nasal lavage fluid (NLF)
NLF was collected using a previously described method[20].Mice underwent partial tracheotomy under deep anesthesia by intraperitoneal injection of 1% sodium pentobarbital (50 mg/kg).A 22-gauge catheter was inserted into the posterior naris from the opening of the trachea and along the direction of the nostrils.Sterile saline solution (3 mL) was perfused gently into the nasal cavities,lavage fluid was collected from the anterior naris, centrifuged at 220×g and 4 ℃ for 10 min, and the supernatant was stored at -20 ℃.
2.8.Biochemical measurement in serum of OVA-induced AR mice
Serum IgE (OVA-specific and total), β-hexosaminidase and IgG1,while IL-4, IL-5, IL-17, leukotriene C4 (LTC-4) and interferons(IFN)-γ in NLF were evaluated using respective mouse ELISA quantitation kit (Bethyl Laboratories Inc., Montgomery, TX, USA)as per manufacturer’s instructions.
2.9.Determination of histamine level in serum of OVAinduced AR mice
The histamine content of serum was measured by the o-phthaldialdehyde spectrofluorometric procedure.The fluorescent intensity was measured at 460 nm (excitation at 355 nm) using a spectrofluorometer, and histamine content was calculated[20].
2.10.Western blot assay
Mice were sacrificed by cervical dislocation, and spleen specimens (n=4) were collected, weighed using electronic balance and maintained at -70 ℃.Each tissue was sonicated in Tissue Protein Extraction Reagent (Thermo Fisher Scientific, Inc.).The lysates were centrifuged at 10 000 ×g for 10 min at 4 ℃.Protein concentration was determined using a Bicinchoninic Acid (BCA)assay kit (Beyotime Shanghai, China) on ice for 30 min.Equal amounts of extracted protein samples (50 μg) were separated by 10% sodium dodecyl sulfate-polyacrylamide gel electrophoresis and transferred onto polyvinylidene difluoride membranes.The membranes were blocked with 5% non-fat dry milk at 37 ℃ for 1 h and incubated overnight at 4 ℃ with the primary antibodies(Abcam, Cambridge, MA, USA): T-box expressed in T cells(T-bet; EPR27094-16; ab307193; 1:1 000), GATA binding protein 3 (GATA3; EPR16651; ab199428; 1:1 000), nuclear factor-kappa B(NF-κB; ab209795; 1:200), inhibitor kappa B-alpha (IκBα; ab97783;1:1 000) and glyceraldehyde-3-phosphate dehydrogenase (GAPDH;ab8245; 1:500).Anti-rabbit horseradish-linked IgG was used as the secondary antibody, which was incubated at 37 ℃ for 2 h.Protein bands were visualized using the Chemiluminescent kit (Bio-Rad Laboratories, Inc.), and GAPDH served as the loading control.
2.11.Histological examination
The nasal mucosa of 3 mice from each group was dissected and stored for 24 h in 10% formalin for histological examination.The specimens were dehydrated and placed in xylene for 1 h (3 times)and in ethyl alcohol (70%, 90%, and 100%) for 2 h, respectively.Infiltration and impregnation were carried out by treating with paraffin wax twice, each time for 1 h.For tissue slide preparation,specimens were cut into 3-5 μm thick sections and stained with hematoxylin and eosin (H&E).The specimens were mounted on slides using Distrene Phthalate Xylene (DPX).Sections were examined under a light microscope (Olympus DP71, DP-BSW Ver.03.03, Olympus Medical Systems India Private Limited, India)for histopathological features of the specimen and infiltration of cells in the epithelium and sub-epithelium.The intensity of histological aberrations in nasal tissue was graded as Grade 0 (not present);Grade 1 (minimal); Grade 2 (mild); Grade 3 (moderate); and Grade 4 (severe), as described in the literature[16,20].
2.12.Statistical analysis
The sample size was calculated based on the power analysis method considering 30% expected attrition using a formula: Corrected sample size = Sample size/ [1- (% attrition/100)][26].
Data analysis was conducted using GraphPad Prism 5.0 software(GraphPad, San Diego, CA) and reported as mean with standard error mean (SEM) and median with quartile range.A value of P<0.05 considered statistically significant.A post hoc analysis was conducted using Tukey’s multiple ranges (for parametric tests)and the Kruskal-Wallis, followed by Mann-Whitney’s multiple comparison tests (non-parametric tests) during one-way analysis of variance (ANOVA).
3.Results
3.1.Effect of myricetin on body weight and relative spleen weight
AR control mice had significantly higher relative spleen weight and lower body weight than normal mice on day 21 (P<0.05).Myricetin(100 and 200 mg/kg) treatment decreased the relative spleen weight and increased body weight markedly (P<0.05) compared with the AR control group on day 21.Treatment with myricetin (50 mg/kg)failed to induce any considerable changes (P>0.05) in relative spleen weight and body weight of AR mice.In addition, the per se group treated with 200 mg/kg myricetin did not show any alteration in spleen weight and body weight of mice (P>0.05) (Table 1).

Table 1.Effect of myricetin on body weight and relative spleen weight in OVA-induced allergic rhinitis in mice (n=6).
3.2.Effect of myricetin on nasal symptoms
AR control mice had higher incidences of sneezing and rubbing and a higher discharge score compared with normal mice on day 21 (P<0.05).Mice treated with myricetin (100 and 200 mg/kg)considerably (P<0.05) reduced the incidences of sneezing and rubbing and the discharge score compared with AR control mice on day 21.However, mice treated with myricetin (50 mg/kg) did not show any considerable changes (P>0.05) in the incidences of sneezing and rubbing, and discharge score.The incidence of nasal symptoms (sneezing and rubbing) in the per se group did not differ(P>0.05) from normal mice (Table 2).

Table 2.Effect of myricetin on OVA and histamine challenge induced nasal symptoms in mice (n=6).
3.3.Effect of myricetin on histamine-induced nasal hypersensitivity
The AR control group showed a considerably higher nasal hypersensitivity induced by histamine compared with the normal group (P<0.05), as evidenced by increased incidences of sneezing and rubbing after the histamine challenge on day 24.Treatment with myricetin (100 and 200 mg/kg) markedly alleviated histamineinduced nasal hypersensitivity in AR mice (P<0.05).The mice treated with myricetin (50 mg/kg) showed no significant differences from AR control mice (P>0.05) (Table 2).
3.4.Effect of myricetin on serum histamine, β-hexosaminidase,IgE, and IgG1 levels
The higher levels of histamine, β-hexosaminidase, IgE, and IgG1 in serum were noted in AR control mice than in normal mice (P<0.05).Myricetin (100 and 200 mg/kg) markedly decreased the levels of histamine, β-hexosaminidase, IgE, and IgG1 in serum of AR mice(P<0.05).However, AR mice treated with myricetin (50 mg/kg)showed no effective changes in serum histamine, β-hexosaminidase,IgE, and IgG1 levels (P>0.05) (Table 3).

Table 3.Effect of myricetin on serum biochemistry in AR mice (n=6).
3.5.Effect of myricetin on NLF IL-4, -5, -17, LTC-4 and IFN-γ levels
The AR control group had significantly higher IL-4, IL-5, IL-17, and LTC 4 levels and lower IFN-γ levels in the NLF compared with the normal group (P<0.05).Myricetin (100 and 200 mg/kg)significantly decreased the NLF levels of IL-4, IL-5, IL-17, and LTC 4 and increased IFN-γ levels in AR mice (P<0.05).The mice treated with myricetin (50 mg/kg) did not show any noticeable changes in IL-4, IL-5, IL-17, LTC-4, and IFN-γ levels in NLF (P>0.05) (Table 4).

Table 4.Effect of myricetin on OVA-induced alterations in ILs, LTC-4, and IFN-γ levels in nasal lavage fluid (n=6).
3.6.Effect of myricetin on spleenic T-bet, GATA3, IκBα, and NF-κB protein expressions
A marked up-regulation in the protein expressions of GATA3, IκBα,and NF-κB and a down-regulation of T-bet were noted in AR control mice (P<0.05).Myricetin (100 and 200 mg/kg) considerably downregulated the protein expressions of GATA3, IκBα, and NF-κB and up-regulated T-bet protein expression in the spleen of AR mice(P<0.05).However, myricetin (50 mg/kg) showed no significant changes in these protein expressions (P>0.05) (Figure 1).
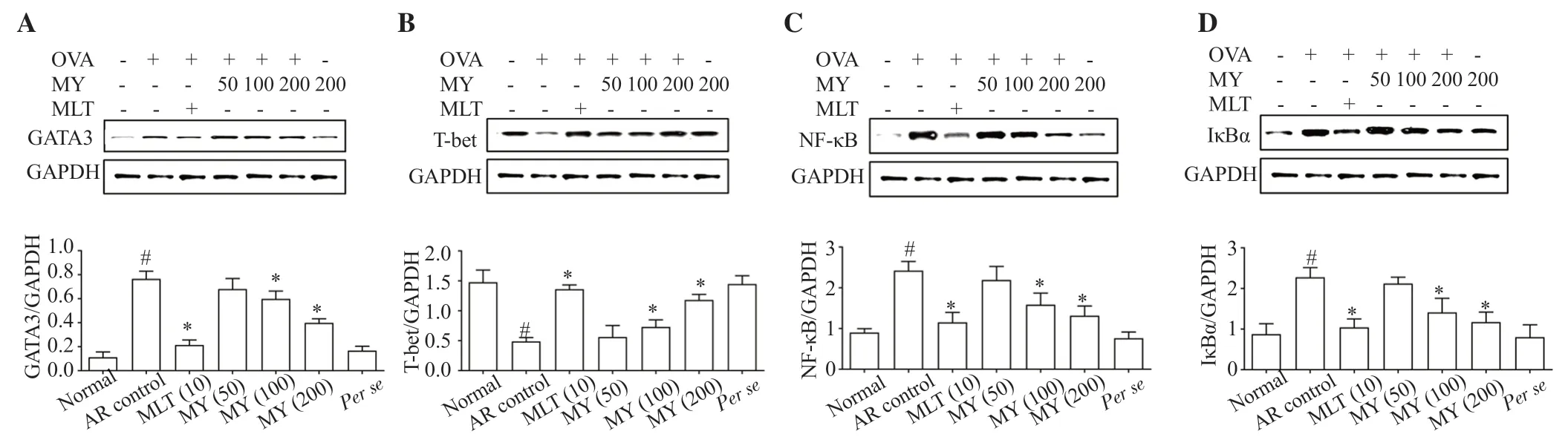
Figure 1.Effect of myricetin on spleenic GATA3 (A), T-bet (B), NF-κB (C), and IκBα (D) protein expression (n=6).The data are expressed as mean ± standard error mean (SEM) and analyzed by one-way ANOVA followed by Tukey’s post hoc test.#P<0.05 and *P<0.05 compared with the normal group and the AR control group, respectively.GATA-3: GATA binding protein 3; T-bet: T-box protein expressed in T cells; NF-κB: nuclear factor-kappa B; IκBα: inhibitor kappa B-alpha.
3.7.Effect of myricetin on histopathology of the nasal mucosa
The histological architecture of nasal mucosa from normal and per se mice showed well-organized capillary vessels, glands, and the lamina propria distributed abundantly without histological aberrations (Figure 2A and 2F).The nasal mucosa from AR control mice showed markedly increased eosinophil infiltration, hyperplasia,disturbance of mucosal epithelium, and edema compared with the normal group (Figure 2B).Treatment with myricetin (100 and 200 mg/kg) or montelukast alleviated hyperplasia, eosinophil infiltration,disturbance of mucosal epithelium, and edema (Figure 2C-2E).The mice treated with myricetin (50 mg/kg) did not significantly ameliorate the histopathological aberration induced by OVA in nasal mucosa (Table 5).
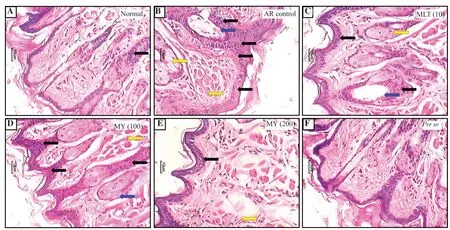
Figure 2.Effect of myricetin on nasal histopathology using hematoxylin and eosin staining (n=3).Eosinophil infiltration (black arrow), hyperplasia (blue arrow), and edema (yellow arrow).

Table 5.Effect of myricetin on nasal histopathology using hematoxylin and eosin staining (n=3).
4.Discussion
The results of the current investigation suggested a potential effect of myricetin against AR.Also, it was seen that the effect of myricetin on nasal symptoms, histopathology, protein expression,and biochemical levels was comparable to that of montelukast, a commonly prescribed medication in allergic diseases such as AR.AR produces a two-phasic reaction, an early phase characterized by the activation of mast cells that activates mediators such as cytokines, prostaglandins, histamine, etc., which finally results in AR symptoms[27].The late phase involves the accumulation ofinflammatory cells, such as neutrophils, basophils, eosinophils, etc.,in the nasal mucosa, this further promotes the histamine release and other proinflammatory cytokines, chemokines, etc., thereby sustaining the allergic response[28].Therefore, intraperitoneal and intranasal administration commonly uses a protein allergen to sensitize the mice[22,25].When challenged by the nasal route,these animals produced features of IgE-mediated allergic airway disease[22,25].
The induction of AR caused elevated levels of IgE titters in the serum, IL-4 levels in NLF, and inflammatory cell infiltration[29].Release of these mediators and inflammatory cell infiltration was reflected in the observation of characteristic pathology and symptoms(rubbing, sneezing, discharge, etc.) of AR.Furthermore, these nasal symptoms might also be mediated by leukotrienes, tryptase,prostaglandins, and histamine[1].In our study, myricetin significantly alleviated the nasal symptoms and decreased the histamine levels.These results confirmed myricetin also has a regulatory effect on histamine or other mediators of the nasal symptoms, i.e.,prostaglandins, leukotrienes, and tryptase.Histamine is important during inflammatory and allergic reactions that induces the nasal symptoms of AR[30].Therefore, many antihistaminic drugs, such as AR, are commonly used in allergic diseases[31].However, these drugs do not completely treat allergic reactions and have many adverse effects[31].In our study, myricetin decreased histamine release and produced a protective effect against histamine challenge.Myricetin also decreased the levels of β-hexosaminidase, an indicator used to identify the degree of activation of mast cells to release histamine.As higher levels of β-hexosaminidase indicate mast cell activation and histamine release, a decrease in β-hexosaminidase level is a sign of anti-allergic activity[32].Furthermore, as evidenced by histological findings, myricetin-treated mice had lower eosinophilic infiltration,edema, hyperplasia, and disturbance of mucosal epithelium.This suggests that myricetin also reduced the penetration of inflammatory cells to nasal mucosa and ameliorated inflammation.
A common characteristic of allergic reactions is the overproduction of IgE against the invasion of various allergens.In response to allergens, Th2 cells release Th2 cytokines, namely IL-4, IL-5, and IL-13, and cause B-cell differentiation into IgE by the interaction of cluster of differentiation 40 (CD40) with its ligand[28].Further exposure to the same antigen induces mast cells to release mediators responsible for allergic responses.LTC-4 as one of these mediators is responsible for irritation and sneezing[33].Therefore, IgE control is an important step in halting the release of these mediators.As seen in the results of the current study, myricetin might potentially have an IgE and LTC-4 suppressing capability, as myricetin reduced IgE and LTC-4 levels.Furthermore, the levels of Th2 cytokines were effectively reduced after myricetin treatment.Interleukins (IL-4, IL-5, IL-13) cause IgE secretion and play a role in the inflammatory response[34].IL-4 causes the Th cells to transform into Th-2 cells and inhibits the transformation to Th-1 cells[35].IL-5 is responsible for eosinophil production, while an increased level of IL-17 has been associated with aggravated AR[36,37].Furthermore, an increase in IFN-γ level was observed after treatment with myricetin in the present study.IFN-γ is released by natural killer cells and is an inhibitor of IgE production from B cells[38,39].These findings further suggest an anti-allergic activity of myricetin.
Myricetin also significantly decreased NF-κB and GATA3 and elevated T-bet levels.T-bet and GATA3 are transcription factors that have a major role in Th cell differentiation, T-bet is responsible for the differentiation to Th 1 while GATA-3 is responsible for the differentiation to Th-2[20].As increased Th-2 and decreased Th-1 cell responses are responsible for increased inflammatory response[40],the decreased expression of GATA-3 and the increased expression of T-bet suggested a beneficial effect of myricetin on AR.Furthermore,myricetin also decreased the expression of NF-κB, which is associated with inflammatory cytokine expression, and thus further prevented inflammation.
There is a need to identify new potential therapeutics for AR since the currently available therapy is inadequate and is linked to various adverse effects[9].Many herbal products are currently being studied for their potential effects on AR[41,42].For example, the potential of cinnamon bark in healthy men experiencing seasonal AR showed improved symptoms, regular daily activities, work productivity,and quality of life[42].Another study utilizing traditional Chinese medicine for treating AR showed improved symptom frequency and severity with minimal adverse effects[41].Furthermore, the results of several clinical trials evaluating the effects of flavonoids on AR reported a beneficial potential of flavonoids on the symptom scores of the participants, with no severe adverse effects reported[43].
Although these findings show the anti-allergic effect of myricetin,this study has limitations.Firstly, the mechanism underlying the interaction of myricetin with mast cells remains unclear.Secondly,more comprehensive scoring criteria and histological evaluation in this mouse model of AR are needed.Thirdly, immunohistochemical analysis of signaling pathway proteins in the nasal mucosa should be performed.Further investigation needs to be undertaken to evaluate these in-depth.
In conclusion, myricetin could exert an anti-allergic effect against OVA-induced AR in experimental mice via achieving Th1/Th2 balance by activation of Th1 response (increased IFN-γ levels and T-bet protein expression) and inhibition of Th2 response (decreased levels of IgE, histamine, β hexosaminidase and ILs, and reduced expressions of GATA3 and NF-κB).These results warrant further clinical investigation to develop myricetin as a potential therapeutic agent for AR.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Acknowledgments
We would like to express our gratitude to EditSprings (https://www.editsprings.cn) for the expert linguistic services provided.
Funding
The authors received no extramural funding for the study.
Authors’ contributions
YS: concept, design, literature search, data analysis, manuscript preparation, and review.JZS: concept, data acquisition, manuscript editing, and manuscript review.JW: literature search, data analysis,manuscript editing, and manuscript review.JQG: concept, design,data analysis, manuscript editing, and review.
杂志排行

Asian Pacific Journal of Tropical Biomedicine的其它文章
- Role of flaxseed (Linum usitatissimum L.) in disease prevention and treatment
- Characterization and antimicrobial, antioxidant, and anti-proliferative activities of green synthesized magnesium oxide nanoparticles with shoot extracts of Plicosepalus curviflorus
- Cryptotanshinone ameliorates cladribine-induced cognitive impairment in rats
- Epigallocatechin-3-gallate exerts antihypertensive effects and improves endothelial function in spontaneously hypertensive rats